In homeopathy it is often said that the patient’s symptoms should be at the centre of every case so that the homeopath can follow the vital force and find the simillimum. But what if the patient’s story and symptoms don’t make sense, and all the time there is a nagging feeling that something is missing? And what happens when homeopathy isn’t helping or makes things worse? In situations like this it is crucial to be able to think outside the box, tackle a problem from every possible angle and not give up when it gets tough. Having a homeopathic education from the Centre for Homeopathic Education provided me with an eclectic homeopathic toolbox that proved essential in dealing with patient AB who presented “simply” with an itchy skin (Homeopathy Treatment for Itchy Skin) rash. This case became a very perplexing chronic case that required a number of homeopathic methods, adjunctive approaches, as well as getting the GP and consultant interested before the final piece of the puzzle fell into place.
- Introduction
What if the patient and the case don’t make sense, and all the time there is a nagging feeling that something is missing, but you don’t know what it is? And what happens when homeopathy isn’t helping or makes things worse? In situations like this it is also crucial to be able to think outside the box, tackle a problem from every possible angle and not give up when it gets tough.
This chronic case, taken in my first year after graduating from CHE, needed every tool I had in my homeopathic tool box. While there is no doubt that other homeopaths reading this account will have chosen other remedies, asked other questions, perhaps stuck more rigidly to certain methods, I present this case as an authentic record of the reality of this case for me, showing my successes, failures and frustrations.
- Patient AB
Patient AB is female, age 70.
AB’s presenting complaint is a very itchy skin rash. AB has suffered with this rash for 4 years following what she believed was exposure to an environmental toxin in a rented house. The itching started on her legs, then arms, torso, around her waist and bra straps and more recently has progressed to around her eyes. It comes and goes with varying degrees of severity; it feels tingly and prickly before the itching starts. Very often AB’s skin is only slightly red with little visible evidence of the itch. The only amelioration for the itch is a hot bath but the itch is worse afterwards; AB also finds great relief in scratching: “scratching overcomes everything”. Since the rash developed AB has felt unable to sweat and she feels like her head is swollen.
AB was seeing, and continued to see, a NHS dermatologist throughout our consultations: he had been unable to offer AB anything to alleviate the itch other than antibiotics and steroids. On my advice after our first consultation AB changed to a smaller dose of junior antihistamine and all natural moisturisers, particularly Aloe Vera: the dermatologist was supportive of these changes. I encouraged her to take an Epsom salts bath twice weekly and change her usual massage treatments for lymphatic drainage.
Despite investigations and medical monitoring, no conventional diagnosis for the itchy skin rash had been given. AB’s GP considered Lichen Planus and Lupus but no confirmation was achieved.
Otherwise, she is generally healthy; she is still working part time in a cash office, where she is a worrier and a perfectionist. AB enjoys an outdoor life, loves horses and dogs, is very practical in both her manner and dress, doesn’t like summer, never feels cold, is vegetarian and has a fear of unseen loud noises like thunder. She has low self-esteem and doesn’t get angry; instead she ‘retreats’ and ‘goes quiet’. She appears very confident but assures me that she is not.
Family medical history revealed some asthma and bronchitis on both sides of AB’s family, and AB’s son has mild eczema and hayfever. No other strong medical patterns were identified.
- To begin: Constitutional Approach
After my first appointment with her I took a classical approach. The mental and emotional aspects of the case could have taken priority in my case analysis but AB appeared to be so together and accepting of her situation I did not perceive that her vital force was too perturbed: she seemed healthy and dynamic.
I prescribed Calcarea sulph. based on Scholten’s description of the remedy1. In addition to the Calcarea sulph I also decided to give AB an anti-miasmatic intercurrent remedy, namely Psorinum, based on Fraser2 where he describes “a terrible itch, worse at night and worse in the heat”. I considered Sulphur as a possible remedy for the Psoric miasm, but Psorinum seemed more appropriate based on the suppression of the itch with antibiotics and steroids. I clarified my choices using Prisma3 and Phatak4 materia medica.
28 Aug 2012- Calcarea sulph. 200c (one a day for five days, week one and three) and Psorinum 30c (one, morning and evening, week two and four).
One month later AB said that she was now itching all over, but felt better in herself. As a homeopathy student we were told that improvements often come from the centre of the patient first so I was encouraged that AB felt better in herself, even though her itching had worsened.
