
Abstract
New Zealand and Australia have the dubious honour of experiencing one of the highest incidences of skin cancer. Their conventional treatment is often painful, mutilating and expensive. I present a “do-it-yourself” local technique for treating basal cell carcinomas that is simple, cheap, pain-free, based on scientific evidence and that does not interfere with any other treatment that could be needed in the future.
Introduction
Basal Cell Carcinomas (BCC) are the most common skin cancers (Homeopathy Treatment for Skin Cancer) originating in the epidermis. Basal cell carcinomas originate in the basal layer of keratinocytes, which is the deepest cell layer of the epidermis. Squamous cell carcinomas (SCC) stem from the more superficial layers of keratinocytes. Based on their histology, the lesions called Actinic Keratosis appear to be early stages of Squamous Cell Carcinoma (1). Sun exposure with cumulative effect, old burns scars, ultra-violet exposure as in tanning beds and PUVA therapy for psoriasis, local radiotherapy, arsenic exposure and smoking are all considered as etiological factors in the appearance of those skin cancers.
BCCs are classified as nodular, infiltrative, superficial apparently multifocal and mixed in terms of growth pattern. They remain local, rarely if ever metastasize but can become enormous in size and ulcerate, giving a picture of “Ulcus Rodens” (eroding ulcer). SCCs do metastasize in around 4% of cases, but otherwise seem to have the same aetiology and the same local behaviour. Here is a more detailed classification of BCC for those who are interested:
- Nodular basal-cell carcinoma(Classic basal-cell carcinoma)
- Cystic basal-cell carcinoma
- Cicatricial basal-cell carcinoma
- Infiltrative basal-cell carcinoma
- Micronodular basal-cell carcinoma
- Superficial basal-cell carcinoma
- Pigmented basal-cell carcinoma
- Rodent ulcer(Jacobi ulcer)
- Polypoid basal-cell carcinoma
- Pore-like basal-cell carcinoma
- Aberrant basal-cell carcinoma
Presentation
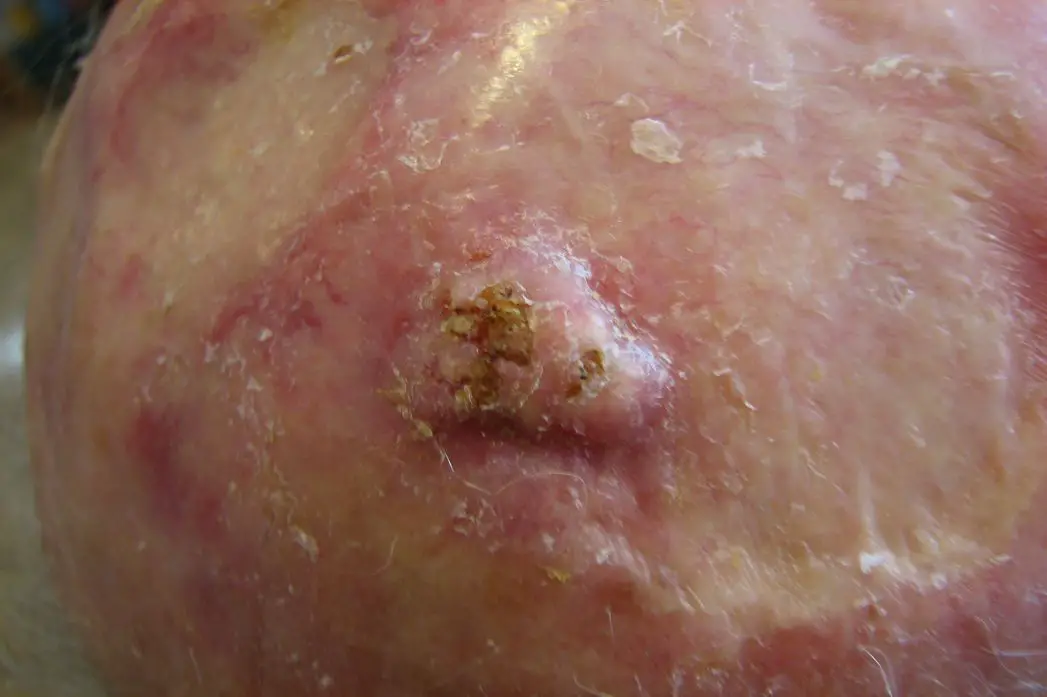
I saw this patient, an elderly gentleman in his eighties, in 2005, when he accompanied his wife for a treatment. It took him some time to ask if I would like to try treating him. The situation is that of recurrent scalp BCCs and SCCs secondary to, according to him, local UV therapy in his youth to “re-grow hair” (most probably rather Radiotherapy for Tinea Capitis). The patient gave verbal consent to use the pictures for publication at the original consultation.
As seen in the picture, he has undergone multiple resections and plastic procedures, the last one a few weeks ago for a huge bleeding tumour. A general treatment (homeopathy, herbs, nutritional supplementation, etc.) was unsuccessful due to compliance problems as well as the cancers having become independent entities, not under the control of the body’s immune system any more. There was a need to control the local growth. The patient agreed to try what was then an experimental treatment and to have the results published.

