Introduction
Thyroid cancer is the most common endocrine malignancy and its indigence is increasing. Differentiated thyroid cancer consists of papillary, follicular, and Hurthle cell histological types. Although it typically has a good prognosis due to its long, indolent, and well-tolerated natural history, lifelong follow-up is recommended as late recurrences may occur after surgery.
Advances in diagnostic modalities and pathologic analysis continue to evolve. High resolution ultrasound plays an increasingly important role in the management of thyroid cancer, including diagnosis of malignancy, preoperative lymphatic mapping and postoperative surveillance. Surgery remains the mainstay of therapy; however, thyroid suppression, and radioactive iodine ablation also contribute to the treatment.
Causes and risk factors
The most important risk factor for thyroid cancer is early exposure to radiation. The radiation source can be X-rays or radioactive fallout. Radiation can damage genes, leading to mutations that allow cancer to develop and spread. Family history and gender are also important. Rates of thyroid cancer in women are almost three times higher than those seen in men.
Symptoms of Thyroid Cancer
As with many other forms of cancer, most people in the early stages of thyroid cancer have no symptoms or signs of disease. When symptoms or signs occur, they may include the following:
- Hoarseness
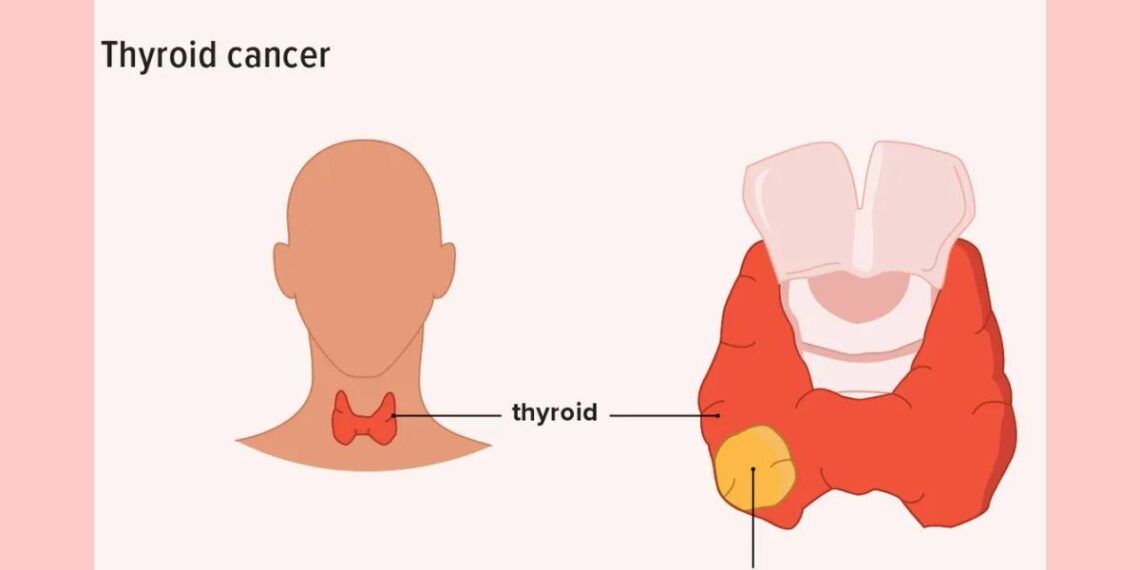
- A lump near the Adam’s apple of the neck
- Swollen lymph nodes in the neck or near by
- Dysphagia (difficulty swallowing)
- Pain in the neck or throat
Medullary carcinoma of the thyroid can cause symptoms such as flushing, nausea, and diarrhea. In addition, medullary carcinoma of the thyroid is often inherited. Family members can be screened by measuring their calcitonin levels or by looking for abnormal chromosomes, such as RET.
Anaplastic carcinoma typically presents in older men as a very hard mass in the neck. It is often incurable at the time of diagnosis, as it does not concentrate iodine, and thus radioactive iodine (RAI) therapy cannot be used. It is poorly responsive, if at all, to chemotherapy and external addition therapy.
