Preliminary information
Name : MR. M.R.
Age : 43 years
Wife’s Age : 37 years
Religion : Muslim – Non-Vegetarian
Occupation : Beer Bar at Central Mumbai.
Admitted at: Mumbadevi Homoeopathic Hospital attached to Smt. CMP Homoeopathic Medical College, Vile Parle, Mumbai.
I.P.D. Reg. No. 1032 Class – Male / General ward
Date of admission : 23/03/1994
Date of discharge : 26/04/1994
Chief Complaint
Recurrent bouts of Jaundice since 1984.
He has had a total of 7 episodes over the last 10 years one every 5 to 6 months. The jaundice was often accompanied by fever, acute abdominal pains and dyspepsia as described below:
The case was diagnosed as Chronic Pancreatitis. He had severe attacks of excruciating pain in the abdomen radiating to the infrascapular region. The pain was > flexing the limbs on the abdomen. He had nausea which was > warmth, but with no vomiting. He had frequent belching with heaviness in the abdomen. Also, the flatus was impeded, could not come out. During this time he would develop fever with chills that would last the whole night with a concomitant splinter like pain in the eyes.
The twisting, griping pain in the abdomen would radiate to back. The patient described this pain as, “agonizing and makes me restless. I am like a fish tossed out of the pond“. Concomitantly he would have itching all over the body, a lot of weakness and his sclera was yellowish.
Other Complaints:
Diabetes Mellitus under poor control. Blood sugar levels were erratic with irregular intake of Insulin. This was diagnosed when he had the first attack of jaundice with pancreatitis.
- Craving: spicy 3 – pungent 3
- Perspiration: profuse
- Thermal state : HOT patient
- Likes Winter 3 : No covering
- Always wants fan; takes cold water bath.
Life Space appreciation
Mr. M. is from Zamindar [Landlord] family from Bihar.
His father was an excise inspector and was a respectable land lord of the village. He was considered a man of principle, who would not tolerate wrongdoing. He punished villagers and had them beaten if they did anything wrong. His mother was calm & quiet.
He was proud of his village being in the neighborhood of an ex- Prime Minister Chandrashekhar’s village, Baliya. He boasted of having taken a photograph with Rajiv Gandhi. He studied up to Class 6 and used to enjoy hobbies like wrestling, playing and hunting in the forest. Initially they were quite rich. But all the problems in his family started after his grandmother’s death. His father left his job and instead they all started living on the money earned by selling off their land.
Around this time he came to Bombay with his uncle. He stayed at Dongri and established a beer bar. Gradually he flourished in his business but developed an addiction to beer, charas, ganja etc. He used to have lot of sexual thoughts and developed “bad-habits” like masturbation. He complained of spermatorrhoea (prostatorhea). Once he got married he settled in Mumbai, and brought the rest of the family to Mumbai. He is extremely contemptuous about relatives. He makes statements like, “My grandmother was 100% mad, my wife has only 50% brain, my brother is 50% mad”. After coming to Mumbai, he came in contact with one of the top dons of the underworld and sincerely worked under him. He became this don’s right hand within no time. Robbery, extortion of money and participation in riots were his regular activities. Gambling and prostitution were inevitable accompaniments.
He expected his wife to eat heavy food, and then would want her to go jogging with which she would not comply. Also she could not conceive and that enraged him. Since he had oligospermia, he had no offspring. His infertility affected him in that he constantly worried, “My dynasty will be destroyed”. He believes he does not have any defect and even mentioned confidently that “I’m quite powerful”. He refused to take any treatment for this while his wife took treatment from different doctors, but all in vain. He mentioned that wife was not interested in going out and wanted to remain home. “I wanted to leave her and marry somebody else, so that my dynasty continues, but now at this age what will she do? This is my confusion and dilemma“.
