The author has presented “Objective analysis of the case: 20 points recipe: A blueprint to use homeopathic philosophy and Organon in clinical practice”. The following case is an illustration of his analytical method of data processing. The readers are requested to read the original article published in this same issue of Hpathy’s journal.
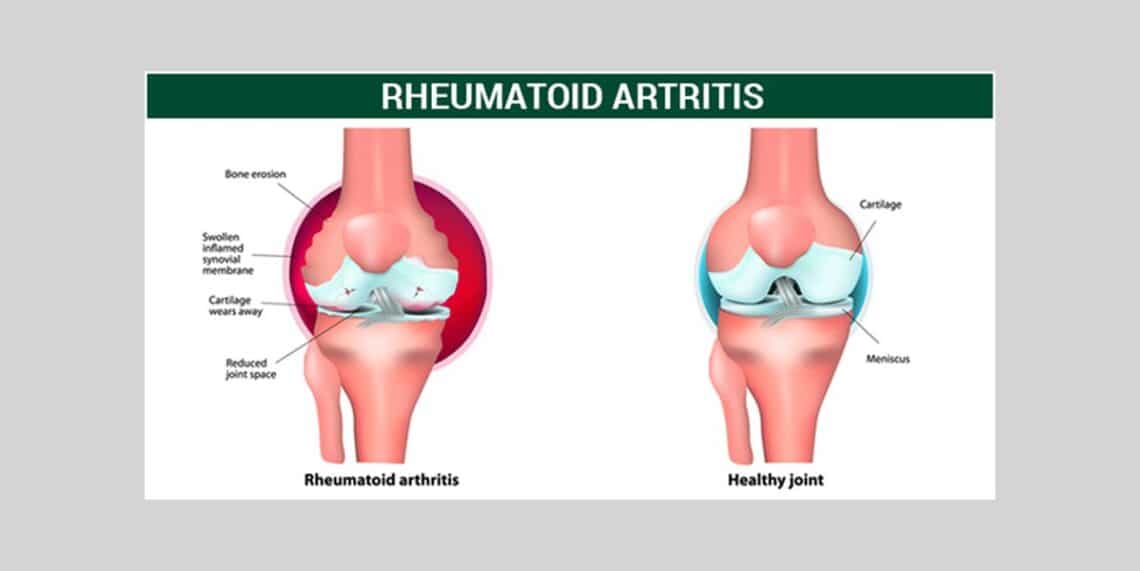
Mrs. E.D. 38 year old female. A case of Rheumatoid arthritis diagnosed three years ago.
CHIEF COMPLAINTS
Pain in joints, with swelling and stiffness since four years. It started simultaneously from both wrists, then elbows, shoulders, fingers, knees, ankles etc. Pain, swelling, stiffness < late in afternoon, night, evening 3 < < 5 to 11p.m.3
Pains: Appear gradually, sometimes dull or sharp; > by warm application. < initial motion3, > continued motion3, < descending the stairs3. < standing2.
Wandering pains, go on shifting to different joints. Constant pain in toes when walking. More pain in wrists and fingers.
Stiffness of joints, < morning, first motion.
Varicose veins since 10 years, more on the left side. Visible varicosis. Itching and burning; there is a big network of varicose veins above knees. Heaviness and pain < standing
PATIENT AS A PERSON
Perspiration: Palms and soles < anxiety.
Thermal: I don`t tolerate winter. I never did like winter. C3H2.
Sleep: Normal. Dreams: Rare. No frequent dreams.
Food <: Chocolate and eggs cause eruptions, itching, more in folds of arms.
PAST HISTORY
Tonsillitis with pus; no tonsillectomy done. During tonsillitis, high fever, pain; once admitted in a hospital as left tonsil was extremely swollen and septic.
Steroids, non-steroidal anti-inflammatory drugs and methotrexate many times.
FAMILY HISTORY
Mo- Rheumatoid arthritis, goitre, heart problem
Father- Lumbar spondylosis
MG2F- Ca colon
EXAMINATION
Rheumatic nodule left palm, right dorsum of leg; synovitis.
Left small toe deformity.
LIFE SPACE
Middle class family. I live with my husband, M-I-L, a daughter and a dog.
