 A clear understanding of pathogenesis, pathophysiology and symptomatology goes a long way in understanding and solving a case. Pathogenesis is a chain of biological mechanisms that leads to the diseased state. Pathophysiology refers to the functional changes resulting from disease. Symptomatology refers to the set of symptoms characteristic of a medical condition. What lies beyond these are the characteristics of the person in a state of disease – what we call the individualizing factors. To find the simillimum we must find a match that covers this entire spectrum. Let us take the example of a stuffy nose.
A clear understanding of pathogenesis, pathophysiology and symptomatology goes a long way in understanding and solving a case. Pathogenesis is a chain of biological mechanisms that leads to the diseased state. Pathophysiology refers to the functional changes resulting from disease. Symptomatology refers to the set of symptoms characteristic of a medical condition. What lies beyond these are the characteristics of the person in a state of disease – what we call the individualizing factors. To find the simillimum we must find a match that covers this entire spectrum. Let us take the example of a stuffy nose.
A stuffy nose affects the quality of life
A blocked nose is a very common symptom encountered by a large number of people. It is described subjectively as fullness, obstruction, reduced airflow, being “stuffed up”, or “stopped up”. It is often the predominant symptom in disorders such as allergic rhinitis, rhinosinusitis, non-allergic rhinitis, and nasal polyposis. Nasal congestion is also a common symptom in middle ear infection (otitis media) and asthma. It can lead sleep disturbances, including instances of shallow or infrequent breathing during sleep (obstructive sleep apnea) which can be life threatening.
A blocked nose can have a significant impact on quality of life in terms of emotional function, loss of productivity, and the ability to perform even routine daily activities comfortably [1]. A blocked nose comes with a heavy price tag – it has an economic impact. Surveys in the US indicate that in the year 2004 rhinosinusitis alone affected tens of millions of people and led to an expenditure of approximately $6 billion in overall health care [2].
Perception and Pathology
Nasal congestion is defined as a perception of reduced nasal airflow or a sense of facial fullness, and it can involve a number of underlying mechanisms. For example, inhaling mentholated vapors activates the cold receptors in the nasal passage and this cool sensation creates the impression of increased airflow without actually altering airflow [3]. Conversely, patients with complete turbinectomy (“empty nose”) may still complain of the perception of nasal congestion [4].
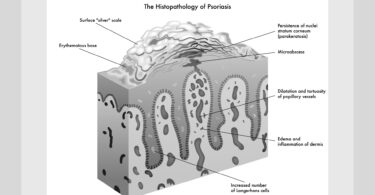
Nasal congestion usually starts with an irritation triggered by an allergen or an infection of the mucosal membrane in the nasal passage which results in an inflammatory response. This response involves increased congestion of veins, increased nasal secretions, and consequently a swelling of the related tissues. This leads to physical problems affecting the structure of the nasal passage; and affects sensory perception. Advances in medical technology like rhinomanometry and acoustic rhinometry, have made it possible to qualitatively and quantitatively study the nasal airways, and have provided greater insight in understanding this more-than-irritating symptom [5]. In a typical episode of allergic rhinitis or rhinosinusitis the physical size of the nasal passages is reduced due to widening of blood vessels (vasodialation). These effects result in increased blood flow and consequent increase in the flow of cells responsible for immune response (lymphocytes) moving across the walls of the blood vessels (increased vascular permeability). This causes swollen tissues inside the nose that cause obstruction of nasal airflow, ultimately contributing to nasal congestion. These swollen tissues can also cause blockage of the drainage pathways of sinuses.
But it’s not just germs and allergens
A blocked nose is not necessarily the consequence of allergic rhinitis or rhinosinusitis. It has been found that all these effects can be produced through the central nervous system (neural mechanisms) without any demonstrable mucosal abnormality. This is so because the nose is armed with a complex nervous system that includes sensory, sympathetic, and parasympathetic nerves. It is also known that emotions can trigger physiological responses that are regulated by the brain [6]. Thus the constellation of symptoms that we see in rhinitis can also be triggered emotionally. It is also interesting to note that neural activity in the nose can influence physiology in another part of the body as well, typically in the bronchial tree and the cardiovascular system. Such an exaggerated physiological response is called neural hyper-responsiveness, which is not yet fully understood [7].
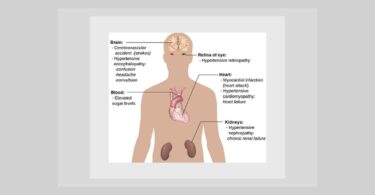
Hypertension and the stuffed nose
Research indicates that there is an association between impaired respiratory function and hypertension. Hypertension is found to be more frequent in men with rhinitis than in men without rhinitis (even after adjustment for major known confounding factors). Hence it is recommended that blood pressure should be regularly checked in men with rhinitis. However researchers admit that the physiopathological mechanisms underlying these associations are not known [8]. In what would be a corollary to these findings, research seems to suggest that treatment of allergic rhinitis can improve blood pressure [9].