Picture taken 10.1.2006.
A close- up picture:

After 2 weeks of treatment, 26.1.2006:


The scalp is cleaner, small lesions have disappeared.
14.2.2006:


The amelioration continued until the main lesion covered itself with a horny layer, preventing contact with the local treatment.
22.3.2006:


Note the rest of the scalp has apparently cleared. This resistance was overcome by using the blistering ability of local fresh garlic applications that destroyed the superficial layer and allowed the local treatment to penetrate again. The garlic was left in place for only a few hours as this patient’s lesions were known to bleed easily and profusely.
19.4.2006:
23.5.2006:
15.6.2006:

23.8.2006:

10.10.2006:

It took about 9 months to completely clean the skin. Because of the aetiology of irradiation, which is a lot more harsh and intense than sun exposure, lesions kept coming back but were immediately taken care of as soon as they appeared, with the same treatment. The local applications never covered the whole scalp, therefore were not dealing with the Cancer Stem Cells (CSC) that were apparently disseminated inside the scalp due to the widespread irradiation. There is no demonstration that this treatment can actually destroy the CSC. The clinical observation was that the recurrences happened in spots that were previously not affected, prompting me to suggest that there could be an action on the CSC; this needs of course to be investigated properly.
Unfortunately, after a couple of years being “cancer-free”, recurrences started to appear. The patient refused to go back to the natural treatment, underwent some plastic surgery procedures until what he needed was major surgery with rotation flaps taken from his back. He refused this too and was then offered local scalp radiotherapy. Soon after this treatment he started developing convulsions as a consequence of too intense brain irradiation. The convulsions evolved into coma and death.
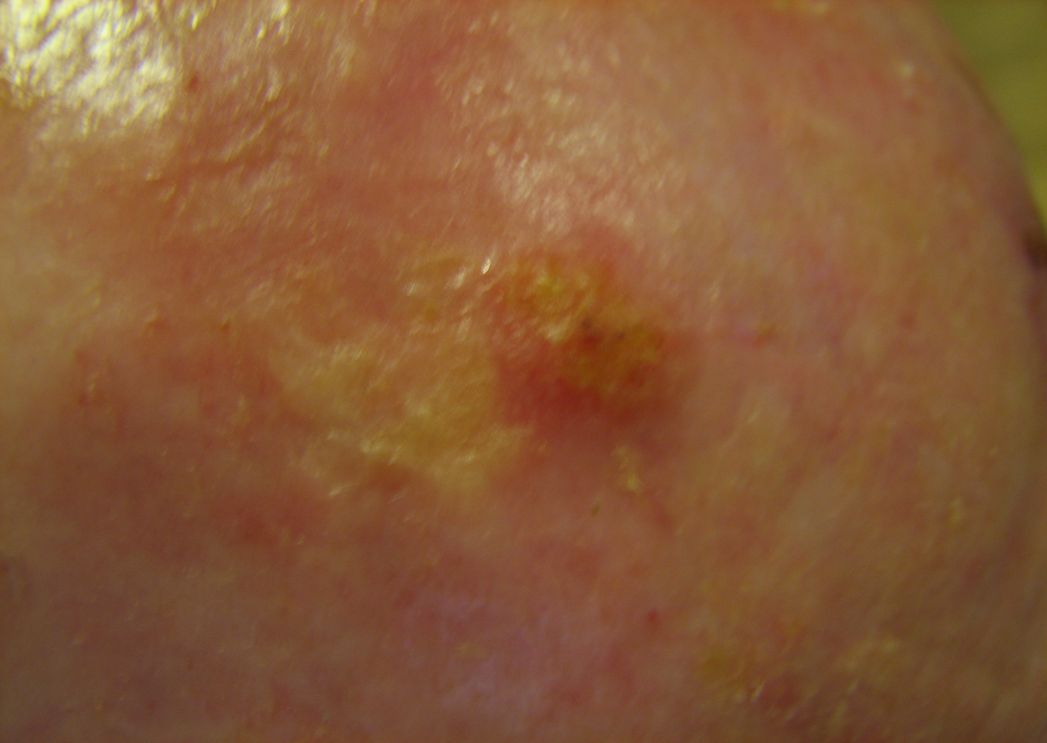
Here are the results for a few other patients. All of them have given verbal or written consent to use and publish their pictures.


