 Gastritis is the most common silent disease of the gastrointestinal tract, affecting more than half of the world population. It is well known that H.pylori is the chief etiological agent of chronic gastritis, peptic ulcer, gastric adenocarcinoma, malt lymphoma. Helicobacter pylorus was discovered by Warren and Marshal in 1983. H. pylori has some unique characteristics:
Gastritis is the most common silent disease of the gastrointestinal tract, affecting more than half of the world population. It is well known that H.pylori is the chief etiological agent of chronic gastritis, peptic ulcer, gastric adenocarcinoma, malt lymphoma. Helicobacter pylorus was discovered by Warren and Marshal in 1983. H. pylori has some unique characteristics:
- It defied its detection by scientists for centuries.
- It survives in the stomach, an organ which is devised by the nature to kill all bacteria.
- 85% of the population hosts this organism asymptomatically.
- It persists in the gastric mucosa for decades.
- It does not penetrate the gastric mucosa for decades.
- It reduces the risk of oesophagitis, Barrett’s esophagus, esophageal adenocarcinoma, in the infected individual.
Gastritis is defined as an inflammatory response of the gastric mucosa to infections or irritants.
In the histology of normal gastric mucosa, inflammatory cells – neutrophils are spare and lymphoid tissue is absent.
ACUTE GASTRITIS is diagnosed endoscopically in the presence of hyperemia, intermucosal hemorrhages, and erosions in the gastric antrum and/or body mucosa.
Erosions are flat, or elevated white based lesions with an erythematous margin, and are frequently seen in the antrum.
Histology shows marked surface epithelial degeneration and heavy infiltration with neutrophils, but it is rarely performed.
CHRONIC GASTRITIS may be classified as chronic active, non-atrophic (superficial), atrophic and pernicious anaemia.
On histology of the gastric mucosa, there is a predominant increase in the chronic inflammatory cells – lymphocytes, plasma cells and an occasional lymphoid follicle may be present.
Presence of numerous neutrophils indicates activity (chronic active gastritis).
In CHRONIC NON – ATROPHIC GASTRITIS inflammatory cells are restricted to upper one third and glandular atrophy is absent
In CHRONIC ATROPHIC GASTRITIS, infiltration extends much deeper and glandular atrophy (mild, moderate, marked) is present.
Gastric Atrophy, is diagnosed in the absence of inflammatory cells and extensive glandular damage is present(pernicious anaemia)
Endoscopy in the patients with advanced atrophic gastritis shows thinning of mucosa (loss of folds) and prominence of sub mucosal vascular patterns.
Atrophy is defined as the loss of appropriate glands and may be with or without intestinal metaplasia.
With atrophic gastritis, metaplastic changes in the glands – pseudo pyloric in the body mucosa or fundus – may be observed, fundus is inappropriate for location.
Metaplastic changes in the epithelium, intestinal in the antrum, body, fundus inappropriate for location, may be observed.
Intestinal metaplasia may be patchy and most frequently found in the gastric mucosal biopsy from the lesser curvature, near the incisura angularis.
Intestinal metaplasia extends proximately with increasing age and severity of ch. Gastritis.
INTESTINAL METAPLASIA may be complete –
Type I (enteric): Small intestinal epithelium with microvilli, goblet cells with acidic mucin, paneth cells at the base or incomplete.
Type II (entrocolic): Goblet cell with sulphomucin it is closely linked to the intestinal type of gastric adenocarcinoma, as the genetic abnormalities noted in pt with dysplasia (intraepithelial neoplasia) is observed in them.
Type III( colonic): Goblet cell with sulfomucin it is closely linked to the intestinal Types of gastric adenocarcinoma, as the genetic abnormalities noted in the pt with dysplasia (intraepithelial neoplasia) are observed in them.
Pernicious anaemia is defined as severe vita B12 malabsorption due to a marked intrinsic factor deficiency (‹ 200 units/hr) following a maximal stimulus.
A new definition of pernicious anaemia – the presence of intrinsic factor antibody in the serum or gastric juice with vita B12 malabsorption due to intrinsic factor deficiency was suggested in 1968.
Pt. of ‘pernicious anaemia’ without IFA should be accurately classified as atrophic gastritis, as the essential genetic factor the IFA, is absent in them.
Gastropathy should be differentiated from chronic gastritis by the absence of significant inflammation and the presence of vascular abnormalities.
ACUTE GASTRITIS
Damage to the gastric mucosa due to –
Medication – Aspirin, or non steroidal anti inflammatory drug (NSAID), cytotoxic drug, iron.
Irritants – Red and green chili, tobacco ingestion, alcohol.
Infections – Bacterial, viral, or fungal.
Uremia
Stress
Etiological factors for acute gastritis vary in developed and developing countries
In developed countries, drugs like Aspirin to prevent arterial thrombosis or NSAID for relief of the pain of arthritis are widely consumed by elderly and the commonest cause of acute gastritis.
Drug induced mucosal damage is predominantly in the antrum.
In acute gastritis, the gastric mucosa is intensely congested both in the body and antrum. The mucosal biopsy shows degenerative changes in the surface epithelium with mucus depletion and heavy infiltration with neutrophils.
