Abstract:
A 13 years boy suffering from vitiligo was seen and managed at Bakson Homoeopathic Medical College and Hospital ,OPD, Greater Noida. The boy presented with de-pigmented milky white patches on eyelids and left cheek with gradual involvement of elbows and legs with positive family history.The patient had Psoric and Syphilitic manifestations, and considering his physical make-up, tendency to catch cold, rapid emaciation and narrow chest, Tuberculinum 200 single dose was prescribed initially to clear the miasmatic block but not much change was seen. Later, on reportorial totality, Calcarea Carbonicum LM potencies 0/1 to 0/3 were prescribed and the case responded favourably with permanent disappearances of most patches and restoration of normal skin colour. (See full case below)
INTRODUCTION–
The term vitiligo is derived from a Latin word VITILUS-meaning calfand was first used by roman physician Celsus of the 1st century AD .The characteristic patches of the disease resemble the white patches of calf in India. It occurs in about 1% of the population,with no gender predilection. It affects all ages, peak incidence between 10-30 years; almost 20% of patients have a positive history of vitiligo in the family .[1]
Vitiligo is a disfiguring disease of unknown origin that causes destruction of melanocytes. The usual presentation (type A) is a symmetric pattern of white macules (5mm to 5 cm or more) with well-defined borders. The type B segmental vitiligo, is limited to one segment of the body (e.g. extremities) and is more common in childhood. Some patients have a positive family history. It is also frequently associated with auto-immune disorders like alopecia areata and thyroid disorder. Non-segmental vitiligo has a greater prevalence than the disorders of other form(s) [2]
Morphology of the lesion is depigmented macules, chalky or milky white in colour .The depigmented centre is surrounded by a hypopigmented rim which has normal pigmented skin around it. Areas subjected to repeated trauma and friction are subject to it, eg. dorsal aspect of hands, feet and knees.There is a marked reduction or even absence of melanocytes and melanin in the epidermis. Histochemically there is a lack of DOPA- positive melanocytes in the basal layer of epidermis.The macules may vary in size, shape and colour as well. Lesions may be of the hypo-pigmented rather than de-pigmented type.The course of the disease is very variable.[3] It occurs with frequency of 0.1 – 2 % in various populations. Family clustering of cases is not uncommon, in a non-mendalian pattern suggestive of multifactorial, polygenic inheritance. A survey of 2624 vitiligo probands from North America and UK showed that more than 83% of probands were causations, and frequency of disease is equal in males and females. The frequency of in proband’s siblings was 6.1%, about 18 times the population frequency, suggesting a major genetic component in pathogenesis. The concordance of vitiligo in monozygotic twins was only 23% indicating a non-genetic component also plays an important role. Probands with earlier disease onset tended to have more relatives affected with vitiligo suggesting greater genetic component in early onset families. Vitiligo has been mentioned in the tomes of every major religion, with its first description dating back more than 3000 years, to the earliest Vedic and Egyptian texts.Despite its ancient recognition, confusion with disorders such as leprosy has been a problem throughout the ages. This has lead to the stigmatization of vitiligo sufferers. This is a social problem that is still widespread in some, but not all parts of the world.
The following case shows the scope of homoeopathic intervention in this dermatological case.
Case Summary
A 13 year old boy with milky or chalky white patches on his body was seen in the OPD in march 2011.He had white patches which started from both eyes and on the left cheek and involved both legs . The patient complained of un-refreshing sleep; there was also pain in the head after waking up and also pain in knees. The patient had not taken any other treatment for his complaint.

The patient presented the following symptoms:-
Presenting Complaints:
Milky white patches on the body since 4 years.
History of Presenting Complaints:
The boy was apparently healthy before 4 years, when a small de-pigmented patch appeared on the eyelid and left cheek, then gradually involved the legs and elbow
Past history:
Patient has suffered from typhoid, 10-11 years ago
Family history:
Cousin / Brother suffering from leucoderma
Personal History: Nothing Specific
General examination
Build – lean thin emaciated
Nutrition – poor
Facies – normal
Decubitus – sideways
Level of consciousness – well oriented with time place and person
Pallor – absent
Icterus – absent
Cyanosis – absent
Oedema – absent
Clubbing – absent
Temperature – 99.10 F
Pulse – 70/min
Respiratory rate – 18/min
Blood pressure – 120/80 mm hg
Lymphadenopathy – absent
Physical generals:-
Appetite-normal, 3 meals/day
Thirst-5-6 glass/day
Desire-sweets, eggs
Tongue-white coated
Stool-once in a day, satisfactory
Urine-burning during micturition
Perspiration-profuse on forehead
Sleep-8-9hrs, unrefreshing sleep, headache on waking up
Thermal reaction-general aggravation of complaints in cold weather
Mentals
- Anger-whenever the patient is angry, he throws the things nearby in order to express his anger.
