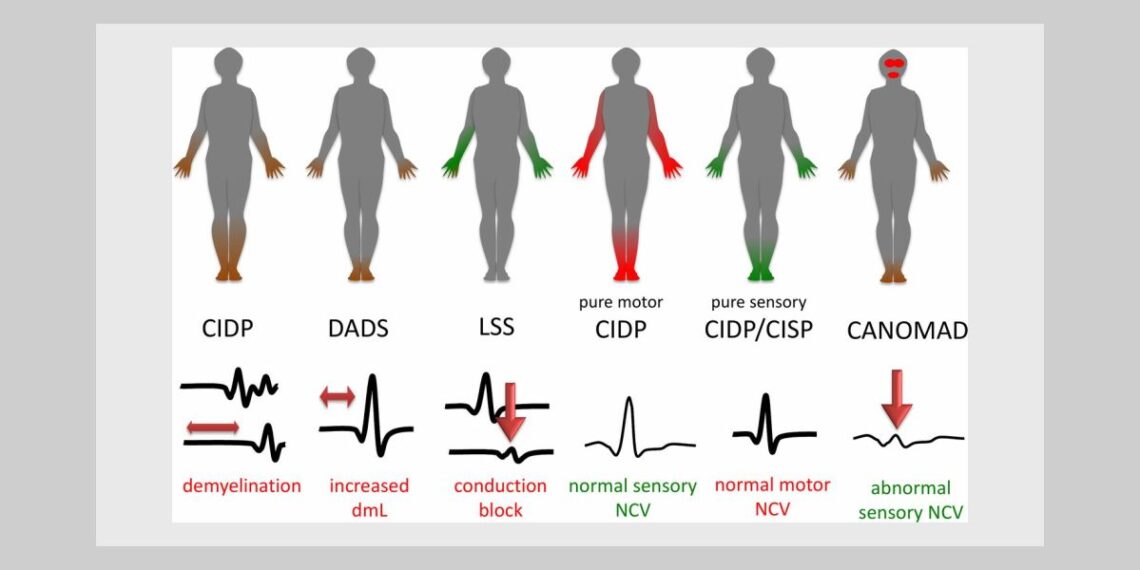
Chronic Inflammatory Poly Neuropathy Disease can be defined as an acquired neuropathy. It has been considered to be of immunological origin. Its clinical presentation and progression is extremely variable. Classic CIDP is characterized by symmetric proximal and distal weakness and loss of sensation. However this can also vary significantly whereby purely motor and/ or sensory involvement can occur. There are many variants which can be pathological, temporal or disease associated. Typical cases associate progressive or relapsing-remitting motor and sensory deficit with increased CSF protein content and electrophysiological features of demyelination. Axon loss associated with demyelination is the most important factor of disability.
Presenting symptoms:
Female 62 years of age presents with a progressive loss of sensation that began in her toes and is progressively moving upwards. She first noticed the symptoms when she suffered from multiple broken toes in a short period of 2 years. Patient described the symptom as ‘not feeling where her feet ended’ and as a consequence kept walking into things and suffering from injuries to the toes on multiple occasions.
The following is an excerpt of her symptoms in her own words:
“My feet are completely numb. I can wiggle my toes by telling my brain but I cannot feel them doing so. I can see that they are responding but I have lost the sensation of this. It is an unnerving feeling. My feet feel warm to touch but I am mindful that I wear warm socks because I am worried that because I cannot tell if my feet are cold that I will get chilblains. I first started noticing this about 2 years ago when I was in bed. I like to rub my feet together at night because I like the sensation and I progressively started to lose the feeling. Then I broke toe after toe (on both feet, multiple toes). It was definitely worse on the left side to begin with but now I would say that both feet are just as bad as the other. I have to be very careful to check the bath water with my hands before I step into it otherwise, I would scald my feet.”
She describes the situation as “numbness”. It began with a tingling sensation but has now progressed to heaviness. She states that her feet ‘feel like lead.’ When she attempts to jump, she cannot gain enough lift from the ground. ‘I cannot spring. I have lost the spring in my step.’ She also describes a loss of coordination that is locomotor and often ‘awkward’ causing her to stumble and frequently stagger.
Past History:
Patient suffered a grand mal at age of 13 years, after a sexual experience that brought on her first menses within a few hours. She states that this was a tumultuous time in her life as she received a big shock from her first menstrual period, believing that she would die as she did not know what it was and she had been hyper stimulated by the experience. The rubric Convulsions, epileptic from fright would be useful if treatment proceeded or convulsions, menses aggravates, or even convulsions, masturbation, after.
Shingles, severe, repeated bouts throughout adulthood, last episode 3 years ago.
After comprehensive case taking the patient also relates some short term memory loss and occasional bouts of confusion.