This lesion disappeared completely after 5 months of treatment.



Three months between those pictures, quite a resistant one, but still evolving in the right direction.


Three weeks between those pictures!
Once a treatment has been started, it should be done properly and at least 3-4 weeks until the lesions cannot be seen or felt in order to destroy all the cancerous cells. Otherwise we can end with a situation like this:


Four months between those pictures. The treatment was done once or twice a week in an irregular manner instead of an intensive, aggressive approach that such an extensive lesion would require. The lesion has grown and there is infiltration of the skin at the periphery of the lesion. Irritating cancer cells promotes their growth and spread, that is a known fact. The biological behaviour of a tumour should be understood and respected.
Other patients sent me written reports without pictures, describing successes. One in particular did the treatment while being on the waiting list for a Mohs procedure. Despite the lesion having regressed, the surgeon proceeded with the intervention, instead of waiting and encouraging the patient to continue with “whatever she was doing”; and to everybody’s surprise (!), could not find any cancer cell anywhere. Many people indicated they were starting the treatment but did not report further. Therefore I do not have a statistically valid series of cases. Nevertheless, this treatment is working and has many advantages as we will see.
The remedy.
What is this natural, topical remedy?
Brassica Oleracea var Botrytis
Better known as Broccoli. Family of Brassicacea, formerly known as Cruciferacea or Mustards, family of cabbages, cauliflower, Brussels Sprout.
According to John Boik (2), the Brassica family contains those carcinogenesis inhibitors specific to the cruciferous plants:
- Agents that block carcinogen activation: Aromatic isothicyanates and Glucosinolates (glucobrassin, glucotropaeolin)
- Agents that increase carcinogen detoxification: Aromatic isothiocyanates
- Agents blocking the action of tumour promoters: Aromatic isothiocyanates, Dithiolethiones, Indoles, Phenols
- Supressing agents: Aromatic isothiocyanates
- Indole 3 Carbinol (I3C) causes apoptosis and prevents spread (3)
- I3C and Genistein increase the amount of BRCA 1 & 2 in cells preventing the transmission of damaged genetic material in next cellular generation (genetic relative deficiency).
- Sulforaphane inside the broccoli cells inhibits the oxidizing enzymes that damages DNA (New Scientist)
Sulforaphane is the most studied and best known broccoli-specific agent, also found in all the other Cruciferacae. The mechanisms of action are diverse and well studied. Even though many of those imply internal use of broccoli, I decided to use it locally so that an extremely high concentration could be achieved. Sulforaphane is an organosulfur substance that has anti-cancer, and antimicrobial properties in. The enzyme myrosinase transforms glucoraphanin, a glucosinolate, into sulforaphane upon damage to the plant, akin to the appearance of allicin when garlic is crushed. Young sprouts are particularly rich in glucoraphanin and can be used instead of the vegetable. I have actually started recommending using the sprouts as they are available year long and are easier to prepare than the florets.
Vegetables and especially Cruciferacae induce enzymes of xenobiotic metabolism and thereby accelerates the metabolic disposal of xenobiotics. Induction of phase II detoxication enzymes, such as quinone reductase and glutathione S-transferases in rodent tissues affords protection against carcinogens and other toxic compounds. Sulforaphane is the most potent inducer, and the presence of oxygen on sulfur enhances potency. “Sulforaphane and its sulfide and sulfone analogues induced both quinone reductase and glutathione transferase activities in several mouse tissues. The induction of detoxication enzymes by sulforaphane may be a significant component of the anticarcinogenic action of broccoli.” (4). It also induces apoptosis, “suicide” of cancer cells (5). And it has been shown to act on telomerase activity, which is an essential component of aging and cancer induction (6).
One study used local broccoli extract, but this was done with boiling and chemical extraction, making it a pharmaceutical substance rather than a natural one:
“Topical application of sulforaphane-rich extracts of 3-day-old broccoli sprouts up-regulated phase 2 enzymes in the mouse and human skin, protected against UVR-induced inflammation and oedema in mice, and reduced susceptibility to erythema arising from narrow-band 311-nm UVR in humans. In six human subjects (three males and three females, 28–53 years of age), the mean reduction in erythema across six doses of UVR (300–800 mJ/cm2 in 100 mJ/cm2increments) was 37.7% (range 8.37–78.1%; P = 0.025). This protection against a carcinogen in humans is catalytic and long lasting.” (7).