Diagnosis
With the increasing use of ultrasound, thyroid nodules are detected on a more regular basis. Features suggestive for thyroid malignancy can also be detected on ultrasound such as hypoechoic echotexture (86%), micro-calcifications (42%) or no calcifications (47%), well defined margins (47%), and intrinsic hypervascularity (69%).
Less common features include hyperechoic or mixed echo texture, cystic elements, irregular margins, hypovasularity, and coarse or peripheral calcifications. Preoperative lymphatic mapping using ultrasound is a relevant development in the evaluation of patients with involved lymphadenectomy.
The diagnosis of thyroid cancers relies on FNA of thyroid nodules.. Although FNA is an accurate diagnostic test for papillary carcinomas, it cannot reliably discriminate between follicular thyroid cancers and benign follicular adenomas. For follicular tumors the diagnosis cannot rely upon FNA findings since certain histological features such as blood vessel or tumor capsule invasion are required for a diagnosis of cancer. Although some surgeons use intraoperative frozen section to guide operative management, frozen section is not useful for follicular or Hurthle cell cancers, as the tissue processing distorts the architecture of the nodule and does not permit accurate assessment of capsular or vascular invasion.
Other diagnostic modalities for accurate localization and anatomic definition of disease are Computed Tomography (CT) or magnetic resonance imaging (MRI) scans of the neck and positron emission tomography (PET) scanning.
Since patients commonly undergo CT scans and PET scanning for unrelated conditions, incidental thyroid findings are frequently encountered. However, there is no indication for routine use of CT scans or PET scans to determine presence or histology of thyroid nodules. If, however, certain pathologic clinical finings are noted or metastatic disease is encountered then further investigational studies such as CT and PET scans are employed.
CT scanning of the neck is most helpful when local regional invasion is suspected based on presentation and physical examination. If malignancy is strongly suspected, it is important not to use intravenous contrast during CT scanning, as the associated iodine load will delay radioactive iodine ablation by 3-4 months.
Management
Surgery is an essential part of the initial management of carcinoma of the thyroid and it is recommended that this be performed in the context of a specialist thyroid cancer programme. Thyroid cancer is usually very radiosensitive, so radioiodine an important treatment, initially to ablate the remaining normal thyroid, and subsequently used to target residual cancer.
Lifelong follow- up is required as recurrent disease may develop after many years. The prognosis is generally excellent with 10 year disease free survival of over 90% in well differentiated thyroid carcinoma.
Homeopathic treatment of thyroid cancer symptoms – Homeopathy is one of the most popular holistic systems of medicine. The selection of remedy is based upon the theory of individualization and symptoms similarity by using holistic approach. This is the only way through which a state of complete health can be regained by removing all the sign and symptoms from which the patient is suffering. The aim of homeopathy is not only to treat thyroid cancer but to address its underlying cause and individual susceptibility. As far as therapeutic medication is concerned, several remedies are available to manage thyroid cancer symptoms that can be selected on the basis of cause, sensations and modalities of the complaints. For individualized remedy selection and treatment, the patient should consult a qualified homeopathic doctor in person. There are following remedies which are helpful in the treatment of thyroid cancer symptoms:
Silicea, Graphites, Calcaria Carb, Phosphorous, Sulphur, Conium, Hepar Sulph, Thuja, Lachesis, Nitric Acid and many other medicines.
Reference:
Johnathan G. H. Hubbard, William B. Inabnet, Chung- Yau Lo- Endocrine Surgery: Principles and Practice; 2009; 111-13
Marshall Cavendish Corporation- Diseases and Disorders, Volume1; 2007; 170
William A. Petit, Christine A. Adamec- The encyclopedia of endocrine disease and disorders; 2005; 224
Shern L. Chew, David Leslie, R. D. G. Leslie- Clinical endocrinology and diabetes: an illustrated colour text; 2006; 07
Some Related Cases Cured with Homeopathic Medicine
Practical Insights for Use of Homeopathy in Cancer Patients – Arup Bhattacharya



hi i am Dr. taher from Dhaka Bangladesh. i am new comer in this site. i think all of my friend share with me ………… !