Acute gastritis is characterized by sudden onset and quick resolution, at times within 3-4 days. To diagnose erosions, as the cause of haematemesis, gastroduodenoscopy examination should be performed within 48 hrs. In humans, the surface epithelium cells of the gastric mucosa are continuously exfoliated and replaced every 2-4 days – approximately half a million cells are exfoliated every minute and the same number replaced. Erosion occurs when there is an imbalance between the damage and repair of the surface epithelial cells. The deoxyribonucleic acid (DNA) content of the nuclei of the cells of different tissues is nearly identical. The number of the cells and the number of nuclei exfoliated during a period of time can be estimated by measuring the DNA content in the gastric juice. When the gastric mucosa is exposed to irritants, far more cells are exfoliated than can be replaced, resulting in the breakage of the gastric mucosal lining, causing erosion in the majority and bleeding in a few patients.
RED CHILI POWDER
Red chili powder and its active ingredient capsaicin were shown to significantly increase the exfoliation of surface epithelial cells of human gastric mucosa by estimating the DNA content in the gastric aspirates. Red chili powder also breaks the gastric mucosal barrier. In any patient with haemetemesis of unknown origin, ingestion of a highly spicy food in the previous meal should be determined.
The approximate amount of red chili powder per meal by Indian subjects, significantly increased gastric acid secretion – the effect of red chili powder on gastric acid secretion was studied by preventing reflux of H+ ions from the lumen, as the gastric mucosal barrier is also broken by the chilies. The DNA content of gastric aspirates significantly increased with intragastric infusion of black paper, asafetida, ginger, garlic. Substances such as red chili powder, aspirin, alcohol, which can break the gastric mucosal barrier, as well as stimulate acid secretion are likely to give conflicting results on acid secretion, depending upon the amount of gastric irritant used and the method employed to measure acid secretion.
TOBACCO
Tobacco contains carcinogens such as nicotine, polycyclic aromatic hydrocarbons, polonium, and 19- nitrosamines. Tobacco is used throughout the world for smoking but in two states of India, Maharashtra and Gujarat, it is ingested with or without pan or used as snuff or for cleaning teeth. In patients regularly chewing tobacco, the prevalence of gastric erosion on gastroduoendoscopy was as high as 20% . Further more, half an hour after the ingestion of 200 mg tobacco or one hour after the ingestion of 400 mg tobacco, per 50 patients., gastric erosions were observed in 35% and 38% patients. respectively.
ALCOHOL
7% alcohol stimulates acid secretion but 12% and 16% alcohol fails to stimulate acid secretion. This is because the higher concentration of alcohol damage the gastric mucosal barrier, resulting in the loss of H+ ions from the lumen.
STRESS
Stress induced acute gastritis with erosion, is observed in the intensive care unit in patients with severe trauma, head injury, burns, sepsis, shock, ventilatory support etc. Inflammation plays a late and secondary role in its pathogenesis and hence may be termed ‘Stress gastropathy’.
INFECTION
Acute viral hepatitis causes damage to the gastric mucosal barrier in 70% of patients.
CHRONIC GASTRITIS
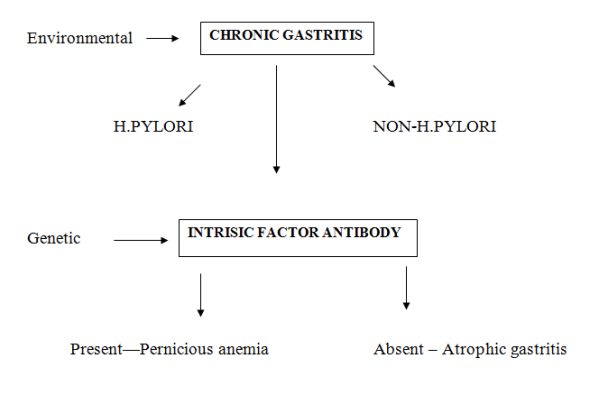
Environmental factors causing chronic gastritis may be:
- Helicobacter pylori infection
- Non helicobacter pylori infection
Various classifications of chronic gastritis based on vitamin B12 absorption, pathology, topography, immunology and endoscopic observations. In 1957 patients were separated in atrophic gastritis and pernicious anaemia on the basis of degree of vita B12 malabsorption. Those with ≥ 5 % excretion on the Schilling test were diagnosed as atrophic gastritis and those with severe B12 malabsorption ≤ 5 % excretion as pernicious anaemia.
In 1972 classified according to:
- The site of mucosa involved: pyloric, body, cardiac, transitional, interminate.
- The grade of gastritis: superficial or atrophic.
- The activity: quiescent or active.
- The presence of metaplasia: pseudo pyloric in the body mucosa, fundus or intestinal in the antrum, body or fundus mucosa.
The earliest immunological classification of chronic gastritis was reported in 1973. This classification was based on the immunological parameters, parietal cell antibody (PCA), intrinsic factor antibody (IFA), divided chronic gastritis into three types:
TYPE I: Absence of both PCA and IFA in serum, e.g. post operative or corrosive gastritis.