Medications:
Both long-term and current include: Dilantin and Neurontin. Most of the common side effects of Dilantin that have been researched are coordination problems, twitching, muscle spasms (uncontrollable), problems with coordination or balance, low blood pressure, slurred speech and confusion. Neurontin is prescribed for nerve pain which occurs with shingles (post herpetic neuralgia), and can also be prescribed alongside other seizure medications. Side effects are similar to Dilantin but depression is emphasized with similar coordination concerns highlighted.
In this case the patient has been on long term medication for epilepsy since an early age and probably is suffering from this as a result, with the CIDP pathology progressing.
This particular case is an interesting one, and I discuss many similar to these when supervising students in clinic or deconstructing a case within class. Often new students struggle most with where to begin the case after they are overwhelmed by a myriad of information. Often they have high expectations upon themselves to find the Similimum within the first consult and this resulting inability to do so leads to a lack of confidence.
This particular patient is a well educated woman who has researched her condition and the pharmacology associated with her medication. She is aware of the long term prognosis and requests that she does not want to have her epilepsy addressed as she is concerned that long term homoeopathic treatment will generate another epileptic episode and she has not had one for many years. However she is concerned about the progressive nature of her condition, as it seems to be rising upwards and she fears complete loss of the use of her legs.
Patient education is an essential part of our consult and many options were discussed. This case can be approached from many angles including lesional, functional, drainage, aetiological, miasmatic, tautopathic etc., but it is important that the needs of the patient be met and balanced with the principles and practice of homeopathic cure. Many rubrics giving specific case information were assessed. These included: Extremities, heaviness, lower limbs; Extremities, heaviness, feet; Extremities, Incoordination; Extremities, pain, feet, as if paralysed; Extremities, pain feet, soles, rubbing amel; Generals, numbness, affected parts and many others.
An interesting rubric for future consideration may have been: Generals, neurological, fright from (convulsions) as a possible aetiological similimum when the case calls for it.
Based upon the totality of the case the prescription of Plumbum met. was made and prescribed at irregular intervals in a 30c potency. Up to this point the loss of sensation was rapidly rising through to her calves and the specialist advised her to undertake a nerve biopsy, which she was unprepared to do.
Following prescription one month later, many significant symptoms including mental and emotional key points had significantly improved. Within 3 months the sensation had returned to her calves and continued to progress downwards. She has not displayed any evidence of an epileptic convulsion since homoeopathic treatment began and her memory and general wellbeing has improved.
She has been stable now for a period of one year with the condition remaining in her toes on both feet. This appears to have stalled at present for a substantial period of time but she is happy with the results and does not want to consider any changes at this point. Her ability to jump and spring off the ground has doubled in height since we first began and we used this as a measurement tool to chart progress throughout her treatment.
Whilst this case may not be ground breaking or exceptional in prescription or process, I think that it is important to highlight the obstacles to cure that modern homoeopath’s face and be more realistic about our limitations and expectations. The challenge sometimes is to balance our expectations with the desires of the patient. The Florence Nightingale within me would have once proceeded with all guns blazing and gone in with a complicated and unfolding list of prescriptions that involved many methods and principles of practice over a period of time in my unending pursuit towards cure. Would this have been the best course of action for the patient? I think that I can safely say no, given the experience that I have now gained over time and the patience and wisdom that only deep reflection can provide when reviewing our own clinical cases.
These days I prefer a more balanced approach. In sharing this case with others, I hope to address the lack of confidence amongst our future peers and encourage them to continue to build upon their skills in a more practical and thoughtful way, without placing such huge expectations upon themselves.
References:
Schroyens,F (2007) The Essential Synthesis, Homeopathic Book Publishers, London.
Hahn AF, Bolton CF, Zochodne D and Feasby TE. Intravenous immunoglobulin treatment in chronic inflammatory demyelinating polyneuropathy: a double-blind, placebo-controlled, cross-over study. Brain 1996;119:1067-77.
Hughes R, Bensa S, Willison H, Van den Bergh P, Comi G, Illa I, Nobile-Orazio E, van Doorn P, Dalakas M, Bojar M, Swan A. Inflammatory Neuropathy Cause and Treatment (INCAT) Group. Randomized controlled trial of intravenous immunoglobulin versus oral prednisolone in chronic inflammatory demyelinating polyradiculoneuropathy. Ann Neurol 2001;50:195-201.
Hughes RA, Donofrio P, Bril V, Dalakas MC, Deng C, Hanna K, Hartung H-P, Latov N, Merkies ISJ, van Doorn PA, ICE Study Group. Intravenous immune globulin (10% caprylate-chromatography purified) for the treatment of chronic inflammatory demyelinating polyradiculoneuropathy (ICE study): a randomised placebo-controlled trial. Lancet Neurol 2008;7:136-44.




I have to Start Same case and I hope to Curing him.
Thanks for this Report. its very Nice Work.
Regard
Saeid