Name : Mrs. D. T. with her baby d.
Age : 30 years
Sex : Female
Religion : Hindu
Occupation : Nurse in Dhoot Hospital
Date : 26 / 10 / 2009
Chief Complaints : ANC second trimester, with fetal Anomalies.
| Location | Sensation | Modalities | Concomitant |
| Palms & soles | Burning | – | – |
Past History :-
LSCS 12-13 months back, Child died after 2-3 days.
LSCS was done due to irregular contractions, os did not open and labor did not progress.
H/O Polyhyramnios.
H/O high BP with swelling over both legs.
H/O fall in FHR i.e 30/min.
Family History : Brother – piles.
Physical General :
Weight – 34 kg.
Appearance :- emaciated, thin, short built dark complexion lady.
Appetite : good
Thirst : Thirsty+
Desires : spicy/pungent, earth, meat, methi (green vegetable).
Aversion : sweet, milk, eggs.
Diet : both
Tongue : Clean
Urine : NAD
Stool : Hard stool
Perspiration : Nil
Bath : Warm water
Fan : Wanting
Coverings : seasonal.
Sleep : unrefreshing. Feels tiredness.
Dreams : God, death of her relatives, running water and snakes are
coming towards her when she is traveling in bus.
Thermals : Hot
Menstrual History : Regular. LMP – 08/05/2009
Physical examination :
Temp : Afebrile
Pulse : 76 / min
B.P : 130 / 90 mm of hg
Systemic examination :
R.S : Clear
CVS : S1 S2 Normal
CNS : NAD
GIT : NAD
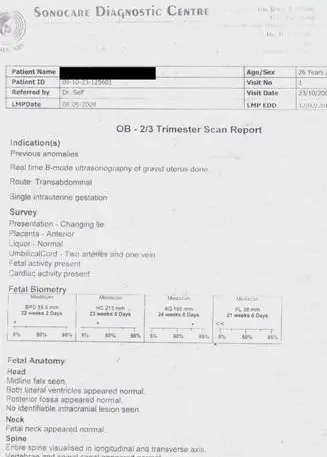
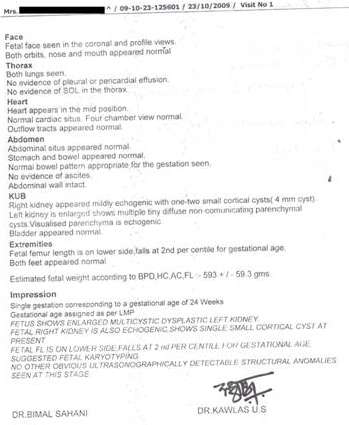
Investigations: OB – 2/3 Trimester scan Report ( 23/10/2009)
Impression :- Single gestation corresponding to a gestational age of 24 weeks .
Gestational age assigned as per LMP.
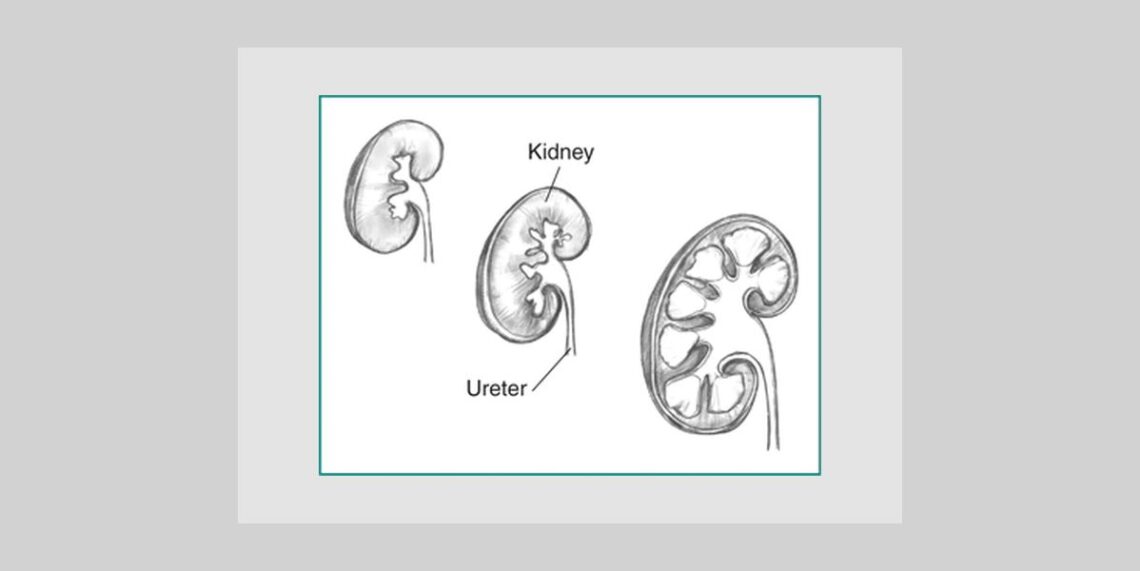
Fetus shows enlarged multicystic dysplastic left kidney.