Childhood: I had difficult childhood.
Father: I had hatred feelings towards my father. He was dictatorial, and used to insist that I must come early at home. When I was 20 years, parents separated. My father started to take alcohol, drinking even till today; he is addicted or not, I don`t know. I saw quarrels during my childhood and nothing else. They continue even today; I usually took side of my mother. I used to protect her. Father used to torture her, not physically but mentally; he used to be abusive. I do not want to follow my father. He had extramarital relations. He didn’t get married after he left my mother and at the moment, he is living alone. I am angry and excitable by nature. I am very anxious. I become restless3, panic3, impatient3.
Mother: Cheerful, singing songs, easily angered and easily calmed down; more problems with health; she was more suppressed and depressed.
Sister: She lives nearby. My father loved my sister more than me. He told me directly, ‘I love your sister more’. I remember this sentence. Sister sustained burn injuries and about to die, then parents started paying more attention to her. I was 11 years old and she was 4 years when she had burn injuries in the kitchen. I don`t have jealousy against my sister.
Current family: M-I-L is manipulative. She tries to cry. If someone cries, I feel pity; but she can`t manipulate me; we live together since 10 years. I do things directly. I am independent in action.
Husband: Different from me; settled, calm and slow. Temperament different; he may be angry for time to time. We discuss things. I don`t think he dictates.
Daughter: 13 years, suffers from tonsillitis.
Job: Since the last 2 years, I am managing a coffee shop. I am doing everything at the job, prepare types of coffee, serve people, clean, keep account etc. It’s a satisfactory job. Before 2 years, I was at another shop, I was a managing director. Some conflicts with the boss and I left the job. Sometimes I am too direct in communication. I can hurt others and be rough. I like to be the leader and to take charge of the situation. When rheumatic pains are worse, I can cry. I feel helpless and angry; < consolation; I never accept any consolation in such moments.
Bursting: I get easily angered but soon get cooled myself.
Body language when angry: Screaming; eyes big; movements of hands; throws things away but will not hit the daughter; will bang the door loudly. Husband and daughter know this well. Anger sometimes uncontrollable; abusive – then I feel guilty; but I don’t like to say sorry. Anger can be expressed on any person.
(Observations during interview: Power play of pointing a finger and making a fist several times during interview. ) I don`t like to be dependent and helpless. I don`t like to postpone something, or I don’t need help from others. I do the things fast and I hate slowness.
Hobbies: Dancing; folk dances. Fast dances.3.
ANALYSIS OF THE COMPLAINTS ACCORDING TO TWENTY POINTS RECIPE
(The bold points refer to the case)
- Nature of disease:
- Acute/Per acute/ acute on chronic (exacerbation). Sub-acute. Chronic/ Remission. Mixed / Messed: natural + iatrogenic. Psycho-somatic mixed. Somato-psychic mixed. Psychiatric. Auto-immune. Clinical diagnosis: Rheumatoid arthritis.
- Phase of the Disease
- Pre/Sub-clinical. Clinical. Functional. Structural. Fully developed. Inadequately developed.
- Affinity
- Cells/ Tissues / Organs/ Systems/Sides (extension, syndrome shifting etc.).
Systemic illness affecting musculo-skeletal system. Veins.
- Type of Pathology
- Atrophic / Emaciation / Shrivelled / Apoptosis. Benign. Degenerative. Destructive. Dysplasia / Proliferation. Hyperplasia / Metaplasia / Hypertrophy. Induration / Hardening. Inflammation (serous, fibrinous, catarrhal, eosinophilic, granulomatous, pyo-granulomatous, fibronecrotic, lymphocytic, suppurative). Malignant. Embolic. Thrombotic. Caries/Necrosis/Sclerosis. Nodular. Ulceration. Hemorrhagic. Ischemic. Venous. Calcareous. Fibrotic. Rheumatic. Excess/Deficiency.
- Investigations: RA test positive. ESR: 64 mm at the end of one hour. Hb – 8.8 gm%
ASO Titre: 178 units. C-Reactive proteins: Positive.
- State of pathology: Borderline. Irreversible. Reversible.