He is extremely impulsive and violent. He had few arguments with one of his customers, which resulted in a severe altercation and fight. He was so enraged that he impulsively pushed an iron rod into the customer’s abdomen. He was arrested but somehow he got away. He is quite censorious about his parents and relatives but needs them badly and cannot stay without them. He always grumbled that though he helped the relatives, they never reciprocated. He wanted to build a bungalow for his parents so he sold his house at Virar for 4 lacs. He then purchased one bungalow for his parents at the out-skirt of his village in a remote place and spent 2 lacs in renovation and construction. His parents found it extremely difficult to stay at such a secluded spot and he had to sell the place incurring loss of Rs. 2 lacs. He says, “I’ll do whatever comes at the spur of the moment and then repent”.
Yet he is quite sensitive. He is moved by seeing poor, hungry people and tries to help them by providing money & food. He has great respect for food. If he happens to see piece of roti (bread) on the road, he will pick it up and keep it aside so that no one would walk over it. In his youth, his father would warn him about his misdeeds and he would react. Now nobody tells him anything. He is also extremely obsessed with his health. Often he would plead, “Please doctor you cure me, and for my whole life I will sing your song”. He presented several hand written papers to the doctor demonstrating monotonous repetition of complaints and anxiety about health. He repeatedly mentioned about his weak will and sought reassurance for his recovery with no disability. At the end he wrote “Doctor you are great, forgive me for my mistakes”. In spite of being a Muslim by religion on every page of the written history he put the symbol of ![]() (AUM). During the follow up he was extremely expressive and wanted to remain in close contact. He would often invite various interns and junior doctors to his restaurant and bar, which they would never accept.
(AUM). During the follow up he was extremely expressive and wanted to remain in close contact. He would often invite various interns and junior doctors to his restaurant and bar, which they would never accept.
Physical Examination:
Pulse : 71/min B.P.: 130/80 mm Hg
Abdomen : fullness present. Tongue : creamish coating
Past History: Underwent a Cholycystectomy (gall bladder removal) in 1981-82.
Past Investigations:
- Liver Function Tests
- 17/9/1992
- SGPT – 219 mu/ml
- SGBT – 87 mu/ml
- GGTP – 990 mu/ml
- Total bilirubin 2.1 mg%
- Direct 1.2
- LDH 354
- Alkaline Phosphatase 825 mu/ml
- Serum Cholesterol 279 mg
- FBS 225 PPBS 315 mg
- Australia antigen – not detected.
- Sonography:
- Dilated CBD Dilated pancreatic duct with calculi.
- ERCP suggested for obstruction at ampulla of vater.
Current Medications:
Insulin 16 units (Highly purified – Redexon Belcomlex).
Case Analysis
The following traits can be determined from the life space above and will allow us to understand the totality.
- Egoistic, contemptuous, censorious.
- Egocentric – mean and selfish
- Violent
- Impulsive
- Desires company
- Intense need for relationships
- Anxiety about health3
- Trying to please others
- HOT patient
- Craving spicy
- Tubercular affection of exocrinal and endocrinal pancreatic tissue.
This man from Bihar shows multiple facets. First the husband – wife relationship indicates his inflated ego, self centred attitude and an inability to accept his own weaknesses. At the same time he has the need for this relationship “This is my confusion and dilemma”. A similar pattern is demonstrated with other relatives. The episode of the bungalow purchase is an expression of his impulsive nature as well as his feelings for his parents. With this understanding Kali-iod was selected as his constitutional. The other durgs which came up for differentiation were Mercurius, Anacardium and Lachesis.
Anacardium is indicated because of cruel behaviour, violence and impulsive attitude. A vicious anacardium can be malicious and scheming. Hering describes this as : “estrangement from society and individuals. He is very indifferent and unfeeling.” But our patient demonstrates an emotional need for relationship.
Mercurius and Lachesis enter the fray with ego and violence. Intense need for relationship, complaining attitude and anxiety about health helped decide on KALI-IOD.
