The Case
A.B, a 5-year old boy was brought by parents to the Homeopathic Center on October 1, 2012. The parents informed me that the child had been experiencing gastric problems since his birth. The first 3 months he had suffered from infantile colics followed by constipation with abdominal pains, crying and straining when defecating since he was 6 months old. By 1.5 years old, constipation had become less pronounced. Stool had changed its nature and became seedy, with particles of undigested food, periodically foul-smelling, frothy and with mucus. By the time of the visit, stool was permanently seedy, foul-smelling, with particles of undigested food, fatty and irregular, either 2 times a day, or every other day. Occasionally, the boy had mild fecal incontinence when coughing or sneezing. The child was experiencing periodical epigastric pains (more rarely) in the para umbilical area since 1.5 – 2 years old. The pains were first mild, then cleared up on their own or after spasmolytics. During the last 10 months the pains intensified, and tended to result in vomiting, which forced the parents to visit a doctor and hospitalize the child (three episodes).
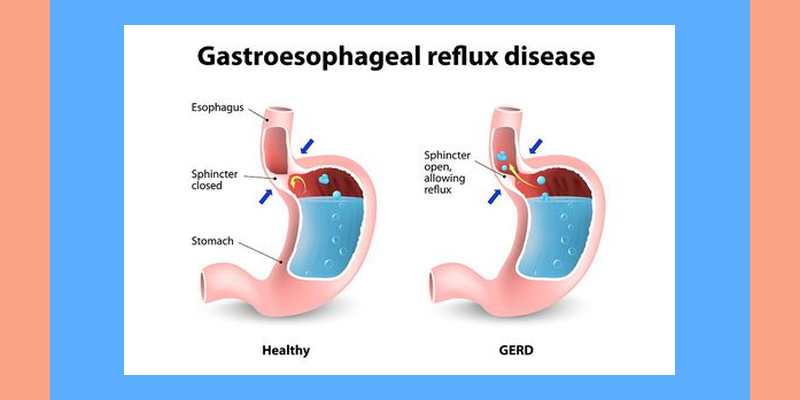
The next problem was heartburn and belching which appeared when he was 3 years old. In the beginning those events were rare, but by the time of their visit, soft belching was observed after each meal. Belching could be sufficiently abundant, and the mother noticed the son to be chewing over what he had eaten half an hour or one hour before. Or, for instance, the drug he had swallowed half an hour before turned out to be in his mouth again.
Esophago-gastro-duodenoscopy (EGD) showed duodenitis events and a positive Helicobacter pylori test result. Ultrasound examination demonstrated increased echogenicity of the pancreas and biliary dyskinesia. A bacteriological test of stool revealed the absence of bifidus/lactobacilli. Thus, remittent gastric pains, stool/digestion disorders, frequent and abundant belching were the main complaints at the examination time. Continuous drug therapy including peristaltic modulators (motilium) and drugs decreasing stomach acidity, as well as the use of enveloping agents, enzymatic drugs, and bifidus/lacto bacilli productshad no appreciable effect.
In addition, the parents mentioned that since around 3 years the child had often suffered from Acute Respiratory Infection with a high temperature and had been treated with antibacterial drugs 2 – 3 times a year. A year before the visit he had been twice treated for obstructive bronchitis and received inhalations of berodual (salbutamol) with pulmicort (cortisone).
Taking into account the nature of the chronic pathology (inflammation of the gastrointestinal mucosa with its dysfunction, absence of deep degenerative damages of tissues and organs) and frequent acute infections of moderate severity, the child was graded as belonging to health group B (4 – 5 levels) according to G. Vithoulkas’ classification.
As for general symptoms, it was worth noting that the boy was hot thermally, liked to bathe in cool water and required a cold pillow and a blanket when going to sleep. He also refused to eat meat, preferred fish and gave up eating eggs since he was 2 years old (sweet and milk – within normal). No emotional pathologies were observed: he was an obedient, sociable child, without expressed fears. Physical appearance was asthenic, the tongue had a yellowish color, some tenderness in the gastroduodenal zone.
Initial flat repertorization brought the following findings:
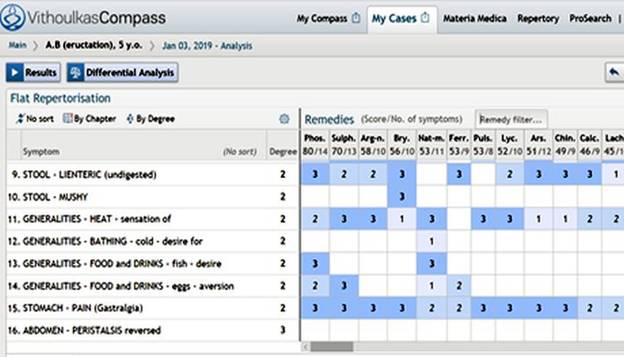
None of basic remedies obtained in compliance with the symptoms complex was confirmed by appropriate key signs. Sulphur seemed to be the most relevant remedy (hot patient, stool disorders, aversion to eggs), however, the patient did not demonstrate morning diarrhea, heat in feet, desire for sweets. To prescribe Lycopodium, there should be flatulence, deterioration of the general state in the morning, and at 16 -20 hours, as well as a great desire for sweets. Argentum nitricum was also rejected because the patient was indifferent to sweets, and also no aggravation when eating sweets, no conventional fears or impulsiveness were observed, belching occurred noiselessly and not noticed by people around him, which was atypical for the given preparation.