TYPE II: Presence of PCA and absence of IFA in the serum- superficial or atrophic gastritis
TYPE III: Presence of both PCA and IFA in the serum- pernicious anaemia
PATHOPHYSIOLOGY
H. pylori colonizes the gastric mucosa because of:
- Its motility with flagella
- Capacity to produce abundant urease to form ammonia “ cloud” for its survival in intra luminal acid
- Special affinity to adhere to the gastric epithelium and its ability to cause transient achlor or hypochlor hydria on initial exposure to the gastric mucosa
In the human stomach, H. pylori lies close to the intercellular junction of the gastric epithelial cells, underneath the surface mucus and within the gastric pits.
This location protects it from the intra luminal acid, to which it is sensitive.
Though H.pylori is non invasive, cytopathic changes are observed where it attaches to the gastric epithelial cells.
After colonization, H.pylori induces both a humoral and cellular inflammatory response.
For tissue injury important cytotoxins blamed are:
- Vacuolating cytotoxin A (vacA)
- Cytotoxin – associated gene A (cagA)
- Induced by contact with epithelium (iceA)
- Outer membrane inflammatory protein A(oipA)
- Bacteria adhesion
Various genotypes and their polymorphisms are identified by the polymerase chain reaction (PCR)
- Helicobacter heilmanni
- Glaucomatous
- Eosinophilic
- Lymphocytic
- Collagenous
- Reflux (reactive)
- Corrosive
- Post- irritation
- Tobacco induced
- Menetrier’s disease
NON H.PYLORI
- Helicobacter Heilmanni:
It is another gram negative spiral bacteria causing mild chronic gastritis.
It is probably transmitted from domestic pets. Less than 1 % of chronic gastritis results from this bacterial infection.
- Glaucomatous Gastritis:
It is diagnosed by the presence of granuloma in the mucosal biopsies which may vary in location, number, size and structure. Granuloma may occur with crohn’s disease, sarcoidosis, tuberculosis, histoplasmosis, syphilis, cryptococcal infection and post operative (structure material). The clinical radiology, endoscopy, histology and serology observations help to establish the etiology. In crohn’s disease, the focal active gastritis is present; the glaucomatous lesion is usually in antrum and may cause gastric outlet obstruction. In India, tuberculous granuloma should be excluded by staining for acid fast bacilli, performing polymerase chain reaction and/or culture.
- Eosinophilic Gastritis:
It is believed to be an allergic manifestation and may be a part of eosinophilic enteritis. It is characterized by eosinophilic infiltration of the gastric mucosa (20 eosinophils per high power field) with or without peripheral eosinophilia. Antral infiltration is common and may even cause an ulcer or a granuloma causing pyloric obstruction. A parasitic infection should be excluded.
- Lymphocytic Gastritis:
It is more often present in women and is usually asymptomatic; anorexia and weight loss occasionally occur. It is diagnosed by the presence of 30 or more lymphocytes / 100 epithelial cells (normally 3-8 intraepithelial lymphocytes). It is usually a pangastritis but occasionally affects the body mucosa only. On endoscopy, giant folds with some nodules and a few central apthous ulcer may be seen. It is associated with H.pylori infection (20%) or celiac disease (50%) and eradication of H.pylori or gluten withdrawal respectively, results in gradual improvement. In the absence of these conditions, MALT lymphoma or adenocarcinoma should be excluded.
- Collagenous Gastritis:
It is rare and is characterized by the presence of subepithelial collagen. Endoscopy shows erosions in the antrum and body mucosa and biopsy detected collagen deposition in the subepithelial region.
- Reflux (reactive) Gastritis:
It is due to reflux of duodenal contents especially bile in the gastric lumen, following operations on stomach – gastrojejunostomy, pyloroplasty or partial gastronomy.
- Corrosive Gastritis:
Corrosive ingestion, accidentally or with a suicidal intent of strong alkali or acid may result in acute gastritis mucosal damage causing erythema, oedema, erosions and ulcerations. The damage is determined by the concentration, volume, and duration of exposure and the occurrence of vomiting. Chronic gastritis and its complications – stricture may follow.
- Radiation Gastritis:
Acute gastritis may occur within a week of radiation on exposure. It usually occurs with higher doses of 4500 to 5900 CGY but may occasionally occur even with a low dose of 1800 CGY. With the availability of linear accelerator, the risk of gastritis with radiation has significantly reduced. Chronic gastritis and its complication, stricture and malignancy are observed in few patients.
- Tobacco:
Chronic gastritis has been reported in tobacco chewers. On electron microscopy, ultra structural changes fragmented basement membrane with reduction in hemidesmosome and widened intercellular spaces, similar to those observed in experimental carcinogenesis, were observed in the gastric mucosal biopsy of tobacco chewing patients.
10. Menetrier’s Disease i.e. Giant Hypertrophic Gastritis:
It is an uncommon disease in which gastric folds in fundus-body mucosa are prominent with occasional nodularity. The patient may present with edema of feet (protein losing enteropathy), diarrhea or weight loss. The histology shows elongation and dilation of gastric pits with reduction of gastric glands. Endo-sonography is helpful to differentiate prominent gastric mucosal folds, due to lymphoma, zollinger-ellison syndrome or gastric varices. Hypochlorhydria is usually present in this while basal, maximal acid output and serum gastrin are markedly elevated in patients with zollinger-ellison syndrome. The risk of malignancy is marginally increased.