It also works by down-regulating the DNA methylation of genes controlling cancer occurrence, sulforaphane acting as HDAC or histone deacetylase, an epigenetic mechanism (8). There are many studies that have investigated the mechanism of action of sulforaphane (see References). There is no doubt whatsoever that this is a potent tool in the treatment (and prevention) of all cancers.
Discussion
The purpose of using a topical application, as mentioned above, is to achieve a very high concentration of active components at the tumour location that would otherwise not be possible or practical. Even though those skin cancers are seen as local events, it is absolutely essential in my opinion to add the general approaches of lifestyle and nutritional changes, homeopathic and herbal general treatments according to every practitioner’s knowledge. The presence of a cancer, even caused by a clear local injury, means that the immune defence system has been overcome or bypassed; it has to be restored to normal to avoid recurrences or the appearance of deeper, more aggressive pathologies. This method as presented here involves the patient in his treatment 100% as he fully controls what he is doing; it is also simple, cheap and effective while being pain free and not aggressive towards normal tissues. This fits perfectly with my personal philosophy of “Power to the people”.
We used the florets of the broccoli, but now have switched to the sprouts. Both contain the highest concentration of active substances, the sprouts being the most effective. The original recommendation was to juice them so that the cells are broken and the maximal amount of sulforaphane is produced. Some juicers cannot manage the small florets or the sprouts and many patients do not have a juicer or cannot afford to buy one. One patient solved this problem by using a mortar and pestle until the plant was reduced to an extremely wet pulp with a pasty, mushy, consistence: it worked very well and has worked well with other patients. Once the juice is extracted, if using a juicer, it is mixed with the dry pulp until a wet, almost dripping, “mush” is created. This is so that all the active substances are available. We tried to use the juice with gauze or cotton balls instead of the dry pulp; the activity was reduced to almost nil. I attribute this to adsorption on the gauze/cotton fibres. The “mush” is generously put on the lesion and covered with a cling film (saran wrap, glad wrap) that prevents the liquid from escaping and increases the local concentration. It is then covered in any practical way possible, depending on the location of the BCC. Ideally, this should be changed every few hours to ensure a permanent saturation in active components. This of course is not always possible. Leaving it overnight and changing the dressing during the night if waking up is a practical and effective method. The juice or mush has to be prepared fresh every time. Keeping it in the fridge is tempting; the activity of the preparation diminishes in time and might not be effective after a few hours, hence the need to change the application as often as practical with freshly prepared broccoli. The plant itself does not need to be freshly picked (active substances are mainly intracellular) or be organic: plain, cheap supermarket broccoli works very well.
If the lesion seems to burrow into the skin or to be covered with a thick layer that prevents contact with the juice, a short application of a slice of fresh garlic or some crushed one will solve that problem. Care should be taken not to leave the garlic too long as it has blistering properties (that is why we use it in this indication) and can cause pain. The good news is that it has also local anti-cancer properties and its use will not slow the treatment.
The different and multiple actions of the active components are active only on cancer cells and leave the normal tissues totally unharmed, and unstained. This very selective destruction allows the normal tissues to replace the dead cancerous cells “on the go” and prevents any scarring. There should be no pain and no bleeding unless the cancer cells have invaded locally a nerve or a vessel. If any local pain appears, it will resolve without any interference and so far I have not received any report saying otherwise or needing any type of intervention. In one single case of scalp BCCs in a gentleman in his sixties following multiple sunburns in adolescence and adulthood, the first application of broccoli gave the expected results. After the emergence of new lesions and repeated treatment, two phenomena emerged: first, the whole area became red and inflamed while the BCCs were quickly destroyed and replaced by ulcers, leading to the need to stop the treatment after about a week, followed by a full healing; second was the appearance of small BCCs in the same area during the treatment, which disappeared within a few days. The patient being otherwise completely healthy and with a very strong immune system, I interpret the reactions as a systemic assault of the immune system on the cancer cells that became recognisable as being pathological once weakened by the treatment. At the same time, the CSCs were stimulated (unproved assumption), started multiplying and were immediately destroyed by the combination of the local treatment and the immune defences. An experimental application of the broccoli on other spots not suspect of harbouring CSCs did not produce any reaction. This emphasizes the need for simultaneous immune-stimulant treatment as well as general core homeopathic treatment, which was the case for this patient.