The following references gives us the depth to image the mental picture of Kali Iod that he presented:
Hering:
Talkative, disposed to jest.
Starts at every noise.
Excited as if intoxicated.
Frantic excitation, catarrhal or mercurial headache.
Inclined to be vexed, vehement, quarrelsome.
Very great irritability and unwonted harshness of demeanor, his children, to whom he is devotedly attached, become burdensome to him, very passionate and spiteful temper, inclined to sadness and weeping, with constant apprehension of impending evil.
Melancholia.
Torturing feeling of anguish preventing sleep.
Whining, apprehensive as from threatened accident.
Sadness and anxiety.
Phatak
Irritable, irascible esp. towards his children; his family. Harsh tempered and cruel. Trivial details of life seem insupportable. Cannot think. Despondent. Bad temper. Abusive. Nervous, must walk. Talkative, disposed to jest.
Robert: Differential Material Medica:
Mean, selfish.
Kent:
This remedy has a peculiar mental state. There is a very strong degree of irritability, cruelty, and harshness of temper. He is harsh with his family and with his children; abusive. It will take all the sense of refinement out of his mind and then he will become sad and tearful. Extremely nervous, and must walk and be on the go. If he remains in a warm room he becomes weak and tired, and feels as if he could not stir, does not want to move, and does not know what is the matter with him.
Investigations done:
1) During admission
23/03/94
- BS fasting – 229 mg/dl
- BS PP – 270 mg/dl
- urine fasting – sugar ++
- S. Bilirubin total 1.2 mg/dl
- Direct – 0.33 mg/dl
- SGOT – 24 u
- SGPT – 52 u
- Hb – 15.4 gm% WBC – 10,100/mm N66 E, L33
- S. amylase – 91 SC units / 100ml
2) During stay in hospital
30/03/94
- BS fasting – 92.8 mg%
- BS PP – 321 mg%
- S. amylase – 87.5 SC units/100 ml
05/04/94
- BS fasting – 235 mg%
- BS PP – 336 mg%
09/04/94
- BS fasting – 150 mg%
- BS PP – 205.5 mg%
18/4/94
- BS fasting – 157 mg%
- BS PP – 328 mg%
- S. amylase – 96.5 SC units/100ml
Philosophical Analysis:
Deciding on the remedy is only half the work done in situations like these. Before we see the follow up management, it is important to get a good philosophical grasp of the pathology one is dealing with in order to have a good long term management strategy. As a teacher, this is how I teach my students to handle serious pathology in any clinical setting.
First, we need to understand the pathology one is dealing with:
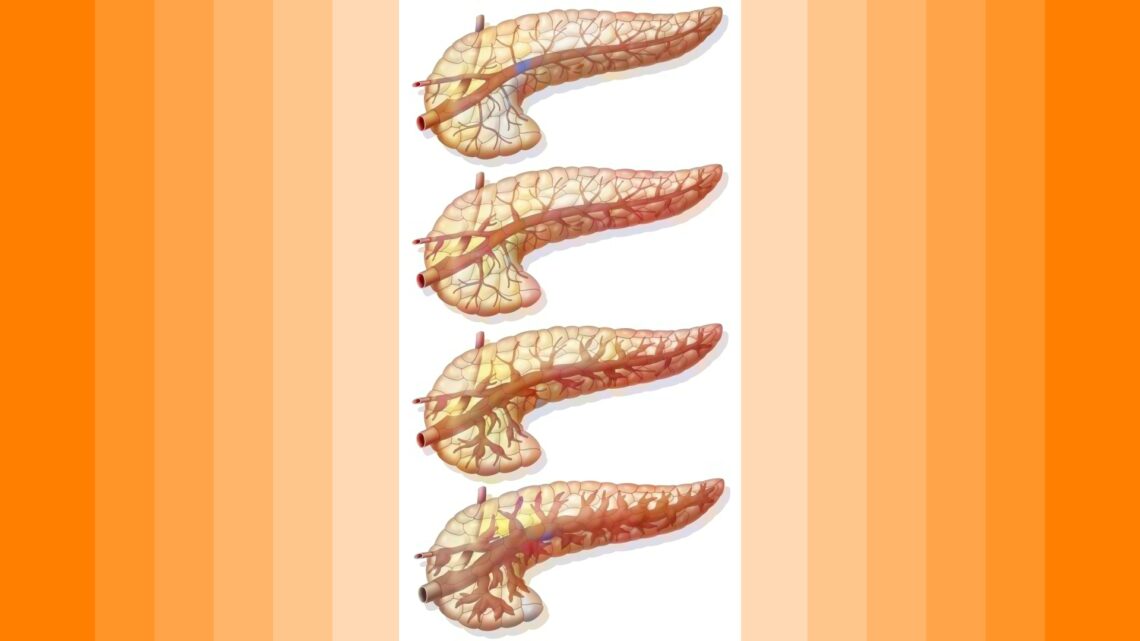
 Chronic pancreatitis (CP) is an inflammatory disease of the pancreas which leads to persistent and progressive morphological and functional alterations of the whole organ. In the terminal state of the disease the extended fibrosis leads to exocrine and endocrine pancreatic insufficiencies. Histomorphologically, the chronic inflammation of the pancreas is often characterized by:
Chronic pancreatitis (CP) is an inflammatory disease of the pancreas which leads to persistent and progressive morphological and functional alterations of the whole organ. In the terminal state of the disease the extended fibrosis leads to exocrine and endocrine pancreatic insufficiencies. Histomorphologically, the chronic inflammation of the pancreas is often characterized by:
- pancreatic head enlargement
- calcifications
- pseudocyst formation
- fibrosis and atrophy
The leading clinical symptoms in chronic pancreatitis are upper abdominal pain and maldigestion.
I like to use a clear concept of form-function-structure in every clinical situation I encounter as it helps us to get deeper insight to the clinical state that needs to be cured. Once the patient presents with complaints, it is important for the clinician to comprehend the degree/level of disturbance in function as well as nature of changes in the tissues and organs responsible for this symptom expression. I will explain how I use this concept.
What is perceptible to the homeopath are the external signs and symptoms. Based on this we recognize the disease and perceive it as a FORM (symptom expression) that evolves over a period of time. This expression keeps changing as the patient interacts with his environment. Ultimately changes in STRUCTURE take place. In other words, changing FORMS express themselves to us through disease complaints which result in structural changes over time. When we appreciate the interrelationships between these various expressions, we perceive a PATTERN in the expression of this form – which is the symptom picture that indicates a similimum remedy.
Diseases arise due to a fault in the functioning of a system. Thus a FORM is an expression of disturbances in the organ function. These disturbances of FUNCTION over a period of time produce a disturbance in the STRUCTURE and then, the latter aggravates the former. Thus a vicious circle is set up in chronic diseases. Again both these disturbances are revealed to us through changing complaints –> changing FORMS (pictures).
In other words, as the disease progresses, it is revealed to us in a continued change in FORM, FUNCTION AND STRUCTURE. It is important to have an integrated understanding of this phenomenon for management of serious diseases.
Based on an understanding of this inter-related phenomenon, one can arrive at logical formulations about following homeopathic parameters:
i) Susceptibility of the patient:
– Seat of disease
– Nature of changes
– Rate of changes –> pace of disease.
ii) Miasmatic diagnosis: Identification of the dominant miasm as well as degree of miasmatic activity.
iii) Posology formulations
iv) Phase diagnosis: Accurate identification of the current phase for a remedy choice :- constitutional , chronic, acute or purely antimiasmatic. We also get insight about possible pattern in which the case might unfold –> future projections.
Now, let us apply this model to appreciate different clinical patterns of chronic pancreatitis:
A) The Form: is the acute sudden expression of excruciating abdominal pain extending to the back. This is often precipitated by increased consumption of alcohol .