- Likes company
- Memory-good and can remember things for a long time.
Case Processing
Analysis of symptoms –
Common symptoms –
Milky or chalky white patches on the body
Uncommon symptoms –
Likes Company
Memory active
Easily angered – throws things nearby him in order to show his anger
Aggravated by cold weather
Desire – sweet, eggs
Sleep – unrefreshing, headache on waking up
Perspiration – profuse on forehead
Burning during micturition
Evaluation of symptoms –
Mentals
Easily angered – throws things nearby him in order to show his anger 3+
Likes Company 2+
Memory active 1+
Physical Generals –
Aggravated by cold weather 3+
Desire – sweets 2+
Desires-eggs2+
Sleep – unrefreshing, headache on waking up 2+
Perspiration – profuse on forehead 2+
Burning during micturition2+
Particulars –
Milky or chalky white patches on the body 3+
Totality Of Symptoms –
Milky or chalky white patches on the body
Easily angered – throws things nearby him in order to show his anger
Likes Company
Memory active
Desire – sweets, eggs
Sleep – unrefreshing,headache on waking up
Perspiration – profuse on forehead
Burning during micturition
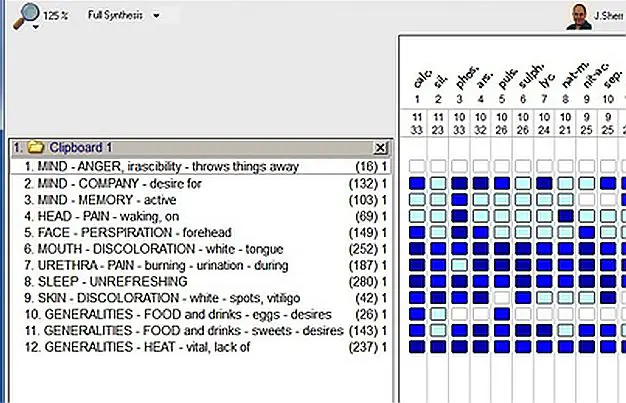
REPERTORISATION [4]
Rubrics –
- MIND – ANGER, irascibility – throws things away
- MIND – COMPANY – desire for
- MIND – MEMORY – active
- HEAD – PAIN – waking, on
- FACE – PERSPIRATION – forehead
- MOUTH – DISCOLORATION -white – tongue
- URETHRA – PAIN – burning urination-during
- SLEEP – UNREFRESHINGSLEEP – UNREFRESHING
- SKIN – DISCOLORATION – white -spots, Vitiligo
- GENERALITIES – FOOD anddrinks – eggs – desires
- GENERALITIES – FOOD anddrinks – sweets – desires
- GENERALITIES – HEAT – vital, lack of
REPERTORIAL ANALYSIS
Calcarea Carbonica – 11/33, Silicea. – 11/23, Phosphorus – 10/33, Arsenic- 10/32, Pulsatilla – 10/26, Sulphur – 10/26 , Lyco. – 10/24, Nat.Mur. – 10/21, Nit. Acid –9/25, Sepia – 9/25
Follow ups:
| 29/3/2011 | Tuberculinum 200 | 1 dose [stat] | Tuberculinum 200 single dose was prescribed considering the miasmatic dyscrasia of the patient and the pathogenesis of the disease, especially the patient’s physical appearance, tendency to catch cold, rapid emaciation and narrow chest and desire for constant changes. | |
| 2 | 12/4/2011 | Sac Lac. 30 | BD for 2 months | Not much change seen |
| 4 | 3/6/2011 | Calcareacarb 0/1 | Od for 1 month | White patches on cheek and elbow joint diminished hair becoming slightly golden. On the basis of repertorial analysis and knowledge of Materia Medica, Calcarea Carbonicum was prescribed |
| 6 | 3/8/2011 | Sac Lac 30 | BD for 2 months | General condition improving; white patches diminished further in size; patient feels refreshed after sleep. |
| 7 | 18/8/2011 | Calcareacarb 0/2 | Od for 15 days | General well being felt .the patches are reducing in size. pigmentations seen in patches . |
| 8 | 30/8/2011 | Sac Lac 30 | BD for 15 days | Patch on cheek totally disappeared; sleep normal ,refreshing ;patches on knee and leg started diminished |
| 9 | 18/9/2011 | Calcareacarb 0/3 | Od for 1 month | Better; the patches on knee getting diminished and has mostly disappeared |
| 10 | 19/10/2011 | Sac Lac 30 | BD for 2 months | Patches on face have totally disappeared and those on knee are getting diminished |
| 11 | 18/12/2011 | Sac Lac 30 | BD for 3 months | Knee shows no presence of patches |
| 12 | 20/3/2012 | Sac Lac 30 | BD for 3 months | Knee patches disappeared totally, sleep – refreshing. Patches on shin bone getting diminished |
| 13 | 15/6/2012 | Sac Lac 30 | BD for 3 months | Patches on shin bone disappeared totally. The size is reducing from periphery with pigmentations in centre. |