Bleeding is controlled by local pressure, as no major vessel should be involved. This is an important difference and advantage over “black salves”, the escharotic treatments, the local chemotherapy, the local radiotherapy and of course surgery: all of them are not selective, destroy all the cells indiscriminately, are often painful and leave scars that are sometimes mutilating. For the same reasons, this treatment does not work on benign, non cancerous lesions (tried) and on warts (tried). Once a treatment has been started, it is recommended to continue until at least 3-4 weeks after the visible or palpable lesion has disappeared, to insure each and every single cancerous cell has been destroyed. This time is a “guesstimate” of course, but also a safety measure. Last but certainly not least, it is simple and cheap, no special skills are needed except some help at the beginning to learn how to dress the spot when in an awkward location. And it cannot be patented, although I have seen some (expensive) creams and ointments containing broccoli extract: I challenge the real activity and the concentration of those preparations.
Inevitably, some lesions will be resistant to the topical treatment. Within the same line of reasoning, but without any clinical concrete results yet, I have suggested to replace the broccoli with either green tea or turmeric. The green tea could be a tea bag barely wetted so that no drinking tea is made but wet enough to have the fluid slowly escape; the turmeric should be of excellent quality (which is always a problem) and made into a paste. That paste should be oily as curcumin, the active ingredient of turmeric, is lipid-soluble and will be more available if oil or fat is used. I suggest the use of coconut oil as it also has some anti-cancer properties; the drawback is that it becomes liquid at body temperature and might spill out of the local dressing. One option is also to rotate those three different plants so that as many active ingredients as possible are put into contact with the tumour.
Extending this practice to locally reachable lesions, I can imagine, but have not yet had the opportunity to do so, using this method for cervical cancers or lower rectal cancers. One theoretical advantage is that the active ingredients would also be absorbed using the same lymphatic and venous pathways that metastases use, allowing for their treatment with high local concentration, in parallel with a general treatment. A direct herbal treatment towards liver metastases or even liver cancer, bypassing the digestive system via the portal system, is also an extension of this method. For the time being, I would not mix those three different herbs in one single “poultice” as I do not have any idea whether the ingredients would react, precipitate, become inactive or on the opposite would potentiate each other. I will leave this research to phytopharmacologists who have access to laboratory equipment.
Conclusion
A natural topical treatment for some skin cancers has been presented. It is simple, cheap, effective, based on research and scientific experimentation, painless and non-mutilating, and is deprived of side-effects. It totally involves the patient in his own care and in case of failure does not in any way prevent the application of other treatments. It should be the first choice, but also accompanied by a general, deeper treatment. It was not tested on any skin melanoma.
References
- Ortonne JP. From actinic keratosis to squamous cell carcinoma. Br J Dermatol. 2002;146(suppl 61):20–3;
- Cancer and Natural Medicine. ISBN 0-9648280-0-6
- Nat. Cancer Insitute, Cancer Research
- YUESHENG ZHANG. Proc. Natl. Acad. Sci. USA Vol. 89, pp. 2399-2403, March 1992 Sulphoraphane, a naturally occurring isothiocyanate induces apoptosis in breast cancer cells by targeting heat shock proteins.
- Sarkar R, Mukherjee S, Biswas J, Roy M. Biochem Biophys Res Commun. 2012 Oct 12;427(1):80-5. doi: 10.1016/j.bbrc.2012.09.006.
- Moon DO, Kang SH, Kim KC, Kim MO, Choi YH, Kim GY. Department of Marine Life Sciences, Jeju National University, Republic of Korea. Sulforaphane decreases viability and telomerase activity in hepatocellular carcinoma Hep3B cells through the reactive oxygen species-dependent pathway. Cancer Lett. 2010 Sep 28;295(2):260-6. Epub 2010 May.