The Funtion: Raised Serum Amylase Levels with indigestion.
The Structure: Acute inflammation of ductal and acinar cells which over time undergo fibrosis following frequent relapses.
* Phase – Acute exacerbation of relapsing pancreatitis
* Susceptibility – moderate to high
* Miasm – Acute exacerbation of tubercular miasm.
* Therapeutic planning: Quite often a stong expression of Form in which the Pain expression dominates and requires an acute medicine like Chelidonium, Colocynth, Mag phos., Phos etc. When gastric irritation is a strong concomitant, which it was not in this case, IRIS, NUX VOMICA, Arsenic alb etc. would be indicated.
* If pain is not clearly defined, it is desirable instead to start with a constitutional remedy.
* If an acute is prescribed, it should be followed sooner rather than later, with the chronic constitutional , while keeping track of the changes in serum amylase level .
* Constitutional medicine: 200 potency or higher and requires INFREQUENT DOSES
B) The Form: This has relapsing features:
– severe epigastric pain with or without radiations
And constant features:
– Weight loss
– Abdominal bloating
– bulky foul smelling stool with oil droplets
– Polyurea/Polydypsia
The Function:
Increased Serum amylase
Poor Digestion and absorption
Impaired metabolism
Raised blood sugar
The Structure: 80% PANCREATIC FUNCTION DESTROYED
Phase : Chronic expression.
Hence, initiate treatment with chronic/constitutional .
Susceptibility : Moderate to Low
Miasm : Advanced Tubercular miasm
Posology : 30 potency (medium to low) and will require frequent repetition.
Prognosis & Homoeopathic Projections:
According to modern medicine, Chronic pancreatitis implies the presence of irreversible damage to the pancreas. In the presence of diabetes mellitus and pancreatic insufficiency, the prognosis becomes guarded. The survival rate in some series in the presence of such complications is less than 10 years. Classical Homoeopathic experience is otherwise. The following points should be kept in mind for management of Acute on Chronic Pancreatitis:
* The Susceptibility here is moderate to low. So one must start with the 30 potency of constitutional and gradually build up the repetition depending on the sensitivity of the system.
* Judicious use of Tuberculinum bov. as the intercurrent antimiasmatic helps a lot in improving the susceptibility of the patient.
* They may present with an acute exacerbation of symptoms. In such instances, if a clear cut Form is expressed, only then treat that phase of symptom expression with a different (acute)medicine; otherwise it’s advisable to enhance your repetition or potency of the constitutional remedy instead.
* During course of treatment, they may present with episodes of loose motion; DO NOT TREAT THIS WITH UNNECESSARY SUPERFICIAL MEDICINES
* Often they develop skin rashes. Here one must learn to differentiate between exteriorization of symptoms, and opportunistic / staphylococcal and fungal infections due to Diabetes Mellitus or poor general health and hygiene so take appropriate measures.
Education and Ancillary Measures
The cause of chronic pancreatitis, which is invariably alcohol , should be emphasized. The patient should be told that unless alcohol consumption is discontinued, no improvement can be expected. An explanation of the various complications encountered with chronic pancreatitis should be explained to both patient and family.
* Treat rationally the Diabetes mellitus, if necessary, with required doses of INSULIN. Gradually taper off insulin as pancreatic function improves.
* Pay attention to protein diet and diabetic diet.
Let us understand the intricacies of the philosophical explanations above through the management of this case.
Follow up Synopsis for 1st 1 month of treatment :
23/3/1994 to 26/4/1994
Since the patient was admitted with an acute excruciating pain which made him quite restless, the first line of treatment was an acute remedy. This is typical of the type A expression of Form – Function – Structure explained above.