- Pattern of response
- Alternating. Changing. Continuous. Erratic. Regular. Irregular. Paroxysmal. Periodic. Lingering. Shifting. Progressive. Recurrent. Static.
- Pace of disease:
- Slow. First rapid then slow. First slow then rapid. Moderately rapid.
Moderately slow.
- Expressions: (+ = scanty, ++ = moderate, +++ = ample)
- The field of modalities: General+ Particular ++
- The field of sensations: General+ Particular ++
- The field of symptoms: Pathognomonic ++ Non-pathognomonic +
- Common ++ Characteristics +
- Miasmatic diagnosis:
- Dominant / Active: Sycotic
- Fundamental: Syphilis
- Combined/Complex: Syco-syphilitic
-
-
- Sensitivity: High. Moderate. Decreased. Mind – Increased. Nerves (Body) – Increased.
- Susceptibility: High. Moderate. Decreased.
- Suppression: Mind: + Physical: +
- General vitality: Good. Moderate. Low.
- Monogram; Pathological Generals. Intertwining threads that run through and through. The consistent behavior of tissues or system.
- Allergic. Venous. Sclerotic.
- Dispositions: Temperamental /Personality traits
-
Independent. Decisive. Angry. Excitable. Impatient. Ego response –
Hypertrophic.
-
-
- Body Language: Totality of all elements of body language for the sake of perceiving the pattern . The clusters that the patient displayed more often: Aggressive. Dominant. Open. Power. The patient was in ‘up’ position throughout.
-
-
- Defense mechanisms: Idealization-devaluation. Undoing. Acting out.
- Themes:
- With auto-immune process, defining ‘auto’ is important.
- Inflammation denotes fight and we have to define the ‘fight’ in the patient.
- Varicose veins indicate stasis, stasis of deoxygenated blood; keeping unwanted in the veins and not able to eliminate; gravitational pull.
- The system is active. The patient doesn’t like slowness. She does the things in a fast way. The rheumatoid arthritis prohibits the activity and makes the system slow. Stasis also denotes the theme of slowness.
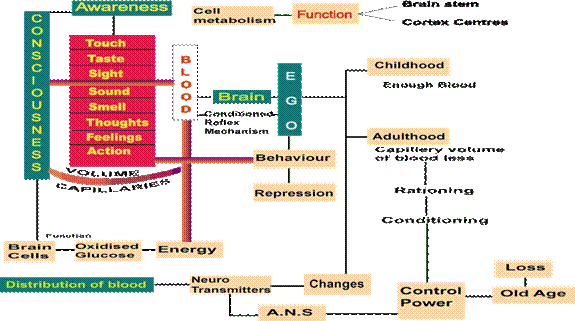
- Blood and Ego
- Repertorization
- Rubrics: Essential/crucial/determining characters
- Posology
- Selection of potency based on nine fundamental concepts
- The schedule of repetition versus individualization
- Follow up
ANALYSIS OF THE LIFE SPACE
The role of mind in auto-immune diseases can’t but be emphasized. The latest discoveries in brain-immune interactions and the brain stress response in autoimmune diseases including rheumatoid arthritis, underscore the role of mind. A blunting of the brain hormonal stress response is also an important contributor to development of autoimmune diseases. The reason is that cortisol, the potent anti-inflammatory hormone that is released from the adrenal glands in response to stress, is also released after exposure to inflammatory triggers.
In normal circumstances cortisol keeps the immune system in check, preventing inflammation from going out of control. In many patients with autoimmune diseases, this cortisol response and the cascade of brain hormones that stimulates its release are impaired, so there is no shutoff valve to end inflammation when it is no longer needed. In other patients, the cortisol response may be intact but immune cells are resistant to the anti-inflammatory effects of cortisol due to abnormalities in the cortisol receptor. In both circumstances, inflammation goes on unchecked without the dampening effect of the body’s own cortisol.
There is a strong miasmatic load in this case and mother’s rheumatoid arthritis is a major direct transmission to develop the rheumatic dyscresia. We have to see the life space of the patient on the background of transmitted material.