- Sulforaphane mobilizes cellular defenses that protect skin against damage by UV radiation Paul Talalay,†‡Jed W. Fahey,†§ Zachary R. Healy,† Scott L. Wehage,† Andrea L. Benedict,† Christine Min,† and Albena T. Dinkova-Kostova†¶ Proc Natl Acad Sci U S A. 2007 October 30; 104(44): 17500–17505. Published online 2007 October 23. doi: 1073/pnas.0708710104
- Promoter de-methylation ofcyclin D2 by sulforaphane in prostate cancer cells Anna Hsu1,2, Carmen P Wong1,2, Zhen Yu3, David E Williams2,3, Roderick H Dashwood2,3and Emily Ho1,2*. Clinical Epigenetics 2011, 3:3
More references from www.Pubmed.com.
1.Gene expression profiling following NRF2 and KEAP1 siRNA knockdown in human lung fibroblasts identifies CCL11/Eotaxin-1 as a novel NRF2 regulated gene.
Fourtounis J, Wang IM, Mathieu MC, Claveau D, Loo T, Jackson AL, Peters MA, Therien AG, Boie Y, Crackower MA.
Respir Res. 2012 Oct 12;13(1):92.
2.Sulphoraphane, a naturally occurring isothiocyanate induces apoptosis in breast cancer cells by targeting heat shock proteins.
Sarkar R, Mukherjee S, Biswas J, Roy M.
Biochem Biophys Res Commun. 2012 Oct 12;427(1):80-5.
3.Sulforaphane inhibits the Th2 immune response in ovalbumin-induced asthma.
Park JH, Kim JW, Lee CM, Kim YD, Chung SW, Jung ID, Noh KT, Park JW, Heo DR, Shin YK, Seo JK, Park YM.
BMB Rep. 2012 May;45(5):311-6.
4.Effect of broccoli sprouts on insulin resistance in type 2 diabetic patients: a randomized double-blind clinical trial.
Bahadoran Z, Tohidi M, Nazeri P, Mehran M, Azizi F, Mirmiran P.
Int J Food Sci Nutr. 2012 Nov;63(7):767-71.
5.Effect of phytochemicals on phase II enzyme expression in infant human primary skin fibroblast cells.
Warwick E, Cassidy A, Hanley B, Jouni ZE, Bao Y.
Br J Nutr. 2012 Mar 19:1-8.
6.Phase 2 enzyme inducer sulphoraphane blocks prostaglandin and nitric oxide synthesis in human articular chondrocytes and inhibits cartilage matrix degradation.
Kim HA, Yeo Y, Jung HA, Jung YO, Park SJ, Kim SJ.
Rheumatology (Oxford). 2012 Jun;51(6):1006-16.
7.Protective effect of sulphoraphane against oxidative stress mediated toxicity induced by CuO nanoparticles in mouse embryonic fibroblasts BALB 3T3.
Akhtar MJ, Ahamed M, Fareed M, Alrokayan SA, Kumar S.
J Toxicol Sci. 2012 Feb;37(1):139-48.
8.Myrosinase hydrolysates of Brassica oleraceae L. var. italica reduce the risk of colon cancer.
Hashem FA, Motawea H, El-Shabrawy AE, Shaker K, El-Sherbini S.
Phytother Res. 2012 May;26(5):743-7.
9.Sulphoraphane enhances aquaporin-4 expression and decreases spinal cord oedema following spinal cord injury.
Mao L, Wang HD, Pan H, Qiao L.
Brain Inj. 2011;25(3):300-6.
10.Sulphoraphane inhibited the expressions of intercellular adhesion molecule-1 and vascular cell adhesion molecule-1 through MyD88-dependent toll-like receptor-4 pathway in cultured endothelial cells.
Shan Y, Lin N, Yang X, Tan J, Zhao R, Dong S, Wang S.
Nutr Metab Cardiovasc Dis. 2012 Mar;22(3):215-22.
11.Comparison of the protective effects of steamed and cooked broccolis on ischaemia-reperfusion-induced cardiac injury.
Mukherjee S, Lekli I, Ray D, Gangopadhyay H, Raychaudhuri U, Das DK.
Br J Nutr. 2010 Mar;103(6):815-23.
12.Molecular crosstalk between TRAIL and natural antioxidants in the treatment of cancer.
Rushworth SA, Micheau O.
Br J Pharmacol. 2009 Aug;157(7):1186-8.
13.Phase 2 enzyme inducer sulphoraphane blocks matrix metalloproteinase production in articular chondrocytes.
Kim HA, Yeo Y, Kim WU, Kim S.
Rheumatology (Oxford). 2009 Aug;48(8):932-8.
14.Isothiocyanates sensitize the effect of chemotherapeutic drugs via modulation of protein kinase C and telomerase in cervical cancer cells.
Mukherjee S, Dey S, Bhattacharya RK, Roy M.
Mol Cell Biochem. 2009 Oct;330(1-2):9-22.
15.Epithiospecifier protein activity in broccoli: the link between terminal alkenyl glucosinolates and sulphoraphane nitrile.
Williams DJ, Critchley C, Pun S, Nottingham S, O’Hare TJ.
Phytochemistry. 2008 Nov;69(16):2765-73.
16.Evaluation of the antimicrobial effects of several isothiocyanates on Helicobacter pylori.
Haristoy X, Fahey JW, Scholtus I, Lozniewski A.
Planta Medorrhinum 2005 Apr;71(4):326-30.
17.Identification of a novel Nrf2-regulated antioxidant response element (ARE) in the mouse NAD(P)H:quinone oxidoreductase 1 gene: reassessment of the ARE consensus sequence.
Nioi P, McMahon M, Itoh K, Yamamoto M, Hayes JD.
Biochem J. 2003 Sep 1;374(Pt 2):337-48.
18.High cellular accumulation of sulphoraphane, a dietary anticarcinogen, is followed by rapid transporter-mediated export as a glutathione conjugate.
Zhang Y, Callaway EC.
Biochem J. 2002 May 15;364(Pt 1):301-7.
19.Effects of dietary anticarcinogens on rat gastrointestinal glutathione S-transferase theta 1-1 levels.
van Lieshout EM, Bedaf MM, Pieter M, Ekkel C, Nijhoff WA, Peters WH.
Carcinogenesis. 1998 Nov;19(11):2055-7.
20.Selective increase of the potential anticarcinogen 4-methylsulphinylbutyl glucosinolate in broccoli.
Faulkner K, Mithen R, Williamson G.
Carcinogenesis. 1998 Apr;19(4):605-9.