Decongestants and blood pressure
The paradoxical situation one faces is that most allopathic decongestants you would like to use to improve your quality of life are contraindicated if you have high blood pressure. Typically these drugs are oral nasal decongestants such as pseudoephedrine and phenylephedrine; topical nasal decongestants, such as oxymetazoline, phenylephrine, naphazoline; and the Vicks Vapor Inhaler (l- desoxyephedrine/ levmetamfetamine); topical hemorrhoidproducts; asthma alleviating products containing ephedrine, aspirin; and NSAIDS, such as ibuprofen.
A homeopathic case
The author dealt with a case of a 60 year old male who was in a good state of health and was not taking any medications for any chronic complaints. He had a history of persistent stuffy nose. It would start with an episode of non-allergic rhinitis. He felt it was caused by stress as he could not associate any particular allergen (like dust, pollen, food etc) with this complaint. He would suffer such an attack two to three times a year. The attack of rhinitis would be followed by nasal congestion and then it seemed that the catarrhal condition had “fallen” into the chest. Recently he had relocated to a new home in a new city, so there was latent stress due to these changed circumstances.
When he consulted me I used the following rubrics (after combining):
COUGH – ASTHMATIC etc…:
MIND – Dreams of death, dying, dead people etc…:
RESPIRATORY SYSTEM – Expectoration – Viscid, tenacious, difficult of raising etc… etc…:
NOSE – SNEEZING – violent etc…:
NOSE – Obstructed etc…:
CONDITIONS OF AGGRAVATION AND AMELIORATION IN GENERAL – Coition – after – agg. etc…:
The top remedies were kali-c, kali-bi, nux-v, carb-v, lyc, anac.
He also reported an aggravation at 3 am in the morning and around 8 pm evening. Kali-c, nux-v and lyc were the leaders. Given the affinity of Kali salts to the mucosal membranes the choice was kali-c.
The patient did quite well on kali-c 30, and in a follow-up after 3 weeks he was free from all the symptoms. Interestingly he said that he had a long standing complaint of dandruff which also seemed to have vanished. However, two months later he came back again with the same symptoms (minus the dandruff). Kali-c 30 was repeated but the symptoms showed only a slight improvement, and only worsened after a week. Nux-v was next considered as it figured quite prominently in the repertorial analysis. But that did not help. In fact the patient has to use Otrivin nasal spray (xylometazoline) for symptomatic relief.
Search for an intercurrent remedy
During this period he underwent a routine medical screening for renewal of a health insurance policy which included an ECG, a chest X-Ray, lipid profile, creatinine/ urine analysis and blood sugar checkup. While these test returned normal values, the blood pressure was noted to be very high -210/100 mmHg. The patient had been asymptomatic for any cardiovascular complaints and was not taking any medication for blood pressure control and was keen not to take any medication on a life-long basis. He preferred to take homeopathic treatment only.
In view of his medical reports, the author considered an intercurrent remedy – Rauwolfia serpentine, a remedy known quite well to herbalists as well as homeopaths. It was the first allopathic drug to be introduced specifically for hypertension [10]. It was a major breakthrough in therapeutics. Efforts were made by the pharmaceutical industry to extract and identify the active ingredient and synthesize the same for clinical use. Reserpine was identified as the active ingredient and introduced in the market. However, very soon both the drugs fell out of favor due to reported side effects. Among the side effects reported for these drugs were: dry mouth, stuffy nose, nasal polyps, loss of appetite, reduced desire for sexual intercourse, diarrhea, and abnormal heart rhythm. There have also been reports of psychiatric symptoms like depression and suicidal tendencies, restlessness, and insomnia. Rauwolfia was added to the homeopathic repertorium after Templeton’s provings in 1955. The proving symptoms replicated the “side-effects” reported by allopathic users of the same drug, in particular the concomitants of stuffed nose and elevated blood pressure.
The patient was prescribed Rauw. MT, and Crataegus MT, 5 drops, three times a day. Blood pressure was checked after 10 days and was found to be 145/90 mmHg. The patient was impressed with this remarkable effect on his blood pressure values. Subsequently he monitored blood pressure on a daily basis (mornings and evenings) and he found a steady improvement as it settled between systolic 125-130 mmHg and diastolic 70-90 mmHg.
But the stuffy nose did not improve and he had to revert to the use of the nasal spray. He also reported dryness of the mouth. At this point the author considered using Rauw in potentized form and selected 6C potency in medicated pill form – 2 pills twice daily. Crataegus MT was discontinued. Within a week the stuffy nose cleared up gradually and he discontinued the use of xylometazoline nasal spray completely.