1 Oct 2012 – Rhus tox.200c, morning and evening for two days. This was a therapeutic prescription based on the match between the modalities of Rhus tox.5 and AB’s rash; I also wanted to give the previous remedies time to continue to act.
Two weeks after the Rhus tox. AB’s itchy rash had not responded to the remedy. AB also now felt that the hot baths were no longer helping alleviate the itch and she preferred cold. I therefore changed remedy to Apis mel. given the new information. Specifically, < warm room, < evening, dryness, < on perspiring parts, allergic looking eruptions, < in warm bed, sensation head swollen, active and busy patients, hot applications agg, scratching amel, urticaria5.
15 Oct 2012 – Apis mellifera 200c, morning and evening for three days.
AB still failed to react to the remedies and nothing about the itch changed.
- Next: a deeper understanding and miasmatic activity
After the first few appointments with AB we had established a good relationship which helped us explore the mental and emotional aspects of her case more fully and I built a deeper understanding of her life and history.
AB’s childhood contains several significant events but her lack of deep emotional response to them was interesting from a homeopathic perspective. AB was brought up by her older brother after their mother died when AB was 6; AB knows little about the death. AB’s aunt was to take care of her but was killed in a car accident. AB’s father re-married to a “wicked” woman so AB spent many years as a step-child being told she was worthless. AB left home before she turned 18.
AB was married for 30 years and thought the marriage was a good one. However, her husband was unfaithful and left. They did not argue about the affair: AB just covered her ears and never spoke to him again. They have been separated for more than 20 years now, but AB refers to him affectionately in the present tense saying “he is my best friend”.
AB cannot face confrontation and does not make friends easily. She believes many things are her fault (+++), including the loss of her mother and husband. AB is extremely nostalgic and in her retirement has moved to the area where she went for childhood holidays.
From this improved insight, I knew that I needed to change my prescribing strategy, so I decided to move away from the aetiology and moved towards the emotional centre of the case. I also moved away from the Psoric miasm as it became clear that the Carcinogenic miasm was highly active in her lifelong emotional suppression, as well as her physical suppression of the itch2,3.
In addition to the decision to prescribe on an active miasm I felt that AB had not exhibited a normal ‘shock’ reaction to much of the loss and grief in her story and this blocked shock could perhaps be an obstacle to cure so needed treatment too.
30 Oct 2012 – Aconitum napellus 10M single dose followed three days later by Carcinosin 1M, one morning and evening.
- Next: Aggravation
In response to the October prescription AB said she felt no change after taking the Aconitum napellus but shortly after taking the Carcinosin AB had a truly horrifying aggravation, the likes of which I never anticipated.
AB had a headache for the first two days after taking the Carcinosin, then she was extremely shivery (++++) and the rash had moved all over her body and become severe. The rash was intensely itchy, like shooting pain in her legs and it oozed pus over her entire body. Her face, neck and arms were ‘velvety’ and slightly swollen. She was unable to sleep and ached all over; her urine turned orange. Upon further questioning, AB said that she had previously experienced these severe symptoms about a year ago and had been given high doses of steroids. If this was a return of old symptoms in response to the Carcinosin I was horrified.
Despite the severity of the aggravation AB persevered with homeopathy and followed my advice to dilute the Carcinosin 1M in a glass of water, stir gently and take one teaspoon a couple of times a day. I advised this course of action based on the standard CEASE6 protocol when a detox aggravation happens. I also advised topical calamine lotion/aloe vera and cool salt water baths, which she did four times a day. A lesser patient would be reaching for some steroid cream!
In terms of case and personal management, AB’s aggravation was a very challenging and stressful time: members of AB’s family were telephoning to express their concern and I have to admit I was very worried too. The support group I had gained from my CHE year group, other local homeopathic practitioners and supervision were all very important.
I called AB daily and explained the homeopathic principle of a ‘reaction’ to remedies being a positive thing. We discussed how she had opened up to me emotionally and that she was now throwing a very effective fever. I genuinely believed she had aggravated due to her lifelong history of emotional suppression and that the appearance on the skin was an indicator that she was healthy and there was no deeper pathology.
- Next: aggravation recovery
As soon as AB was able to she came to my clinic. Her body was covered in raw wheals and she was in severe pain. Her leg was completely inflamed and oozed pus (see Figure 1).