That is amazing! Thanks for sharing.
This is very timely for my client with basal cell. Thank you for sharing a non-invasive tested approach that empowers the people!
Nature is very gracious. We only need to explore it for the benefit of humanity at large. If the photographs of the herbs were inserted for clear understanding by the readers of different soils, in my opinion, it would have been more gratifying. With regards – Asghar Ali
Very interesting ! What is the ” scientific ” back ground, therapeutic action of garlic paste. Do we have to use it daily and what amount.
Thanks .
I would like to know if Dr. Joe has any updates to the above treatment, please?
I followed the broccoli juice protocol as suggested in the article for two weeks. Lesion was easily accessible on the front of my leg; changed the poultice (juice plus broccoli pulp from the juicer) every 4-5 hours; did not change during the night. As a dressing, followed the suggestion of using a generous piece of plastic wrap taped around the sides. Still, there was some juice leakage and I could smell broccoli occasionally – fortunately no one else seemed to notice or was too polite to mention! Since I was already scheduled for a Mohs surgery there was an acceptable “allopathic backup plan.” Surgeon took the first layer and within 25 minutes returned to say no cancer was found. He also told me that the pathology report stated that the lesion was squamous cell. When I told my busy dermatologist that no cancer had been found, that I had treated it with broccoli juice, it was so far outside her realm that she simply shrugged and asked no questions. My acupuncturist, who is also a TCM doctor, said that the effectiveness of broccoli to cure skin issues has been well known for centuries in China. Issue is that the juice has to be fresh, and most TCM remedies are dried herbs.