It is interesting to note that Rauw has obstruction of nose (chronic), dryness of mouth, sneezing, sleep disturbance at 3 am, 8 pm aggravation, cough aggravated by lying down, diminished sexual libido, and dreams of dying, dead people and death [11]. However, Rauw is a small remedy and will not show up in a repertorial search for rhinitis-like complaints. But an understanding of the connection between hypertension and swollen turbinates in the nasal passage and its relationship to the proving symptoms and clinical symptoms of Rauw made it possible to help the case.
The way ahead
The patient has been symptom free for a few months, but the author has asked the patient to follow-up with a session to work out a “constitutional” remedy to prevent acute manifestations of an underlying chronic condition. It is interesting to note that Rauw is associated with the increased Morg-g in stool cultures. Since the patient is symptom free and not on any medication, perhaps a dose of bowel nosode Morg-g could help give a clearer picture?
The case showed that an understanding of the pathogenesis, pathophysiology and symptomatology in a case can help us to form a clearer picture of the totality. The author is grateful to Dr. Sunirmal Sarkar of Kolkata for the guidance provided by his book on clinical approaches [12].
References
- Shedden A: Impact of nasal congestion on quality of life and work productivity in allergic rhinitis: findings from a large online survey. Treatments in Respiratory Medicine 2005;4(6):439-46.
- Leggett JE: Acute sinusitis. When – and when not – to prescribe antibiotics. Postgrad Medorrhinum 2004;115(1):13–19.
- Eccles R. Menthol: Effects on nasal sensation of airflow and the drive to breathe. Curr Allergy Asthma Rep. 2003;3(3):210–214.
- Naclerio RM, Bachert C, and Baraniuk JN: Pathophysiology of nasal congestion, International Journal of General Medicine 2010:3 47–57.
- Corey JP, Houser SM, Ng BA: Nasal congestion – a review of its etiology, evaluation, and treatment. Ear Nose Throat J. 2000; 79(9):690–698.
- Dirk Hagemann, Shari R. Waldstein, Julian F. Thayer: Central and autonomic nervous system integration in emotion, Brain and Cognition, volume 52, issue 1, June 2003, p. 78-79.
- Sarin S, Undem B, Sanico A, Togias A: The role of the nervous system in rhinitis. Journal of Allergy and Clinical Immunology 2006 Nov;118(5):999-1016.
- Sabine Kony, Mahmoud Zureik, Catherine Neukirch, Bénédicte Leynaert, Daniel Vervloet, andFrançoise Neukirch: “Rhinitis Is Associated with Increased Systolic Blood Pressure in Men”, American Journal of Respiratory and Critical Care Medicine, Vol. 167, No. 4 (2003), pp. 538-543.doi: 10.1164/rccm.200208-851O
- Magen E, Yosefy C, Viskoper RJ, Mishal J: Treatment of allergic rhinitis can improve blood pressure control. Journal of Human Hypertension 2006 Nov;20(11):888-93. Epub 2006 Sep 7.
- Vakil RJ: A Clinical Trial of Rauwolfia Serpentina in Essential Hypertension; British Heart Journal 1949;11:4 350-355doi:10.1136/hrt.11.4.350.
- Stephenson J: Materia Medica and Repertory 1924-1959. Proving of Rauwolfia serpentina
- Sarkar Dr. S: Just You See, Homoeopathic Medical Publishers, Mumbai, 2013.

This article by Dr Rajguru is indeed very well written in a manner that can be easily understood by laypersons like myself .It certainly emphasises the importance of understanding the pathogenesis, pathophysiology and symptamatology of any particular case in order to get a clear holistic picture of an individual for diagnosis and treatment even in simple ailments such as a blocked nose…
This article is guru gyan.blocked nose disturbed emotions.kent lecture says see red knob on end of nose strawberry nose,lachesis nose drunkarad with black blood black heart facepurple mottled,beware notice planted on nose,sixth sense of kent is unparallel.in general homeopaths are feared of using lachesis remedy warn that it should not be repeated.learned doctor is requested to advise how to deal with red nose personalities.
our grand fathers were using gidadbaha naswar to clear the blocked nose natural otrivin,gurdas man punjabi singer belongs to gidadbaha he is also highly emotional,ayush may research if naswar has any link with emotions.wether using inhalers we are stuffing emotions in our lungs,why not drain out with naswar.brain fog with hypothroidism and hypotension article by ami shah is relevant.gurdas man they say is charitable person,gidadbaha naswar role in healing emotions be researched.
sir,my above naswar comment be deleted,i was not aware of naswar content,my apologies for in convenience,i am hurted for my ignorance.