Figure 1: AB’s skin rash after a single dose of Carcinosin 1M and two weeks of low potency management of the flare-up. Date photo taken: 5 Nov 2012.
In terms of case management I was feeling at sea. With permission, I gave AB’s case to my colleagues and graduating class for their input and advice. This was invaluable support and a sharp reminder of how important working with colleagues can be, especially in a profession that is often very solitary.
It was obvious that my priority for AB was now to control the aggravation and restore her symptoms to a manageable level. To do this, I chose to continue with the same remedy but at a much lower potency. I chose to use another CEASE prescribing strategy6 and work slowly back up the potency scale. Carcinosin was also clearly doing something but the potency needed adjusting and because AB appeared to be going through a return of old symptoms it was possible that this process was ‘necessary’ – although it certainly challenged my ideas of homeopathy being gentle.
5 Nov 2012 – Carcinosin 30c single dose orally
10 Nov 2012 – WAIT
16 Nov 2012 – Carcinosin 30c single dose orally
20 Nov 2012 – Carcinosin 30c single dose orally
Thankfully, AB was supportive of my efforts to calm the aggravation and she continued to believe in homeopathy: she believed that homeopathy would find a solution to her skin rash. This expectation weighed heavily on my mind: her case was like no other case I had seen or handled previously and things just did not make sense to me the way I had come to expect. In hind-sight we did have a lecture at CHE on case failures and mistakes but these case examples seemed to be so unusual that as a student I simply did not believe that it would ever happen to me.
Thankfully, towards the end of November 2012 AB was exhausted, but sleeping very soundly and sweating (+++) for the first time in a number of years: “I am dripping”; “I feel like I’m being steam cleaned”.
- Next: watching the subtle shift and a lesson in being patient
As the horrendous aggravation subsided AB began to tell me about her difficult relationship with her children: this was to become a key element of the case. AB was aware that she did not know how to ‘mother’ as she had never been mothered, having been brought up by her older brother.
24 Nov 2012 – Carcinosin 30c single dose orally
3 Dec 2012 – Carcinosin 30c – every other day orally
With the repeated prescriptions I was struggling to remain patient and I was continually telling myself that AB was working through the remedy and that all would be well in time. AB’s itching was back to ‘normal’, with ‘normal’ being exactly where she was before she started homeopathic treatment: I had taken her to hell and back just for her symptoms to return to baseline.
17 Dec 2012 –WAIT
By mid-December AB had lost most of her body hair. The hair on her head was also now very dry. Her skin was ‘velvety’ (++++) and sensitive.
24 Dec 2012 – WAIT
In the New Year I decided to increase the potency of the Carcinosin to keep the case moving towards improvement.
3 Jan 2013 – Carcinosin 200c single dose orally
In response to the increased potency AB felt “awful” and was terrified that she was going backwards again: she was extremely itchy and very disappointed.
7 Jan 2013 – WAIT
14 Jan 2013 – WAIT
In mid-January I decided to change potency scales to LM preparations as I had been taught at CHE that this was a much more gentle approach to a deeply set disturbance in the vital force than the centesimal potencies. However, I was still not convinced that I really had a solid grasp on what was happening to AB and why – something still did not seem to fit.
28 Jan 2013 – Carcinosin LM1 taken as pillules, one daily
In response to the LM1 Carcinosin preparation AB felt awful again, and was beginning to despair. Her nails had become ridged and brittle. She was shivery, felt cold and damp (although she was hot to touch), and itchy (++++): “My thermostat is not right”.
These new symptoms matched the remedy Calcarea carb.3,5, so, alongside the Carcinosin LM1 I also added a prescription of Calcarea carb. 30c.
At the same time I was struggling to know how to move AB forward emotionally, now that I knew how emotional her case really was and how suppressed her responses to life events had been. I did not feel that I was bringing out the issues that needed to be dealt with and that the remedies may have been trying to bring to the surface: AB agreed to see a counsellor.
18 Feb 2013 – Carcinosin LM1 taken as pillules, one daily; Calcarea carb. 30c, one every 4 days.
AB felt the cold sensation lift after taking the Calcarea carb. and she was no longer shivering. The counsellor that AB was seeing also felt there was a link between her skin symptoms and her emotional state. In particular, during February, AB talked a lot about her daughter who visited unexpectedly and when she left AB “itched like mad”.