Fetus right kidney is also echogenic and shows single small cortical cyst at present.
Fetal fl is on lower side, falls at 2nd percentile for gestational age.
Suggested fetal karyotyping.
Scaned copy is given below
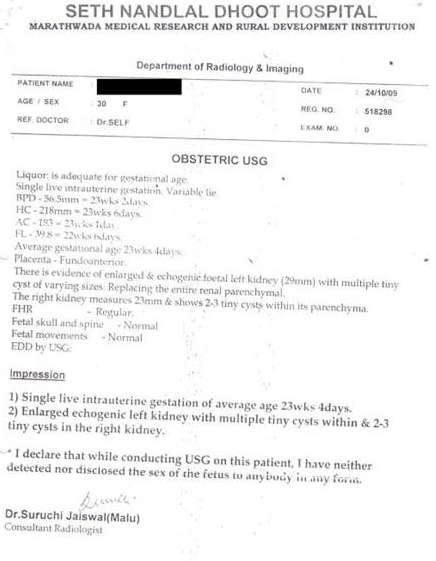
OBST. USG:- (24/10/2009)
Impression:- Single live intrauterine gestation of average age 23 wks 4 days.
Enlarged echogenic left kidney with multiple tiny cysts within replacing the entire renal parenchyma & 2-3 tiny cysts in right kidney.
Scaned copy is given below
Analysis of Mental traits :-
Anger after contradiction. Becomes aggressive and goes into either indignation with guilty feeling that I must not get angry, or throws things which are in hand and remains silent. Wants to beat that person who has contradicted her.
There is history of vexation from her in-laws.
Diagnosis of Disease : ANC with Fetal multicystic Dysplastic left kidney.
Phase of Disease : Chronic Reversible
Diagnosis of miasm : Fundamental – Sycotic
Dominant – sycotic
Diagnosis of susceptibility : Moderate.
Opinion of gynecologist and nephrologists – Suggested to terminate the pregnancy as it could be IUD or it may survive after delivery.
Diagnosis of Remedy : Nat.mur 10M . 1 dose, followed by silicea 3X TDS for 15 days.
Follow up Chart :-
| Date | Observation | Prescription |
| 11/11/09 | Wt – 36kg.
H/O one episode of vertigo while walking. H/O Vomiting one episode. Palms & sole burning >+++ Dreams reduced. Sleep sound. |
S.L |
| 12/11/ 2007 | USG – obst : – Single live intrauterine gestation of average maturity 25 weeks 2 days.
Foetal left kidney is enlarged with multiple cysts are seen at periphery. Two tiny cysts are seen in right kidney. |
Medorrhinum 200 1 dose. |
| 23/11/ 2009 | No any new complaints | Nat. Mur 200 1 dose . |
| 02/12/ 2009 | Pain in lumbar region since morning
> lying on back. PV – White sticky discharge. Frequency of micturation increased. No /H/O – PV – bleeding. Fetal movement is normal. Cervix is closed. Adv – Obt USG. |
Nat. Mur 200 1 dose with water. |
| 03/12/2009 | OB – 2/3 Trimester scan report.
Single gestation corresponding to a gestational age of 29 weeks 6 days. Breech presentation. Fetus show bilateral echogenic kidneys. Multiple tiny cysts in right kidney F/S/O ? mild degree multicystic renal disease (right) with echogenic left kidney. Sever oligohydramnios, AFI – 4.5 |
S.L |
| 14/12/2009 | No any complaints.
USG Obst – Sever oligohydramnios; AFI – 4 H/O PV – white sticky discharge. Gynecologist opinion – e/o some vaginal infection white discharge present. |
Nat. Mur – 10M 1 dose. |
| 20/12/2009 | Labor pain – irregular.
1 finger dilatation of cervix. |
Caullophylum 200 2 dose, Pulsatilla 6 c 6 dose / 4 hrs each. |
| 21/12/2009
9Am |
Irregular labor pain.
2 finger dilatation of cervix. Gynecologist Adv – for LSCS. Red discharge +,Thirsty , hungry feeling , weakness +. Direction of pain – weak irregular pain arising in back extending downward going to front & extending upward. |
Kali. carb – 200 in water / 10min.
Time – 9Am. |
| 21/12/2009
12 MD |
Complete regular contraction+++
Full dilatation of cervix. Membrane ruptured |
Stop Kali. carb |
| 21/12/2009
2 PM |
Normal delivery of male child at 1:45pm.
Wt – 1400gms Serum sodium – 121 mmol/L, serum potassium – 4.8 mmol/L, blood group – B positive. CRP – negative. Hb – 17.4 g/dl. |
Arnica – 200 1 dose for both mother & child.