The analysis of his symptoms indicated Colocynth. It was given in 200C 2 hourly. With no significant relief after 4 doses, he was switched over to Mag Phos 200 2 hourly and later 4 hourly. There was significant relief in his distress within 4 hours but the Mag Phos 200 4 hourly was continued for 3 days.
Now was the need to start the chronic remedy as the constitutional features were beginning to become more evident.
The KALI-IOD 200 was given at bed time every night, while the Mag Phos was going forward. Later Kali Iod was increased to a b.i.d. [two times a day] and then t.d.s.[three times a day] dosage.
Tub bov 1M 1 dose interpolated on 19/4/1994.
Other measures:
He was advised on other ancillary measures to support the healing process.
- Diabetic diet
- High protein diet
- INSULIN : Inj. Norsuline (Plain) 10 unitsInj. Monosuline (Lente) 16 unitsInj. Insulin doses were adjusted to regular investigation of blood sugar levels. Subjective features mentioned in the initial history promptly disappeared. Jaundice also improved. Serum amylase level was still high at this point of time.
Follow up Synopsis of the following 1.5 years of treatment:
27/4/1994 to 31/12/1995
* There was not a single episode of Jaundice or acute exacerbation of pancreatitis.
* He had recurrent bouts of loose stools which required Podophyllum 200 and later Podo 1M.
* On 9/11/1994 – He developed several boils all over the body which required Calcarea sulf 30 qds [four times a day] for a week.
* On 9/12/95 he had one episode of URTI [upper respiratory tract infection] that required Ars alb 200.
* Serum amylase returned to Normal by 6/12/1994 (42 SC units/100ml ), nearly 8 months after the start of treatment.
LFT and lipids became normal by 1/5/1995, a little over a year since Kali Iod was started.
Blood sugar remained stable in contrast to fluctuating, unstable levels before treatment began.
Fasting Sugar = 65 and Post Prandial = 70. Inj. INSULIN had to be reduced considerably to adjust to the new sugar levels.
* Over all his irritability and mental state improved quickly in the initial phase of treatment, but his relationship with his wife remained almost the same. His wife ran away to her parents place at Bihar. The patient went to bring her back but he was very angry with her. He felt like killing her! He even got into a physical fight with his brother-in-law who tried to defend her. Both were in an enraged state of mind and the patient stabbed him. Luckily the Brother-in-law survived. But the patient turned himself in and was arrested. He was sent to jail for 3 months.
* From 27/4/1994 to 9/8/1994: He was on Kali-iod 200 4 hourly.
Tub bov 1M was interpolated twice
* From 9/8/1994 to 31/12/95: The potency was increased to Kali-iod 1M 1 dose every night. During this phase the Laboratory Parameters began to improve and returned to normal .
* From 1/1/1996: all active medication was discontinued as he remained stable and normal clinically as well as from biochemical angle. His L.F.T was rechecked and it was W.N.L .
* 10/2/1999: He brought one of his neighbours for treatment with us. We observed that the patient had mellowed down considerably. This was also attributed to his parents demise. He had developed Grief++, Guilt+, “I did not listen to my Father”. His wife had left him and he felt very lonely. His Diabetes Mellitus remained under control . He had no other health problems.
References:
1. Medicine for Practising Physicians: J. Willis Hurst
2. Text book of Pathology: Willium Boyd
4. Materia Medica: Hering, Phatak, Robert, Kent.
5. Chronic Pancreatitis: New Pathological Aspects, Shailesh Shrikhande, Helmut Fries, Marcus E. Bombay Hospital Journal Vol .44 – No.4, 1999.
This article was published in ijhm vol . 33 issue 1/2000-2001
Dr. Praful M Barvalia, MD(Hom)
Shalibhadra Society
148, Hingwala Lane Extention
Near Popular Hotel
Ghatkoper (East)
Mumbai 400077
Ph: 91-22 – 2516 5985
91-22 – 2513 4467
Email: [email protected]
[email protected]
Website: www.holisticfoundation.org

Hello Dr.Praful,
What would be your method of treatment for idoapathic pancreatitis?