12 Mar 2013 – continue Carcinosin LM1 until the end of March.
25 March 2013 – AB was feeling better and had experienced a continual improvement all week.
- Next: reanalysis of the case and revisiting the margins
I questioned AB further about her past. She told me that she had tried to buy the house she was born in. AB stated that she did not want anyone at her funeral and that she has already started preparing boxes of things to leave for her children. AB also spoke more of her marriage: she did not want anyone else at her wedding – “only us”.
Was I getting stuck in my thinking? Was Carcinosin really the simillimum? Was she really simply going through a return of old symptoms? What was her vital force trying to tell me? At this stage in the case I chose to go right back to the beginning and treat AB afresh, as if she were a new patient. Following a full repertorisation (done manually, see Figure 2), Natrum mur. was the top remedy choice.
1 April 2013 – Natrum mur. 30c, one daily for 3 days.
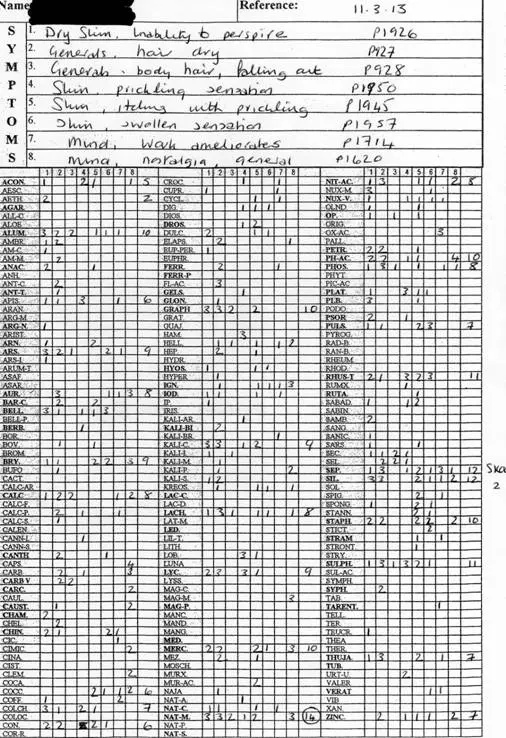
Figure 2: Manual repertorisation of AB’s symptoms. The remedy Natrum mur. was identified as the top remedy choice, scoring 14 and covering 6 of the 8 rubrics. Rubrics were selected from Murphy’s Repertory, 3rd edition.
The plan was to increase the Natrum mur. dose gently without going to a higher potency too early and risking the return of the awful symptoms again, especially given the similarity in emotional themes between Carcinosin and Natrum mur. This was a cautious approach to potency selection and did not reflect the usual rule of thumb that the more the remedy and case match, the higher the potency7.
8 April 2013 – Natrum mur. 30c, one, morning and evening.
AB felt ‘really bad’ after taking the remedy and her skin went bright red and the itching worsened.
12 April 2013 – WAIT
AB continued to feel “awful”, gradually worsening over time and becoming stressed in anticipation of her symptoms returning. Interestingly, at the same time AB ended her sessions with the counsellor, indignant that the counsellor had suggested her home life and marriage were not happy.
With AB’s permission I once again took her case to supervision and discussed it at length with two other homeopath friends. I was perplexed: was AB’s skin angry when she was not? Why was she refusing to be angry? Was she in denial?
After another repertorisation of the case several mineral remedies were examined, but the final remedy choice was Silicea as it scored the second highest after Natrum mur. (see Figure 3).
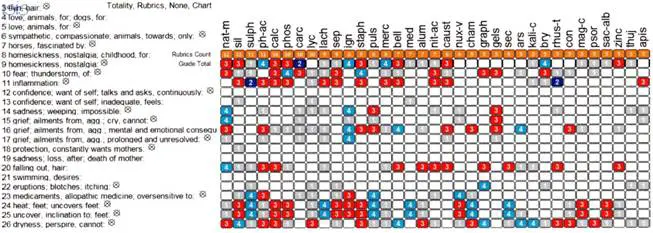
Figure 3: Computerised repertorisation of AB’s case (using ISIS software) after her responses to Natrum mur.: Silicea was the second highest scoring remedy to be identified.