SYMPTOMS AND COMPLICATIONS
In humans the absence of H.Pylori in the gastric mucosa is associated with a higher prevalence of endoscopic oesophagitis, Barrett’s esophagus and esophageal adenocarcinoma.
The presence of H.pylori in the gastric mucosa causes diseases such as:
Chronis gastritis
Duodenal ulcer
Gastric Ulcer
Mucosa-associated lymphoid tissue (MALT) lymphoma
‘Epidemic’ achlorhydria
Non Ulcer Dyspepsia(some patients)
H. PYLORI AND GASTRITIS
Symptoms:
The vast majority of chronic gastritis patients are asymptomatic. Non colicky pain in upper abdomen within 15 minutes after ingestion of a spicy meal and absence of pain on delaying or omission of a spicy meal are considered suggestive of chronic gastritis. Heaviness in upper abdomen immediately after a meal is also not an uncommon symptom. With a fiberoptic gastroscope a definite diagnosis of chronic gastritis is easy with biopsy from the body mucosa and the antrum. H.pylori causes chronic gastritis in all subjects. H.Pylori colonizes normal antrum and may extend into the body mucosa causing corpus gastritis. Chronic gastritis due to H.pylori slowly progresses over a few decades from the superficial to atrophic gastritis, intestinal metaplasia, dysplasia and gastric adenocarcinoma.
H. pylori was earlier responsible for more than 80% of chronic gastritis but its prevalence is decreasing in countries with improved sanitation.
H.PYLORI AND PEPTIC ULCER
DUODENAL ULCER:
The patients. with duodenal ulcer may present with dull aching pain in the epigastrium, occurring daily on an empty stomach or at midnight relieved soon after the ingestion of antacid, milk or non-spicy food. Nearly half of the numbers of patients with typical history of duodenal ulcer do not show any ulcer on endoscopy. The popular multi-factorial theory of stress and spices causing duodenal ulcer, died its natural death, with the discovery of H.pylori in 1983.
A major breakthrough in understanding of the etiology of duodenal ulcer was the discovery of H.pylori in the antral mucosal biopsy of humans, on upper gastrodudenal endoscopy- as; H.pylori is present in the antral mucosal biopsy of >90 % of duodenal ulcer patients., following the eradication of H.pylori from the gastric mucosa, annual duodenal ulcer recurrence reduced to less than 10% compared to 80%. Failure to eradicate H. pylori results in a higher recurrence rate of duodenal ulcer. H. pylori infection of the antral mucosa increases the risk of duodenal ulcer by 3-6 folds.
GASTRIC ULCER:
Pt. with benign gastric ulcer does not have any classical pattern of symptoms for a clinical diagnosis. Pt. may complain of dull aching pain in upper abdomen soon after food intake, nusea, heaviness, heamatemesis or symptoms of anemia.
Benign gastric ulcer is rare in Indian population, it may occur with ch.gastritis due to H.pylori or following ingestion of aspirin or NSAID. H. pylori increases the risk of benign gastric ulcer by 3 folds.
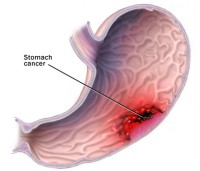
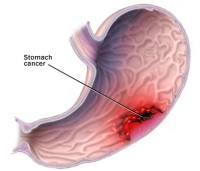
H.PYLORI AND GASTRIC MALIGNANCIES:
The patient with gastric malignancy presents with loss of weight, abdominal pain after food, nausea, vomiting, anaemia, haemetemesis and/or malena. Intestinal metaplasia is an important intermediary step in the development of gastric adencarcinoma (intestinal type). In India, intestinal metaplasia is uncommon in patients of atrophic gastritis and Type III (colonic) is rare, hence the incidence of gastric adenocarcinoma is low in South Asian population, despite a high prevalence of H. pylori in them. The exact cause for the low prevalence of intestinal metaplasia is not known but dietary factors are considered important.
MALT LYMPHOMA:
H.pylori infection increases the risk for the development of MALT lymphoma by 6-50 fold. In response to H. pylori infection, B and T lymphomas are attracted to the gastric mucosa. Monoclonal expansion and malignant transformation of B cells results in MALT lymphoma. H. pylori eradication usually cures MALT lymphoma in 70% of patients.
H.PYLORI AND ACHLORHYDRIA:
H. pylori has been blamed for the transient ‘epidemic’ hypo or achlorhydria at onset of infection, as it helps in its colonization in the gastric mucosa. Initial acid inhibition occurs due to a protein inhibition and pro-inflammatory cytokine interleukin 1B. Subsequently, acid output gradually increases over the next few months.
H.PYLORI AND NON ULCER DYSPEPSIA:
Non ulcer dyspepsia (functional dyspepsia) was initially defined as upper abdominal discomfort in the absence of an ulcer on endoscopy or barium meal.