The painful childhood experience is a major issue to build upon a decisive personality. She has enough say of her own to go ahead in her way. There is a definite lack of affection from father but the patient doesn’t harbor any abandoned feeling out of the sensitive phases of childhood and adolescence. She is independent and wants to be a leader. She can cut off the relations and the theme of life is not to invest emotions in other persons. If the things don’t agree with her, she will find her own way. She can’t tolerate the domination.
It is typical for her to be easily angry; she will speak out. She can be abusive and rough with others and then she may feel some kind of self-reproach but it is not important because she will not apologize for it. She doesn’t want to be helpless and she has an illness of RA that makes the sufferer helpless.
REPERTORIZATION
Rubrics –
- Extremities, pain, motion, beginning of motion, agg.
- Extremities, pain, motion, continued motion, amel.
- Extremities, pain, < evening
- Varicose veins
- Generals, food and drinks, chocolate agg.
- Generals, food and drinks, < eggs, agg.
- Mind, Anger, easily
- Impatience
Filter
Puls – 7/17, Lycopodium – 6/14, Calc – 6/10, Ruta – 6/7, Rhus-t 5/12, Ferr- 5/11, Sep 5/8, Dulca 5/7, Ign 5/7, Nat-mur 5/7, Psor- 5/7, Sulph 4/8, Ars 4/7, Plb-met 4/7, Sil 4/7
SELECTION OF REMEDIES
CHRONIC CONSTITUTIONAL REMEDY: DISCUSSION
Repertorization yields many remedies of acute and chronic dimensions. Puls and Calc rank high but fall short in essence. Both Puls and Calc are yielding, dependent and wants support and protection. Ruta is also ranking high as it covers modalities; mentally Ruta patient is very dissatisfied, suspicious and has weeping disposition. Sep is chilly and has varicose veins. Sep is independent too. But she is not Sep because she has neither stifled emotions nor has she become indifferent towards anybody. Her work speed is fast and moreover, she wants to work as a leader than to take a back seat of withdrawal through apathetic response as of Sep. Dulc matches many aspects viz. domineering, strong-minded and possessiveness. These three aspects of Dulc are chiefly available in family and not outside. In work area, Dulc is more confused. Dulc can be abusive and quarrelsome but without being angry. Soft, gentle and vulnerable Ign can’t be thought of as a constitutional remedy for this case though it appears in repertorization chart. Nat-mur is known to possess antipathic and hatred response towards father in a chronic way. But Nat-mur becomes melancholic and isolated and there is much more personal aggrandizement of sufferings. Our patient lacks the emotional investment that Nat-mur literally pours in others. Sulph comes more as a quantity than quality in repertorization, though bursting out and detachment are typical for Sulph. Plb-m is a good idea in this case in view of early sclerosis in bones and rheumatic diathesis. But Plb-m is much more selfish, egoistic and becomes increasingly slow and apathetic in evolution. I often term Plb-m as syphilitic Calc.
Ferr and Lyc are the best choices in this case and they need discrimination. Ferr has domineering disposition (like Lyc) but has no power of love. Lyc is more manipulative and boaster. Ferr never feels let down. Both are performance oriented. ‘Strike when the iron is hot” is more of Lyc. Ferr is more excitable, impatient, easily angered and sensitive than Lyc. Ferr is allergic too; rather the entry point for Ferr in this case is < from eggs. Ferrum is in motion always (like blood in circulation). Varicose veins as pathological concomitant of rheumatic diathesis is a point in favour of Ferr.
Ferrum-met is selected as a chronic constitutional remedy.
POSOLOGY
We have to see that patient’s age is 38 years and within a span of 3 years, there is a small toe deformity. X-ray has revealed sclerosis and hence, I have categorized the pace of the disease as moderately rapid and pattern of response as progressive. The chronic inflammatory response is of destructive type. Even though mind sensitivity is high and there is a qualified mental state, in view of stepped-in pathology and the remedy’s action should reach at the tissue level, it was decided to begin with LM scale.
REPETITION SCHEDULE: SOME COMMENTS
Fer-m LM1 to be given daily one dose at bedtime for 10 days. Then a gap of 10 days. Then again Fer-m once per day for 10 days. This schedule to be continued for 3 months. I have found this type of schedule extremely useful in many cases.