Please email me to my email given above.
Thanks!
Hi praful . Thanks a lot for the information. When there are multiple calculai inside the main pancreatic duct and the the duct is dilated then how to remove that calculai ? What would be your method .
Thanks in advance …..
Hi Doctor,
I’m suffering from CHRONIC PANCREATITIS for the last 13 years and done one major SURGERY.
Shall I marry? If I marry somebody, then what will be the reaction?
No medicine cured me. I ve suffered alot.
Pls give me solution
Hi Doctor,
I have been dignosed CHRONIC PANCREATITIS few days back, with calcification and dilated pancreatitic duct 9.3 mm. sugar level are normal.
Can u plz tell me whether it is detected early or it is late??
Pls give me solution, what to do,
thanks in advance.
Regards. rohit
hi doc..im siddesh .im student ,graduating civil engg.my age is 22.im suffering frm pancreatitis frm past 5 years,and calcification was noticed in head and body of pancrease frm past 4 years.can i go with surgery ?will my digestion ability increases aftr surgery or should i take oral enzyme life long.im still young im sacred of surgery.is there any alternate solution other than surgery?im not alcoholic i hav not tasted tht not even one time.hw did i get this disease ?im very lean .how can i improve my body?how to gain weight?im very much tired of this disease .pls pls share ur knowledge wit me. Thanking u .pls do replay .im waiting…… .siddu
Sir,
My daughter aged 27yrs suffering from chronic pancreatitis and a duct dilated last two years. She is marrd . Can she go with surgery? Will my digestion improve after surgery. Should I take oral enzymes life long, and there any solution in your homeopathy treatment? Please reply me on my mail . For this I shall be ever grateful to you.
GERD WITH CHRONIC PANCREATITIS
I am 50 yrs old suffering from gastric troubles excessively for last 8 months having so much belching, heaviness at pit of stomach and indigestion.
Endoscopy (20 -05 -2013) reveals GERD since then I m taking PPI daily and USG shows – a circumscribed hypoechoic lesion measuring 21mm – 19.9 mm in body of pancreas, which is avasular .No pancreatic fluid or calcification detected . No dilation of MPD.
CECT abdomen done shows No significant abnormality. but same time test showed raised serum lipase ,amylase and CA 19.9 ,which were normalized in next month.
Endoscopic USG shows pancreatic mass, inflammatory? neoplastic?
FNAC also done suggest chronic inflammatory lesion, No evidence of cancer in specimen.
Meanwhile blood sugar also shot up as I was already diabetic, had not control from hypoglycemic drugs. so started mixtard insulin 20 unit daliy.
MRI + MRCP whole abdo ( 13-08-2013 )shows – tiny calcific focus is seen in tail region .
Now retesting USG at every two months , the lesion is same in size….No progression and No regression..
During last 8 months of my illness , I had changed so many doctors, tried all medical science and read so many articles on web. All these resulted depression and persistent thought of incurability and even thought of suicide also, as some where I read pancreatitis is incurable and can become malignant. Doctors prescribed me anti-depression .
Now a days condition is better but gastric trouble and gas formation in stomach, belching and feeling of heaviness is persistent.
I came to know about u Sir, I want to know about the following-
1. Is there is any relation between GERD and ch. pancreatitis?
2. How this gastric trouble can cure?
3. What is prognosis of this ch . focal calcific pancreatis, what are chances of its malignancy?
4. Can this lesion shown in USG cured?
5. What is your advice ragarding this?
kindly , help me out from these question of my mind. A big hope from u sir !!!
Thanking u !
with regards
My son 11 yrs is suffering frm chronic pancreatitis is there treatment in homeopathic
I’m suffering from chronic pancreatitis last 3 years
Sir I am suffering from chronic calcified pancreatitis from 1 year stone in head.Can it be completely curable in homeopathy…