It was later defined as ‘upper abdominal or retro-sternal pain, discomfort, heartburn, nausea,or vomiting or other symptoms considered to be referable to the proximal alimentary tract and lasting for more than 4 weeks, unrelated to exercise and for which no focal lesion or systemic disease can be responsible.’Chronic gastritis is diagnosed in about 70% of patients of non ulcer dyspepsia.
H.PYLORI AND GASTROESOPHAGEAL REFLUX DISEASE (GERD):
(a) Presence of H. pylori and GERD
In patients with oesophagitis and control subjects, the presence of H.pylori infection in the gastric mucosa was not different, indicating H. pylori (alone) in the gastric mucosa, does not affect the incidence of oesophageal mucosal damage.
(b) Presence of H. pylori corpus gastritis and GERD
There is a reduced risk of endoscopic oesophagitis in the presence of corpus gastritis. The presence of the most pathogenic H.pylori in the gastric mucosa causing corpus gastritis protects the development of GERD complications.
ABSENCE OF H.PYLORI IN THE GASTRIC MUCOSA AND GERD:
(a) Lack of exposure
In serum, helicobacter pylori antibody (HPA:IgG) prevalence was 50% in the population, at the age of 5 yrs in developing countries and at the age of 50 yrs in developed countries. With continuous improvement of sanitation in developed countries during the last four decades, the prevalence of H.pylori in the gastric mucosa is decreasing and the lifetime risk of exposure is only 10 %. The decreasing prevalence of duodenal ulcer and gastric carcinoma and the increasing prevalence of endoscopic oesophagitis and its complications, indicates the decreasing exposure to H. pylori.
INVESTIGATION
- Gastric mucosal Biopsy
- Gastric secretion: Acid, Pepsin, Intrinsic factor
- Co vita B12 excretion test
- Fasting serum pepsinogen,serum gastrin
- Parietal cell, intrinsic factor, helicobacter pylori antibody
- H.pylori detection : invasive ,non invasive methods
THE HOMOEOPATHIC APPROACH
Abdominal pain and inflammation present difficulties in diagnosis for even the most experienced physician. All cases of dynamic diseases, acute or chronic even when resulting from mechanical or psychological injuries, are amenable to homoeopathy. The homoeopathic medicine works quite well in the treatment of an acute abdomen often averting the need for surgery in many of cases. The problem may range from entrapment of gas, to constipation, perforation of the bowel which results in sever inflammation and sepsis which may result in death. Any acute onset of abdominal pain should be considered a medical emergency.
By carefully applying the law of similars, the physician will observe that all cases of curable dynamic disease are curable with homoeopathy. To achieve this, the physician must be thoroughly familiar with the principles of homoeopathy as taught in the ORGANON and must know how to make the use of materia medica.
Repertories are used as essential links between the patient’s symptoms and the vast materia medica.
Clinical guides such as below mentioned, provide a synopsis of the most characteristic symptoms of the leading remedies in a given condition. Their objective is to give assistance only. While using it one has to be aware of two general drawbacks. One, it may fail because of its incompleteness as only leading remedies in given a given condition can be presented, and the symptomatology of each remedy presented is limited to only the leading characteristic symptoms.
In clinical practice the patient will most of the time present some symptoms that can only be found in a more complete materia medica. Second, there is the inevitable temptation to associate remedies with a given disease. The practice of homoeopathy consists of constant individualization. – The more we understand this science the more we individualize. Frequent follow up to monitor the patient’s condition is a must.
ABIES CANADENSIS:
Gnawing, hungry faint feeling at the epigastrium
Burning and distension of stomach with palpitation
Tendency to eat far beyond the capacity for digestion
Great appetite, craving for meat, pickles, radish, turnips, coarse food
Flatulence disturbs the heart’s action
Wants to lie down all the time
ABIES NIGRA:
Pain in stomach always comes on after eating
Sensation as if a hard-boiled egg had lodged in the cardiac end of stomach
Great craving for food at noon and night
Dyspepsia of the aged, after tea or tobacco
Sour eructation
ACETIC ACID
Constitution – Pale, lean, emaciated persons.
Symptoms relating to GIT indicating hyperacidity – Burning pains as of an ulcer
Cancer of stomach
Sour eructation
Vomits every kind of food
Heartburn and water brash
Hyperchlorhydria
Concomitants – Profuse salivation
Intense burning thirst
Haemorrhage from bowels
Great prostration.