| 14 | 19/9/2012 | Sac Lac 30 | BD for 3 months | General condition better, no patches seen in all over body |
| 15 | 18/12/2012 | Sac Lac 30 | BD for 3 months | General condition improved |
| 16 | 20/3/2013 | Sac Lac 30 | BD for 3 months | Improved |
| 17 | 19/6/2013 | Sac Lac 30 | BD for 3 months | Improved
The patient is still following up. |
SUM OF SYMPTOMS (SORTED DEGREE)
On the basis of repertorisation and with relation to materia medica and observation analysis, the best indicated remedy is
Calcarea carbonica
DISCUSSION:
In homoeopathy there is no use of steroids or UV rays and no surgical measure is required. It has a holistic approach that it treats the patient as a whole and considers the totality as a whole taking into account The mentals, physical generals and particulars of the patient. In this particular case it resembled Calcarea Carbonica and when it was prescribed in LM potency the case got its direction of cure with diminishing size of patches. The LM potency was prescribed to the patient and there was no aggravation.
The patient had some Psoric and Syphilitic manifestations from a miasmatic and pathogenesis point of view, with destruction of melanocytes in its background. Secondly, vitiligo being a one sided disease, considering patient’s physical make-up, tendency to catch cold, rapid emaciation and narrow chest, it was expected that Tuberculinum would bring about the clear picture of the patient and help in building the totality. Also, being a nosode, it would pave the way for better action of subsequent medicines.
Research
In an observational study of vitiligo where 207 patients were treated, Arsenicum sulphuricum flavum, Arsenicum Album, and Nitric Acid were found to be useful and Syphillinum was effectively used as an intercurrent remedy[5]. In another case Phosphorous 30 was found of great help to reduce the hypopigmented patches and treatment was continued for a period of 17 months.[6]
In the present study the medicines which were found useful were Tuberculinum and Calcarea Carbonicum.
Conclusion
The remedy when prescribed according to the principles of homoeopathy, leads to the permanent restoration of health, which was demonstrated in this case. The patches are reducing in size and gaining normal skin texture. The correct approach for analysis and evaluation has to be followed.
This case again proves beyond doubt the importance of a good case taking, paving the way for correct repertorization and final selection of the simillimum.
Acknowledgment
I shall remain grateful to Dr. C Nayak, Director and professor, for being an inspiration and great motivator. I am thankful to my students Dr. ManmeetKaur, Dr. Tina Banerjee, Dr.Chaksu Mishra and Dr.Vijaya Goswami for assisting me in compilation.
References:
- Sehgal Virender N, Text Book of Clinical Dermatology. Fifth ed. New Delhi:Japee Brothers Medical Publishers (P) Ltd, 2011.
- Behl P N, Practice of Dermatology. Fifth ed. Calcutta: Allied Book Agency, 1982.
- Khanna Neena, Illustrated Synopsis of Dermatology & Sexually Transmitted Diseases. New Delhi: PEEPEE Publishers & Distributors (P) Ltd, 2005.
- Complete Repertory Radar10
- Prasad R.V.R., Ravender Ch., BharathaLaxmi, Singh K., Vichitra A.K., OberoiPr, et al. Clinical evaluation of pre-defined homoeopathic medicine.Vitiligo. Clinical research studies- Series II-New-Delhi; CCRH 2009;pg-85-95.
- Ravi Kumar. A. Case of Vitiligo treated with Phosphorous. Indian journal of research in homoeopathy 2008; (I): 49-57
For more information about vitiligo visit-
https://hpathy.com/cause-symptoms-treatment/vitiligo-leucoderma/