But the result of Vithoulkas Compass – expert system was completely different:
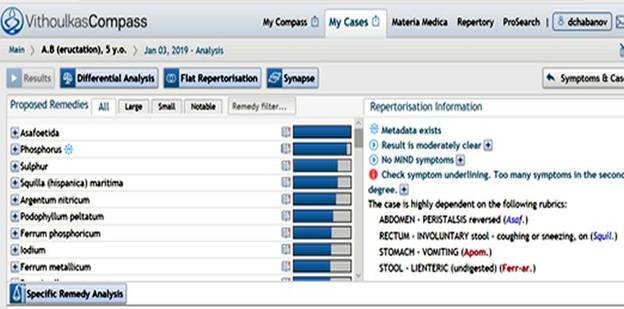
Indeed, the most unusual and striking symptom in this case was belching with a mouthful of food. Materia Medica states that antiperistaltic catastalsis of the esophagus with a belched content of the stomach (“everything goes up, nothing comes down”) is most typical for Asafoetida. Its pathogenesis also contains foul-smelling, liquid undigested stool.
Thus, based on the main signs of pathology (G. Vithoulkas’ “essentials” strategy), primarily taking into account the striking symptom – burping large volumes of food, Asafoetida was chosen as a remedy for therapy.
Prescription: Asafoetida 30C in solution (5 globules to be dissolved in 60 ml of water and taken 3 times a day with a 5-6 – hour interval in between) for one day.
Follow Up:
Follow up took place in a month after the first prescription. There were no pains in the stomach during this month. Stool became more formed, once a day, though belching remained the same. During palpation in the epigastric region and in the right hypochondrium, tenderness was still there.
Prescription was: Asafoetida 200C – 5 globules in solution (60 ml, three times a day with a 5-6 hour interval for one day).
In two weeks after taking the remedy, belching practically stopped. There appeared an erythematous rash on the body accompanied with itching lasting a week, which reflected the manifestation of Hering’s law of cure: “inside-out healing” and “from more important to less important”.
1.5 months after the onset of therapy there was a relapse of stomach pains with single-shot vomiting. The parents called an ambulance and the child was hospitalized. Soon after discharge from the hospital, belching occurred again and tended to recur with the same frequency (after each meal), but its volume was significantly reduced. Heartburn was noted once in a while, stool was devoid of undigested admixtures, though frequently pale, loose and fatty. Two months after the onset of therapy, the child developed an acute respiratory infection, with temperature rising to 38 °C, headache and photophobia.
Belladonna LM (Q) X was prescribed as an agent for treating the acute, 5 globules in solution (per 100 ml, a table spoon every 30 min three times). The temperature started decreasing, the headache was gone and the child fell asleep to wake up the next morning feeling well.
In 4 months since the onset of therapy, belching occurred more frequently again. Stool was closer to a seedy one, loose, but not foul-smelling and without pathological admixtures and periodically it could be fatty. There was a relapse of heartburn 1-2 times a week. No stomach pains during the last 2.5 months.
The child received Asafoetida 200C – 5 globules as a single dose. Further on, the patient received Asafoetida 200C several times, with a 2-3 month interval, when the symptoms (heartburn and seedy loose stool) recurred. When the subsequent dose of Asafoetida 200C produced no effect, Asafoetida 1M, 5 globules as a single dose, was prescribed.
During the next (second) year of follow-up there were three acutes. One of them was mild and required no therapy, the second one manifested as febrile fever (the child received Belladonna LM (Q) X with good effect). The third acute state was characterized by lacunar tonsillitis (this disease was recorded in his anamnesis two times, at 1 and 4 years of life). The child received Lycopodium LM (Q) X (pharynx hyperemic, plaqued right tonsil, thirst quenched with frequent small gulps of water) and recovered within a few days. Following each acute state, the patient’s main pathology aggravated and he received Asafoetida 200C, 5 globules in a single dose every time.
There were a few more short-term episodes of skin eruptions but without expressed pruritus. The periods of normal stool and absence of belching became considerably longer. After 3.5 years of therapy the given pathological symptoms were not observed, the child returned to health group A and got sick with acute respiratory infection just one time a year, in a light form and without a considerable rise in temperature.
The follow-up of the case is 5 years. It demonstrates a success in the application of a remedy rarely used in homeopathic practice.The patient’s recovery is in compliance with Hering’s law of cure and return to a higher level of health (Group A).