ANACARDIUM
Symptoms relating to GIT indicating hyperacidity – Duodenal ulcer; All gone sensation when stomach is empty, > by eating, during the process of digestion
Apt to choke while eating and drinking
Swallows food and drink hastily
Pain usually two hours after eating, with a dull epigastric pain extending to the back of the trunk
Always better after eating
Concomitants – Ineffectual desire for stool, rectum seems to be plugged up
Sensation of a band or hoop around a part
Sudden loss of memory
ARGENTUM NITRICUM
Ulceration of stomach with radiating pains
Gnawing, burning splinter like pains
Belching accompanies most gastric ailments
Nausea, retching, vomiting of glary mucus
Flatulent dyspepsia, stomach distended as if it would burst with wind
Diarrhoea, green mucus like chopped spinach < eating candy, sugar, sweets, ice creams
Diseases from unusual or long continued mental exertion
ARSENICUM ALBUM:
Cause – Gastric derangements after fruits, ice creams, beer, strong cheese, alcohol
Symptoms relating to GIT indicating hyperacidity – Burning pains in abdomen, burns like fire, as if hot coals were applied to the parts
Vomiting of bile, blood, brown black mucus mixed with blood
Gastralgia < at mid day and mid night
Severe, burning pain and exhaustion; pain immediately after eating food and a lack of appetite
Modalities – > by heat, hot drinks
Keynotes – Cannot bear the smell or sight of food
Excessive thirst for warm drinks at short intervals
Fear, anxiety, restlessness
Prostration
ATROPINUM
Chronic stomach affections
Paroxysms of gastric pains
Vomiting of all food
Hyperchlorhydrea
Pyrosis
Great dryness of throat, almost impossible to swallow
BISMUTH
Symptoms relating to GIT indicating hyperacidity – Gastralgia, pain from stomach through to spine
Vomiting of water as soon as it reaches the stomach, food retained longer, of enormous quantities at intervals of several days when food has filled the stomach
Pressure in stomach as from a load in one spot, alternating with burning, pain crampy, spasmodic
CALCAREA CARB
Acidity of the digestive tract, sour eructation, sour vomiting, sour stool, sour odour of the whole body
Ravenous hunger
Pit of stomach swollen like an inverted saucer, painful to pressure
Aversion to milk and meat, craving for eggs
Habitual constipation, stool has to be removed mechanically
Leucophlegmatic, fair, obese persons
CALCAREA PHOS
At every attempt to eat, colicky pain in stomach
Heart burn
Much flatulence
Craving for bacon, ham, salted or smoked meat
Flatulence temporarily > by sour eructation
Easy vomiting
Green, hot, spluttering diarrhea
Sunken, flabby abdomen
Feeble digestion
Anemic, thin, spare subjects
Ailments from grief, disappointed love
Feels complaints more when thinking about them
CADMIUM SULPH
Burning and cutting pains in stomach
Carcinoma
Persistent vomiting, violent nausea, retching, vomiting of black, coffee ground matter, of blood
Severe prostration
Black offensive clots of blood from bowels
Chilliness and coldness
CARBO VEG
Weak digestion, simplest food disagrees, excessive accumulation of gas in stomach and intestines (upper abdomen), sensation as if abdomen would burst
Eructations give temporary relief
Haematemesis and malena
Bad effects of fatty food, pork, butter, late supper, debauch, salted meat, spoiled fish or meat
Frequent involuntary cadaverous smelling stools
Carcinoma of stomach, late stages of disease
Complaints from loss of vital fluids, broken down constitution
CINCHONA
Hyperacidity, vomiting of undigested food
Hungry with out appetite
Excessive flatulence of stomach and bowels (lower abdomen), fermentation, belching gives no relief
Colic at a certain hour, each day, periodical< night, eating fruits, touch
> Hard pressure, bending double
Diarrhoea painless at night, undigested food particles
Haematemesis and malena
Hemorrhage long continued
Ulcers with persistent suppuration
Longing for sour things
Broken down constitution, loss of vital fluids
CONDURANGO
Symptoms relating to GIT indicating hyperacidity – Gastric ulcer, carcinoma of stomach
Constant burning pains
Vomiting of food, burning behind sternum, where food seems to stick
Stricture of esophagus
Chronic gastric catarrh
CROTALUS HORRIDUS
Symptoms relating to GIT indicating hyperacidity – Gastric ulcer, cancer of stomach
Vomiting of bloody slimy mucus
Black or coffee ground vomiting
Violent vomiting of food
Concomitants – Haematemesis and malena
Chronic alcoholism
Intolerance of clothing around stomach
Diarrhoea, stool black, offensive, like coffee grounds. Black, dark, fluid, non coagulable blood
Tongue fiery red, smooth and polished
Prostration, broken down constitution
GERANIUM MACULATUM
Catarrhal gastritis with profuse secretion, tendency to ulceration and passive hemorrhage
Lessens the vomiting in gastric ulcer
Vomiting of blood
Atonic, foul ulcers
Constant desire to go to stool, with inability to pass anything for sometime
GRAPHITES
Symptoms relating to GIT indicating hyperacidity – Duodenal ulcer; Chronic constipation, stool hard knotty with lumps united by mucus threads
Modalities – > – after eating, drinking hot milk
GRINDELIA SQUARROSA
Symptoms relating to GIT indicating hyperacidity – Gastric ulcer, gastric pains associated with splenic congestion
Nausea and retching
Hyperchlorhydria
Hyperemia of gastric mucus membrane
Dullness and pain in left hypochondria
Paresis of pneumogastric
Gastritis with asthmatic symptoms
HYDRASTIS
Constitution – Old debilitated persons.