This method has many advantages.
- You can gradually increase the potencies as per assessment of follow up.
- There is no fear of aggravation.
- You give a remedy consecutively for 10 days so that the action gets explored fully over the system.
- Within 10 days gap of no medicine, the system tries to adapt to the already administered doses.
- You have on one hand, potential remedy’s action being harped on the system for reaching at cellular level through adequate registration, and on the other hand, you allow the system to evoke its response.
- At the end of follow up, say, after 2 or 3 months, you are in a better position to assess clearly; there is no confusion if the remedy has acted or not.
- With this method, I suggest to go to higher scale after the improvement has come to halt. My clinical experience is that if you don’t give the ascending scale, the remedy stops its action.
Of course, this method can’t be and shouldn’t be followed in all cases. If you follow in all cases, you are not following the principle of individualization. In advanced pathological cases, it has more scope. Further in cases where vitality is low, pathology is advanced, susceptibility is poor and there is a fear of killer aggravation, this method has a great scope.
DIET FOR AUTO-IMMUNE DISORDERS
Suggestions
- Eat frequently.
- Eat a diet rich in carbohydrates in the form of whole grains, fruits and vegetables. This type of diet will lessen inflammation in the body and promote healthy immune functioning.
- Eat antioxidant foods, including fruits (such as blueberries, cherries, and tomatoes), and vegetables (such as squash and bell peppers).
- Avoid refined foods such as white breads, pastas, and especially sugar.
- Reduce salt.
- Eat beans for protein.
- Use healthy oils, such as olive oil or vegetable oil.
- Reduce or eliminate trans-fatty acids, found in commercially baked goods such as cookies, crackers, cakes, French fries, onion rings, donuts, processed foods, and margarine.
- Avoid caffeine and other stimulants, alcohol, and tobacco.
- Drink 6 – 8 glasses of filtered water daily.
- Exercise at least 30 minutes daily, five days a week.
- Omega-3 fatty acids
- Probiotic supplement (containing Lactobacillus acidophilus), 5 – 10 billion CFUs (colony forming units) a day. Probiotics, or “friendly” bacteria, can help maintain gastrointestinal health.
- Vitamin E helps prevent the tissue hardening. Both the essential fatty acids and vitamin E are helpful for all autoimmune disorders.
- Calcium and silica are minerals needed for bone tissue.
- Vitamin C (with bioflavonoids) act against inflammatory process and is needed for the health of the connective tissues.
- Take magnesium and zincum more through natural diet.
Take following diet
- Mostly Organic Vegetables: including anise, artichoke, asparagus, beets, bok choy, broccoli, cabbage, carrots, cauliflower, celery, chives, cucumbers, garlic, kale, kohlrabi, leeks, lettuce, mustard greens, onions, parsley, radishes, rhubarb, shallots, spinach, squash, sweet potatoes, water chestnuts, watercress, yams, zucchini, including kimchi, kombucha tea, pickled ginger, sauerkraut, unsweetened coconut yogurt. You must make your own or buy one of the few brands that are genuinely fermented (not made with vinegar) and free of sugars or additives.
- Low Glycemic Organic Fruits: including apples, apricots, avocados, berries, cherries, grapefruit, lemons, oranges, peaches, pears, plums.
- Coconut: including coconut butter, coconut cream, coconut milk, coconut oil, unsweetened coconut flakes, unsweetened coconut yogurt.
- Noodles: brown shirataki yam noodles (sold in Asian grocery stores). Avoid the noodles that also contain tofu.
- Herbs and Spices: including basil, black pepper, cilantro, coriander, cumin, garlic, ginger, lemongrass, mint, oregano, parsley, rosemary, sage, sea salt, thyme.
- Other: apple cider vinegar, herbal teas, olive oil, olives.
Foods to be avoided
- Sugars: including agave, candy, chocolate, corn syrup, fructose, high fructose corn syrup, honey, maple syrup, molasses, sucrose.
- High Glycemic Fruits: including bananas, canned fruits, dried fruits, mango, pineapple, raisins, watermelon.
- Grains: including amaranth, barley, buckwheat, bulgur, corn, couscous, kamut, millet, oats, quinoa, rice, rye, spelt, wheat, wheat germ.