14 May 2013 – Silicea 200c single dose, orally
At this time I wanted to explore if AB and her children could reconnect with the hope that this might heal some emotional tensions and triggers. However, between appointments AB’s daughter telephoned to fill me in on her version of her up-bringing. I used the new information to frame questions at my next appointment with AB: it was easy to see how the same events could create a mismatch from AB and her daughter’s perspectives so, without revealing that AB’s daughter had telephoned, I gave AB ‘homework’. That is, I asked her to try to connect with her daughter in particular ways and see what kind of response she got and to see how it made her feel.
In response to the first Silicea 200C AB felt different for 2 days then reverted back to ‘normal’ so I chose to repeat the prescription.
17 June 2013 – Silicea 200c, single dose in water
During late June and early July 2013, AB had no more remedies and undertook a series of light therapy sessions at the local hospital. This helped alleviate the itch and the skin rash but as soon as the treatment ended her symptoms returned.
When AB came back to see me there had been a very important family breakthrough: AB had reconnected emotionally with her daughter. After telephoning me in May, AB’s daughter confessed to her mother about our conversation and they have since committed to developing more open communication: both feel they have made great progress. When I look back on this case now I realise that the only satisfaction I felt was this family breakthrough, especially considering that over a year later they have effected lasting change in their relationship.
10 July 2013 – WAIT.
- Next: shifting tactics brought new insight and GP interest
When AB came back to see me she was feeling well emotionally but her presenting complaint was still as bad as ever and her sleep was still poor. As a homeopath I had witnessed AB’s successful reconnection with her daughter but her skin was still itchy!
It was time to change tactics again and delve back into my tool box of approaches. I chose to look at AB’s skin irritation from a physiological perspective. A key indicator of liver dysfunction is itching skin so I wondered if AB’s liver was an obstacle to cure. I drew on my own interest in nutrition from a sports perspective as well as lectures we had received at CHE covering organ support and therapeutics.
6 Aug 2013 – Chelidonium 3x, twice daily for 2 weeks then once daily for 2 months.
During her routine visits to the GP and dermatologist AB told them that I was working on her liver. This information seemed to resonate and they agreed to perform a series of routine liver function tests and to consider an auto-immune component to her skin condition.
AB’s appearance was very different at our consultation six weeks later: her hair was in poor condition, her nails had developed a fungal infection, there was a faint musty smell around her, the rash was now all over her body.
AB told me that she was prepared for more change so I challenged AB to change her diet. This new nutritional approach to AB’s case was inspired by my own keen interest in nutrition. There was a growing body of evidence behind a ‘low histamine’ diet which I felt resonated with AB’s case. In particular, the enzyme diamine oxidase helps breakdown histamine during digestion and if a patient lacks this enzyme then allergy-like symptoms such as hives and urticaria can occur. The only way to test this clinically, however, is through an elimination diet.
23 Sept 2013 – advised histamine exclusion diet in addition to continuing with the Chelidonium 3x.
21 Oct 2013 – the GP advised AB that she had abnormal liver function tests and neutropenia (Figure 4). In particular, AB’s AST and ALT results were significantly outside the reference range but were steadily dropping after AB had started taking Chelidonium on 6 Aug 2013. AB’s GP encouraged her to remain on the histamine elimination diet for longer as her skin was improving slowly and she was feeling better than usual.
21 Oct 2013 – Chelidonium 30c, one daily.
AB’s rash had returned and was all over her body including her eyes and face: she was now using cortisone cream regularly.
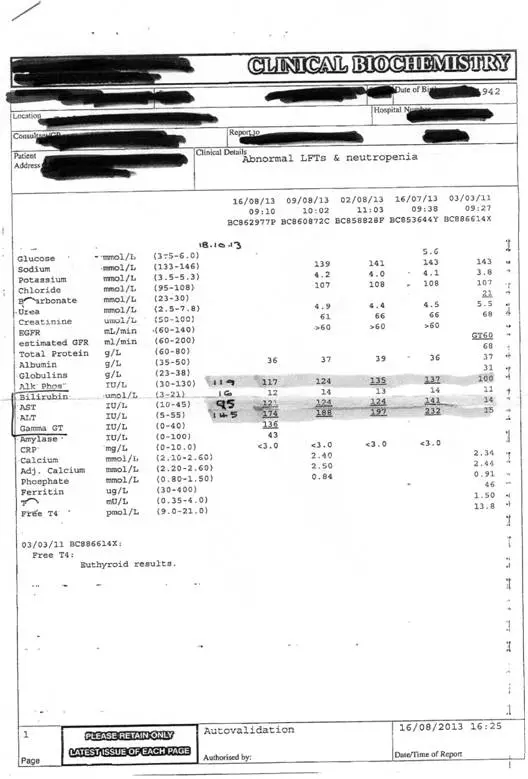
Figure 4: A copy of AB’s blood test results showing the elevated liver function tests, in particular the AST and ALT levels were significantly above the reference range in all tests performed from July to October 2013.