Symptoms relating to GIT indicating hyperacidity – Gastro duodenal catarrh
Carcinoma of stomach
Cachetic or malignant dyscrasia
Ulcerations, profuse discharge of thick yellow stringy mucus
Atonic dyspepsia
Concomitants – Chronic constipation
Enlarged liver, jaundice
Cancer pains
Broken down by excessive use of alcohol
IODUM
Constitution – Emaciation, loosing flesh while eating well
Scrofulous diathesis
Symptoms relating to GIT indicating hyperacidity – Duodenal ulcer; Empty eructation, as if every particle of food was turned in to air
Constipation > by drinking cold milk
Ravenous hunger,
Modalities- > – while eating or after eating
IRIS VERSICOLOR
Hyperacidity, burning of the whole alimentary canal
Vomiting sour, bloody, biliary
Nausea, profuse salivation
Deficient appetite
Diarrhoea stools watery with burning of anus
KALI BICHROMICUM
Symptoms relating to GIT indicating hyperacidity – Gastric ulcer; punched out or round ulcer of stomach
Pain in small spots, can be covered with the point of finger; appears and disappears suddenly, rapidly shifting
Pain in the epigastric region
Burning or shooting abdominal pain
Weight in pit of stomach, flatulence, vomiting of stringy, ropy mucus and blood
Loss of appetite
Modalities- < – immediately after eating, after midnight
KREOSOTE
Gastric ulcers; Carcinoma of stomach
Vomiting of food several hours after eating, vomiting of sweetish water with ptyalism
Haematemesis and malena
Flow passive, dark, oozing
Diarrhoea offensive, dark brown, bloody stools
Corrosive fetid ichorous discharges from mucus membranes
LYCOPODIUM
Constitution – Carbo-nitrogenoid constitution
Intellectually keen but physically weak
Upper part of body is emaciated, lower part semi-dropsical. Unhealthy complexion looks older than he is
Cause – Dyspepsia due to farinaceous and fermentable food, cabbage, beans, etc.
Symptoms relating to GIT indicating hyperacidity – After eating, pressure in stomach, with bitter taste in mouth
Eating even little causes fullness
Immediately after a light meal there is bloating and fullness of stomach
Incomplete burning eructation
Sour eructation
Rolling of flatulence
Food and drink regurgitates through nose
Wakes at night feeling hungry
Concomitants – Aversion to bread
Desire for sweets
Likes to take food and drink hot
Excessive hunger
Stool hard, difficult, small, and incomplete.
Keynotes – Right side complaints
Fan like movement of alae nasi
Half open eyes in sleep.
Modalities –
< – 4 to 8 p.m., right side, heat except throat and stomach.
> – warm food and drink, loosening the garments, open air.
NATRUM PHOS
Excessive acidity, sour eructation, sour vomiting, spits mouth full of food
Gastritis, Flatulence
Yellow creamy coating at the back part of tongue and roof of mouth
NUX MOSCHATA
Gastric ulcer; Pain in stomach while or immediately after eating
Eating a little too much causes headache
Abdomen enormously distended after every meal
Flatulent dyspepsia
Diarrhoea, stool white, fetid
Great dryness of mouth without thirst
Women, hysterical temperament, drowsiness, sleepiness, inclination to faint
NUX VOMICA
Constitution – Thin people, with dark hair and dark complexion, who lead a sedentary life, nervous, extremely sensitive to external impressions
Cause – Dyspepsia from drinking strong coffee, high living, alcohol, highly spiced seasoned food, irregular diet, and long continued mental or physical stress, excessive intake of medicines.
Symptoms relating to GIT indicating hyperacidity – Nausea in the morning and after eating
Weight and pain in stomach which is worse some time after eating
Nausea and vomiting, with much retching
Epigastrium bloated, with pressure as of a stone, several hours after eating
Sour, bitter eructation
Concomitants – Region of stomach very sensitive to touch
Desire for stimulants
Loves fat and tolerates them well
Constipation, with frequent ineffectual urging; passing small quantity at each attempt; feeling as if part remained unexpelled. Throat: rough, scraped feeling
Tickling after waking in morning
Other keynotes – Oversensitive to all external impressions
Extremely irritable
Aversion to cold air
Irresistible desire to sleep in the evening
Modalities –
< – morning, mental exertion, after eating, stimulants, spices, cold, dry weather
> – in evening, damp wet weather
PETROLEUM
Duodenal ulcer; Ravenous hunger, must rise at night to eat
Pain abdomen > by constant eating <empty stomach, eating cabbage
Heartburn, nausea
Diarrhoea only in day time
Symptoms appear and disappear suddenly.
PHOSPHORUS
Burning pains in stomach > by cold drinks, ice creams, juicy refreshing things
A weak empty all gone sensation in entire abdomen
Vomiting, water is thrown up as soon as it gets warm in stomach
Vomiting of blood
Carcinoma of stomach
Bleeding ulcers, frequent, profuse
Discharge of blood from rectum during stool
Diarrhoea, stool involuntary, watery, sago like particles, coffee ground
PULSATILLA
Pain in stomach an hour after eating
Pain with chilliness, rapidly shifting, appear suddenly, goes gradually
Vomiting of food eaten long before
Eructation, taste of food remains a long time
All gone sensation in tea drinkers
Complaints from eating rich food, cake, pork, sausage
Thirstlessness with dry mouth and tongue
Diarrhoea only at night, greenish yellow, very changeable
ROBINIA
Symptoms relating to GIT indicating hyperacidity – Intensely acrid eructation.