- Nuts and Seeds: including almonds, peanuts, sunflower seeds, sesame seeds.
- Gluten-Containing Compounds: including barbecue sauce, binders, bouillon, brewer’s yeast, cold cuts, condiments, emulsifiers, fillers, chewing gum, hot dogs, hydrolyzed plant and vegetable protein, ketchup, soy sauce, lunch meats, malt and malt flavoring, malt vinegar, matzo, modified food starch, monosodium glutamate, nondairy creamer, processed salad dressings, seitan, some spice mixtures, stabilizers, teriyaki sauce, textured vegetable protein.
- Dairy Products and Eggs: including butter, cheeses, cow milk, creams, frozen desserts, goat, milk, margarine, mayonnaise, sheep milk, whey, yogurt (except coconut).
- Soy: including edamame, miso, soy milk, soy protein, soy sauce, tempeh, tofu.
- Fungi: edible fungi and mushrooms.
- Alcohol: all alcohol.
- Beans and Legumes: including black beans, lentils, peanuts, peas, pinto beans, soybeans.
- Nightshade Foods: including eggplant, paprika, peppers, potatoes, Tabasco® sauce, tomatillos, tomatoes.
- Other: canned foods, coffee, processed foods.
PROGRESS NOTES
26/9/2006
Ferrum-met, LM1 one dose daily at bedtime for 10 days and then a gap of 10 days.
Follow-up 3/1/2007
I am definitely feeling better. The pains have reduced and there is less morning stiffness. I feel more energetic when I am on 10 days of medication. The last 10 days, however, are not useful- my pains become stronger and my mood is not good.
Ferrum met LM2 with the same schedule of 10 days medication and 10 days gap for 3 months.
10/3/2007
Soon after your remedy, I started feeling better. The pain in joints is less and I don’t feel heavy as before. Swelling is less. I think I have less explosion of anger.
Continue with Ferrum met LM2 with the same schedule.
15/6/2007
I was better but since couple of days I have severe pain in knees, elbows and toes. My back is also aching badly and it is difficult to find the right position for sleep.
A dose of Carcinocin 1M was interpolated due to family history of cancer. Then a gap of of 10 days. Continue with Ferrum met LM2 with the same schedule.
22/9/2007
I think mentally I am better. I take the things lightly and don’t react strongly. I wanted leave for some days but my boss refused but I didn’t react and I didn’t take it to my heart. As far as pains are concerned, there is no change and no deterioration also. Morning stiffness is for 10-15 minutes and my knees hurt while ascending the stairs.
Ferrum met LM3 with the same schedule of 10 days medication and 10 days break.
22th Dec. 2007
I am feeling better, no swelling, no strong pains, at the beginning there was <. Now I am able to open the fingers.
I can say the following – 50% > with LM1 for your first set of treatment. With LM2 – just > temporarily but no further improvement. With LM3, I feel good improvement.
General amelioration of the complaints. Swelling of the joints, stiffness, and pain – all three are relieved.
I have changed a lot – I became calm. Before the remedy I was exploding like a bomb, then I was weeping for many days. My irritability has been >. I had only two episodes of anger explosion but I calmed down quickly.
One week ago, for 10 days, I had strong pain in right forehead, extending to occiput. First time headache in the life. But now it is okay. I don’t know the cause, may be stress related. But I am not sure. Pain was for the whole day, spotty.
Eggs and chocolate < has stopped. I am happy that with your medicines I can consume eggs and chocolate.
Varicose veins – same. But they are not painful.
Ferrum met LM3 with the schedule of 10 days remedy and 10 days break.
Investigations: Hb 10.5 gms%. RA test: Positive. ESR: 36 mm/hr
19/4/2009
Last 2 years the patient has not seen me. She told me that you are just increasing the potency of Ferrum met when I have more complaints. I decided not to meet you and I took Ferrum-met L4, L5 and L6. In your way of 10 days of medicine cycle and 10 days of break. Overall I am better than what I was before 2007.