9 Dec 2013 – Chelidonium 30c, one daily
AB’s dermatologist asked BA to stop taking the remedies for two weeks to see if they were genuinely helping: at her next routine dermatology appointment the liver function test results worsened during the time she was not taking Chelidonium so she resumed with the original prescription. Unfortunately I don’t have this report in writing.
So what next? I was running out of ideas! I had considered the liver as a possible obstacle to cure but perhaps something else was blocking improvement? I returned to the physiological approach. In particular I reasoned that if chronic itching and gut dysbiosis are linked then perhaps the low histamine diet CW followed on my recommendation didn’t solve the problem simply because the gut flora was too disturbed. Perhaps if the gut flora could be improved the low histamine diet could help more?
Further reading highlighted that a bowel nosode might be indicated for AB: Saxton8 suggests the ‘overwhelming usefulness’ of bowel nosodes in chronic conditions and that they can be extremely useful when a number of medications have been used, and when well selected remedies fail to act. Thus, I selected Morgan Pure as the most appropriate bowel nosode for AB as it is specifically linked to chronic skin and liver conditions.
9 Dec 2013 – Chelidonium 30c, one daily and Morgan Pure 30c, on alternate days for 10 days.
CW reported no change when taking Morgan Pure 30c, but I believed it to be a good prescription and reasoned that the chronicity of AB’s symptoms warranted more time for the remedy to take effect. I therefore decided to try again with a higher potency.
15 Jan 2014 – Morgan Pure 200c, once a day for four days
In the New Year, AB was experiencing no changes on the Morgan Pure and was becoming weary, emotionally low and pessimistic; her GP prescribed SSRIs as he believed she was depressed. She was the lowest emotionally that I had ever seen her.
Using rubrics that matched AB’s current state I prescribed Pulsatilla nigiricans3. Specifically I felt that AB was < warmth, < evening, < bed, < rest, always better outdoors – “I think I’m allergic to indoors”, chilly but can’t tolerate heat.
20 Feb 2014 – Pulsatilla nigricans 200c, one morning and evening
- Finally: a diagnosis.
AB’s next appointment with her dermatologist was in April, after which she rang me: AB had been diagnosed with a form of cancer called Sezary syndrome.
Sezary syndrome is a rare cutaneous T Cell Lymphoma9. It is an advanced leukemic form of mycosis fungoides. Its aetiology and risk factors are unknown and it usually occurs in adults aged 50-60 with a slightly higher occurrence in men. Sezary syndrome manifests as extensive thin red itchy rashes over 80% of the body. There may also be changes to the nails, hair and enlarged lymph nodes. Sezary syndrome is distinguished from mycosis fungoides by the presence of malignant lymphocytes in the blood. Sezary syndrome is also very hard to diagnose even with a biopsy. Treatment can only slow the disease: there is no cure.
Looking back over AB’s case, all the characteristic symptoms of Sezary syndrome had been there all along:
- Erythroderma and unrelenting pruritis not responsive to other treatments
- Lymphadenopathy (AB felt swollen all the time)
- Hepatosplenomegaly (altered liver function tests)
- Loss of body hair and poor nail and hair health
- Inability to control own body temperature.
However, it is important to note that Sezary syndrome is extremely difficult to diagnose so it is not surprising that it took AB’s GP and dermatology consultant years to identify it and it was outside my sphere of expertise to suspect it.