Nausea, with sour eructation
Profuse vomiting of an intensely sour fluid; acrid and greenish vomiting
Great distension of stomach and bowels
Flatulent colic
Incarcerated flatus
Sour stools
Acidity in children; child smells sour
Nightly burning pains in stomach with constipation with urgent desire
Concomitants – Frontal headache, dull, throbbing; worse motion and reading
SULPHUR
Burning pains in stomach < at night, warm food and drinks
Weak empty all gone sensation at about 11 am > by eating, cannot wait for lunch
Acidity, sour eructation
Desire for sweets
Diarrhoea, driving out of bed early in the morning
Constipation stools hard, dry as if burnt, painful
Redness of external orifices
Chronic alcoholism
Nervous temperament, scrofulous diathesis
SULPHURIC ACID
Hyperacidity, heartburn, sour eructation, sets teeth on edge
Sour vomiting
Haemorrhage of black blood from bowels
Ulcers bleed easily
Water causes coldness of stomach, must be mixed with alcohol
Pains come gradually and go suddenly
Tremor and weakness
SYMPHYTUM
Gastric and duodenal ulcers
Gastralgia
Stimulates the growth of epithelium on ulcerated surfaces
URANIUM NITRICUM
Gastric and duodenal ulcers
Ravenous appetite, eating followed by flatulence
Boring pain in pyloric region
Excessive thirst, nausea, vomiting
Burning pains
Abdomen distended
Great emaciation, debility
Diabetes, ascites, nephritis, hypertension, degeneration of liver
PREVENTION
Prevention of H.pylori Infection –
In developing countries, the major mode of transmission of H.pylori infection is the faeco-oral route due to contaminated water or food, poor sanitation and personal hygiene. If a pure water supply is guaranteed, the risk of H. pylori infection dramatically decreases. Supplementation of vitamins A and C have positive impact.
The most serious complications of peptic ulcer – haematemesis and /or malena and perforation, can be prevented by avoiding drugs like NSAID’s, Aspirin etc. in all patients with active or past history of peptic ulcer.
Proper diet regimen can help in prevention peptic ulcer formation. It also helps in speedy recovery and arrests the further progression of complications. Dietary and regimen measures that should help are as follows:
DO’s
The food should be masticated well and swallowed.
The food should be taken in a relaxed manner, without any hurry.
TO TAKE
Easily digestible, oil free diet to reduce the workload of the stomach and intestines. Frequent small meals should be encouraged.
Water is to be taken before and after meals.
Nutritious diet should be taken at regular intervals.
Diet rich in fiber, like green vegetables and fruits which are good for digestion and also for the general health should be consumed regularly.
Foods containing flavonoids, like apples, celery, cranberries (including cranberry juice), onions, and tea may inhibit the growth of H. pylori.
AVOID
Smoking, drinking alcohol, chewing tobacco and overeating which increases acid secretion of the stomach.
Hunger – which denotes acid load, avoid it by taking small meals often.
Full meal, oily diet, pickles and fatty snacks before bed time.
Food containing spices like chilies and pepper.
Dry bread, cakes and cookies.
High fat content nuts and biscuits.
Aerated drinks, coffee and tea.
Milk products.
Stress by the regular use of relaxation techniques such as yoga, tai chi, or meditation.
Cabbage, onions, garlic, cauliflower, tomatoes – if not tolerated
Drugs like NSAIDs – pain killers (for example. – aspirin)
REFERENCE:
- http:// www.nlm.nih.gov/medlineplus/
- http://www.niddk.nih.gov/
- http://www.emedicine.com/EMERG/topic820.htm
- http://www.diagnosishealth.com/ulcer.htm
- http://www.dietsite.com/Diets/
- Harrison’s Principles of Internal Medicine, 14th ed, McGraw-Hill
- Davidson’s Principles and Practice of Medicine, 17th ed, 1996, Churchill Livingstone
- New Manual of Homeopathic Materia Medica & Repertory, William Boericke, 2nd revised ed., 2001, B. Jain
- A Concise Repertory of Homeopathic Medicines, S.R.Phatak, 3rd ed, B. Jain
- The Prescriber, Clarke, reprint ed, 1998, B. Jain
- Practical Homeopathic Therapeutics, Dewey, reprint ed, 1993, B.Jain

An all encompassing, comprehensive and detailed article on the subject. Very very useful.
DEAR DR,
YOUR LABOUR IS VERY EXTENSIVE. THE ARTICLE HAS COVERED ALL THE REMEDIES. IT IS BETTER IF THE COMMON SYMPTOMS OF REMEDIES ARE EXCLUDED. IT WOULD HAVE BEEN EASIER TO GRASP THE REMEDIES FOR THEIR PIN POINTED DIFFERENCES
THANKS
kindly accept my sincere thanks for writing a beautiful article on gastritis with lot of information on etiology, pathology,diagnosis and homoeo treatment with appropriate drugs.