But now there is some crisis. New small nodules have appeared within the last 3 months on right hand. Morning stiffness for 30 to 60 minutes. Veins of legs are more painful; of course my standing at the job is now for the whole day. I removed two workers in my cafe as they were working less and chatting more. Now I do all work single handedly. Anger is less. I am calmer than before. Menstrual cycle is normal. I became more chilly this strong winter. Has put on more weight.
Last crisis was > with Ferr-met LM6. But now it is not helping.
Pains –sharp and strong at different places.
I interpreted this data in two ways. Not meeting me and taking further ascending doses by her own discretion is due to her independent disposition and secondly Ferrum met LM6 has stopped its action. I explained her how follow up from a doctor is essential and she should not act as a doctor!
DILEMMA FOR A PHYSICIAN
- What should I do?
- Ascending scale of Ferrum met in LM?
- Ferrum met in centesimal scale?
- Change of remedy?
- Use of an intercurrent? Which intercurrent? A nosode or any other?
I decided to follow a different method.
- Ferrum–met LM7 BD x 3 months without break and
- Plumbum-met 200 monthly one dose for 3 months.
The reasons to give Plb-met: to stimulate the vitality both at systemic and local level, to check the auto-immune process (and sclerosis has stepped in) and to give a deeper-acting remedy in complementary relationship. Nosodes are not the only intercurrents. Note that Plb-met is also listed under ‘Lack of reaction’ for 3 marks. I think that the remedies covering ‘lack of reaction’ should be thought of for intercurrent prescribing.
9/11/2009
No crisis within 6 months. Nodules have disappeared. Swelling is less. Pain in feet. Itching spot over ankles. I have pains but they are bearable. Overall I am better. There is no deterioration. I work hard and my energy status is good. Morning stiffness is definitely less. I travelled a lot at many places in Europe and didn’t notice any crisis. I enjoyed the vacation.
I suggested continuing the same schedule for 3 months.
2/4/2010
I am fine; my arthritis is coming and going. But I must say that I am much better. There are no crises as before and my daily activities are not hampered. I did tests: RA is weakly positive. Hb 11.3 gms%. ESR: 32 mm/hr. I could not meet you because when you came in our country, I was traveling with my family. But I continued your recommended recipe. I am taking Plb-met 200 once every month and only last month, I started taking Ferrum met LM8 daily two doses as per recommendation on Skype.
Varicose veins are on both legs, more on 1eft, but they are not painful; occasional itching. Over the years, with your treatment, there is > in varicose veins and no new varicose veins. Morning stiffness is there though less and I have shoulder pains in morning.No eruptions from eggs and chocolate.My daughter, 16 years of age, had stroke in Jan 2012. Now she is 90% better. She is a high school student. She had right hemiplegia. I blamed myself for her stroke. I took her to a doctor, who told me that she is okay. Everybody helped. Husband and me went together with all this experience. I was asking constantly why this happened. At first fear, what will happen to my daughter and then anger against the doctor who couldn’t diagnose and prevent.
Joint pains worsened during this phase. I know that I am strong and I have to fight.
Overall, I am better and my arthritis is well under control.



It was an amazingly presented case, which gave a precise learning about how to deal with a difficult case.
I learnt following lessons from this case.
1. The direction to collect the components of patient’s information
2. The importance of a well-taken case, which is the cornerstone of homoeopathic practice
3.Then the analysis of the data through 20 points gives a clear picture as to the integrated homoeopathic approach.
4. Differential diagnosis of the remedies and final selection of Ferrum metallicum is a deep thinking process
5. Selection of potency and reasoning of LM scale make this case study par excellence.
6. In the follow up of the case, while the patient was getting relief the patient knowing the prescription leaves the doctor and engages in self-
prescription. This was a great twist in the curative process of the patient, we all doctors face this problem by revealing the drug name to the
patient and how to handle this situation also is aptly explained.
We as students and practitioners actually need such thoroughly worked out cases to read, learn and understand the logical reasoning behind
each step.
Thank you Ajit sir for guiding the needy like me through your integrated case presentation.
Dr. Sonia Hemnani
Dear dr,
i think that so many food items do or do not eat is too much. more over it gives an impression that homeopathy is meant for rich men. the choice of remedy and determination of dr is trust worthy.
thanks