The homeopathic approach to patients is often described as not needing a diagnosis as treatment focuses on symptoms not syndromes, but in the case of AB, her responses to remedies (especially the Carcinosin) and her relentless itching have only come to make sense in the light of the Sezary syndrome diagnosis. In particular, AB’s aggravation from the first dose of Carcinosin may well reflect the pathophysiology of the disease; the skin rash only manifests when the circulating cancer cells move from the blood to the skin9, so it was entirely conceivable within homeopathic philosophy that the Carcinosin remedy was moving the cancer along the direction of cure, from innermost to outermost.
AB was relieved to finally have a formal diagnosis and for me, it was the final piece of her complex puzzle that I had been missing all along.
- Conclusion
Since receiving her diagnosis, I have continued to see AB, supporting her through the side effects of steroids and chemotherapy. Our joint treatment goal had always been to relieve the itching and to date, we have yet to manage this!
I wanted to share AB’s story to highlight the advantages of an eclectic and practical homeopathic education such as that provided by CHE. Through having many different approaches at my disposal I was able to continually try new avenues to gain traction in her case, understand what was going on and help her. I have also written this case for others to read for two reasons: firstly, to acknowledge that homeopathy cannot solve all problems that patients bring to us; and secondly, that some patients are humbling reminders that as homeopaths, no matter how much we feel we have learnt, we are perpetual students and our patients are our teachers. This was a case that represents homeopathic treatment as an on-going journey for both the patient and practitioner. Sometimes the reality of being a homeopath is a lot of head-scratching, reading and hoping, but we keep going because we honour our patients by not giving up on them when they have not given up on us.
Acknowledgements
I would like to acknowledge Angelina Mosley for her complete dedication and unconditional support and encouragement, in this case and many others at all times and without reward. I would also like to acknowledge the support I received from Rachel Swanney and Laura Bailie. My homeopathic colleagues have been amazing and I am very grateful.
References
- Homeopathy and Minerals, J Scholten, 1993, Stichting Alonnissos, Utrecht, The Netherlands., p71-73.
- Using Miasms in Homeopathy, P Fraser, 2008, Winter Press, Kent, UK., p13-16.
- Prisma, The Arcana of Materia Medica Illuminated, 3rd ed, F Vermeulen, 2004, Emyrss bv Publishers, Haarlem, The Netherlands.
- Materia Medica of Homeopathic Medicines, 2nd ed, SR Phatak, 2004, B Jain Publishers, New Delhi, India.
- Desktop Guide to Keynote and Confirmatory Symptoms, R Morrison, 1993, Hahnemann Clinic Publishing, California, USA.
- Homeopathic Detox Therapy; a renewed look at homeopathy. Syllabus, Version 1.1 T Jansen & A van Veen.
- What about the Potency?, M Shine, 2004, Food for Thought Publications, Norfolk, UK.
- Bowel Nosodes in Homeopathic Practice, J Saxton, 2008, Saltire Books Ltd, Glasgow UK.
- Sezary syndrome; Genetics home reference. Available from: http://ghr.nlm.nih.gov/condition/sezary-syndrome



I speak up reluctantly, because I don’t like to criticize fellow homeopaths. I have often said that more often than not, our profession takes its inspiration from allopathy and not so much from Hahnemann and The Organon. The fact is, though remedy selection seems well thought-out in this case, the dosing schedule and potency selection seem right out of a doctor’s office instead of The Organon. Though the Organon may have been “read” at the author’s school, it clearly was not studied. I can say only at this point that Aphorisms 275 and 276 should be read by the author and her fellow school mates immediately. These are the aphorisms that warn against unnecessary high potencies and too-frequent repetitions as, according to Hahnemann, they can make the case almost incurable and even cause the death of the patient. Homeopathy historian Julian Winston was once asked, “Don’t you think more people should be prescribing as per the 6th ed. of The Organon?” Julian replied, “I would be happy if people would prescribe as per ANY edition of the Organon!” Dr. Luc De Schepper has said, “Case management is poor world-wide.” Because of this fact, I wrote an article called “Organo-Phobia (Fear of Reading the Organon)” which is here: https://hpathy.com/homeopathy-papers/tidbits-24-organo-phobia-fear-of-reading-the-organon/ and I would hope that everyone here would read it in the best interests of homeopathy and our patients, who always have to come first.
My reply may be irrelevant but looking at the prescriptions and the potencies and usage of double remedies, the practitioner has deviated too much from the basic principles. Kent mentioned that homeopathic failures are the worst failures – and the above is one among them.