
It’s very commonly said, “The scope of homoeopathy begins where that of other pathies end.” Today, I would like to share with you how this thought got etched into my life through my experience in a very simple yet commonly seen disease of the skin and how homoeopathy can do wonders in such cases.
INTRODUCTION:
Molluscum contagiosum –is a viral disease caused by a DNA poxvirus that is largely (if not exclusively) a disease of humans. Molluscum contagiosum virus causes characteristic skin lesions consisting of single or, more often, multiple, rounded, dome-shaped, pink, waxy papules that are 2-5 mm (rarely up to 1.5 cm in the case of a giant molluscus) in diameter. The central umbilication of the papules containing a caseous plug forms the hallmark for diagnosis.
Histology-
The epidermis appears thickened (acanthosis) within the region of indentation, up to 6 times the thickness of the surrounding, uninvolved skin, and the cornified layer typically is disintegrated. The striking feature is the presence of intracytoplasmic, eosinophilic, granular inclusions called the Henderson-Paterson bodies within the keratinocytes of the basal, spinous, and granular layers of the epidermis can measure 35µm in diameter.
Infection –
It follows after contact with infected persons or contaminated objects. Lesions may spread by autoinoculation. The initial infection seems to occur in the basal layer, and the incubation period is usually 2-7 weeks.
Clinical features –
It is most common in children but may be found in persons of all ages. The virus is transmitted by direct skin-to-skin contact, through minor abrasions or indirect skin contact with fomites, such as bath towels, sponges, and gymnasium equipment, transmits the virus. Among young adults, it is usually a sexually transmitted disease. Lesions typically occur on the chest, arms, trunk, legs, and face but rarely on palms and soles. These lesions are usually painless. It is generally self-limiting in healthy patients and heals spontaneously within 6-9months, some persist for 3-4years.
Treatment-
The mainstay of taking treatment is most often for cosmetic reasons and spontaneous recurrence.
Conventional treatment includes surgical removal by scraping, de-coring, freezing, or through needle electrosurgery. This may result in scarring or post inflammatory pigmentary changes. Frequently, multiple treatment sessions are necessary because of the recurrence of treated lesions and/or the appearance of new lesions.
Homoeopathic treatment involves the administration of a well-selected constitutional remedy in each individual case.
A case of a 23-year-old female who visited me on 29th of March 2016.
CHIEF COMPLAINT:
- Molluscum contagiousum since 8 months.
L: On face and neck.
Started on forehead and then spread all across the face and neck.
No form of medication or external application was used for the same.
ASSOCIATED COMPLAINTS:
- Acne on face- comes and goes, no relation with menses
No treatment taken for it
- PCOD, diagnosed in 2009
USG dated 22/12/09 suggests- Normal sized uterus
Cervical fibroid (1.3cmx1.5cm)
Both ovaries are enlarged in size with presence of multiple small follicles at periphery suggestive of polycystic ovaries.
Rt ovary measures 2.4cm x 2.8cm x 3.8cm, volume 13.32cc
Lt ovary measures 2.0cm x 2.9cm x 3.6cm, volume 10.94cc
Menses are irregular, dark red, profuse lasting for 5-6 days.
Complaints before and during menses- severe cramping pain in lower abdomen
Takes Tab. Dymen for this pain.
No complaints after menses
LMP- 5/2/16
- Tendency to catch cold easily
<change of weather, <winters, <cold drinks/cold food
Suffers from breathlessness in winters and takes Asthalin pump (SOS).
FAMILY HISTORY:
Paternal Grandfather- DM, expired from brain hemorrhage
Paternal Grandmother- 80yr -DM
Maternal Grandfather-HTN, expired from MI
Maternal Grandmother-HTN, expired from MI
Mother- 57yr- HTN
Father – 64yr – Chronic Kidney Disease, Hypertension, DM, IHD
Sisters (identical twins)- 28yr old- PCOD, Primary infertility
– 28yr old- PCOD
PAST HISTORY:
No significant surgical history
Admitted in 2014 for Acute Gastroenteritis with Intestinal Obstruction- Managed medically.
GENERALS:
App- Good
Thirst -1litre/day; room temperature
Likes- cheese+, chocolates, carbonated drinks, potatoes
Dislikes – nothing specific
Perspiration – upper lip, forehead
Sleep – position- back
eyes- half open during sleep
disturbed by slightest noise
cannot sleep in darkness
Thermals- Chilly patient
Likes winter
Can tolerate summer better
Fan-Seasonal
Bath- seasonal
Covering – throughout the year.
MENTALS/LIFE SPACE SITUATION:
Patient is the third child, born and brought up in Mumbai.
She has completed her graduation B.A Economics, in 2003. She was working as a content writer but recently quit her job due to her father’s ill health. Loves to read, travel. Says she gets angry when people don’t listen or do as she says. Family is very career oriented. Sisters- twins- elder is chartered accountant. Younger twin is a doctor. Expectations are high that she also should do something big in education. But she never felt inclined towards making her career in such a field. She is very creative and loves drawing, writing poems and even acting in plays.
She is very close to her family members. A constant worry is her father’s ill health. Father was diagnosed with CKD in 2008 and has been on dialysis since 2011. He is on dialysis and not improving much. Her eldest sister is married and staying in Chennai. And the other sister is a doctor but does full time duty at a hospital in Andheri so then it’s only her mom who has to handle everything for her father. Hence she quit her job to help out at home and to take care of any medical needs for her father.
There is a marked fear of darkness. She is very particular about her work (perfectionist). Wants that things should be kept in order, in their place.
REPERTORIAL TOTALITY:
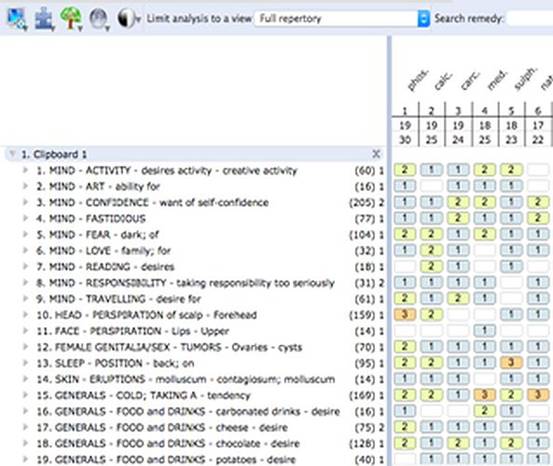
PRESCRIPTION: Carcinosin 30 tds
DISCUSSION:
My understanding of Carcinosin comes from what I have seen while working with Dr. Farokh Master. Here is a brief explanation of why I chose Carcinosin in this case. The Carcinosin child comes from a family where the parents are very pushy / demanding of the child to do well in studies, to excel in life. They expect a lot from the child. These children have never been able to express their own individuality. They cannot ‘be themselves’ for fear that they will not be accepted, they will not be appreciated, they will not be loved, and thus they are in a state of constant insecurity. They appear as accepting, submissive or even repressed persons. They are artistic, love – reading, dancing. Carcinosin patients are very sympathetic and compassionate people. They are extremely sensitive to the sufferings of others. They are the ones who sacrifice their comfort for others. A strong sense of responsibility is usually seen. Children feel overly responsible from an early age on, taking on responsibility for the whole family. They are very reliable in looking after their pets, taking care of the household, and so on. Their exaggerated sense of responsibility for the well-being of their relations and loved ones may lead to feelings of guilt, anxiety fits and eventually depressive states.
All carcinosin patients tend to be anxious and fears form an integral part of the picture. Another strong characteristic is an inherent need to establish order, to remove the disorder around them (or so they feel) and in response to this need they can become fastidious. It is as if they feel the threat from the oncoming internal disorder.
Strong craving for cheese.
Desire to travel.
Strong family history of Diabetes Mellitus in the family.
FOLLOW UP:
| Date | Rx | |
| 13/4/16 | Molluscum – decreased in size over cheeks and jaw line.
No new eruptions Had an episode of cold, which settled on its own. Acne – SQ- Menses not yet got
|
Carc 30 tds x 15 days |
| 29/4/16 | Molluscum – > –
No new eruptions Nose obstruction <night Coryza- greenish, mucoid Mild cough from throat irritation Expectoration- green Acne – > – Menses- not got as yet
|
Carc 30 tds x 15days
+ Home remedies for cold and cough |
| 15/5/16 | Molluscum – SQ-
New eruptions on chin Coryza/cough -0- Acne –SQ- Menses- not got as yet
|
Carc 30 tds x 15days |
| 17/6/16
|
All complaints –SQ- | Carc 200 bd x 15days |
| 4/7/16 | Molluscum >>
No new eruptions Sneezing -0- Acne > Menses- 26/6/16, Normal flow which lasted for 7 days, NO PAIN.
|
Carc 200 bd x 15days |
| 2/8/16
|
Molluscum >
Menses – 25/7/16; normal flow, lasted for 5 days, no pain |
Carc 200 bd x 15days |
| 6/9/16 | Father’s health deteriorated, was hospitalized and that was very stressful period for her
Molluscum – SQ- only on forehead New eruptions appeared on chin, nasolabial folds Acne > Menses – late by 6 days, profuse, mild cramps in abdomen
|
Carc 200 tds x 15days |
| 15/10/16 | Molluscum – only on forehead
Acne >> Had an episode of anxiety attack in the hospital when father was admitted again. Confidence low, feeling very helpless Menses – 11/10/16, normal flow, lasted for 5 days, no pain
|
Carc 1M bd x 15days |
| 14/11/16 | Molluscum cleared
No episodes of cold/cough Acne >> Menses – delayed Confidence much better, taken up a job and also pursuing Masters in Economics. |
Carc 1M bd x 15days |
BEFORE TREATMENT:


29/04/16:


15/5/16


17/6/16


4/7/16


15/10/16


14/11/16


“A well-chosen constitutional remedy or simillimum will produce a desirable result in the very first follow up.” This case was a classic example of it and I knew that I had struck the right cord. Not only did the remedy help the patient in the presenting complaint of molluscum but it was beneficial at other planes too.
- At the level of the mind the patient was much more confident than before.
- The chronic complaint of recurrent cold and cough settled with the very same medicine.
- The menstrual abnormalities in this case- oligomenorrhoea, dysmenorhoea saw marked improvement.
I gave the same remedy but increased the potency at occasions
when the potency failed to act despite having helped earlier and
when there was a situation of acute stress leading to new
symptoms at a deeper level (mind- anxiety attack) to overcome the
crisis.
In conclusion, I would like to say that Homoeopathy shows remarkable results in many such ailments that are limitations of modern medicine.
BIBLIOGRAPHY:
- Synthesis Repertory by Schroyens F. (2009)
- Materia Medica Viva by Dr. George Vithoulkas
- Skin Homoeopathic Approach to Dermatology by Dr. Farokh Master
- http://emedicine.medscape.com/article/910570-overview
- http://virus.stanford.edu/pox/2000/molluscum_contagiosum.html
Brilliant case thank you for sharing
I have had success with Molluscum a few times with Carcinosin and agree that with this condition the constitutional remedy is the way to go. 🙂
Molluscum contagiosum vanishes itself within few months if left untreated..i do appreciate ur efforts and understanding of carcinosin though..it has definitely helped her building her confidence at mind level 🙂