Child was sent to NICU. |
| 22/12/2009 | Child passed urine multiple times
And stool 2 times. Sr. bilirubin total – 6.59 mg%. |
Aconite 200 1 dose olfaction. |
| 23/12/2009 | Child passed urine multiple times
No e/o swelling over legs or face of child. Sr. bilirubin total – 8.53 mg%. Sr. creatinine – 1.7 mg/dl morning. Evening : Sr. sodium – 101 mmol/L; Sr. potassium – 8.1 mmol/L |
Natrum mur. – 30 1 dose in mother milk. |
| 24/12/2009 | Child passed urine multiple times
No e/o swelling over legs or face of child. USG of child – Right kidney appear normal except for two tiny cysts. Left kidney show e/o numerous small cysts s/o ? multicystic kidney. Pediatrician and nephrologist suggested to discourage treatment as above all investigation was s/o prerenal failure. |
Discharged from NICU.
EEL serum 30 with water twice a day for 2 days. |
| 26/12/2009 | Child passed urine and stool multiple times.
No e/o swelling over legs or face of child. |
Urea pura – 30 BD X 3 days. |
| 29/12/2009 | Child passed urine and stool multiple times.
e/o swelling over both legs + |
Natrum mur. 6 c BD X 4 days |
| 1/01/2010 | Child passed urine and stool multiple times.
Swelling of both legs regressed. e/o swelling below lower eyelids. Tongue reddish, central white. |
Natrum mur. 6 c OD X 4 days. |
| 7/01/2010 | Child passed urine and stool multiple times.
Swelling below lower eyelids regressed. – Hiccough ++. – Fever + – Wt. 1500gms |
Nat.mur 6 c , 5 dose every alternate day once in day. |
| 19/01/2010 | H/O fever for 2 days 10 days back
Weight increased by 200 gms. USG Abdomen & pelvis:- scan report given below
Blood urea – 17, Sr.creat – 0.9, Na – 140, K – 6.2 |
Nat.mur – 6c one dose every alternate day 10 dose. |
| 16/02/2010 | Crying+
Redness all over body+ Sweating on dorsal region+ Desires to be carried+ Aversion for milk of mother, throws out milk. Weight – 2250 gms. |
Silicea 200 1 dose. |
| 30/03/2010 | date – 30/03/2010.
blood urea – 18 creatinine – 1.1 sodium – 138 potassium – 5.3 |
S.L |
| 31/03/2010 | 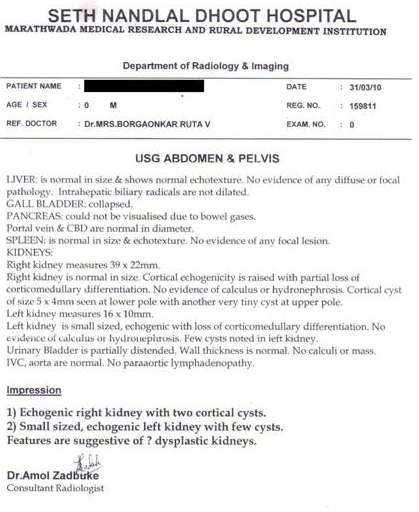 |
|
| 10/05/2010 | Coryza+
Nose obstruction+ Sneezing+ Fever with irritability+ Sweating neck |
Calcareaphos – 200 1 dose. |
| 05/10/2010 | No any complaints
Weight – 6.2kg |
S.L |

Comments :- It was the mother’s second baby ; first baby was expired after 2 – 3 days of birth but during that time no antenatal scan anomaly. Scan was done so its cause of death was undiagnosed. It was LSCS delivery.
This baby was diagnosed as multicystic dysplastic kidneys in fifth month of ANC.
Nephrologist and gynecologists suggested for MTP as baby will never survive. Mother decided on homoeopathic medicine with due consent of risk of baby as well as mother.
After birth baby went into prerenal failure and low birth weight (1400gms) with preterm normal delivery, though her previous was LSCS delivery. It was only due to homoeopathic medicines used during labor pain.
NICU management was discouraged by intensivists, Pediatrician and nephrologist, due to poor prognosis of baby. She decided to take home care for baby with homoeopathic medicine only. Since then baby is only on homoeopathic medicine without any help of NICU.
At present baby is well and gaining weight day by day without any sign of renal impairment,
though there are cysts in both kidneys . His recent weight was 6.2kg. Lastly I only want to say that homoeopathic medicine can not only help in labor, but also in early detected anomaly in ANC.

super case!!!!!!!!!!!!!!!!!!!!
dosta ekdam bhari case ahe.keep it up.
Sir, so great of you and homeopathy.
wow! u have done great job…
Thanks
What homeopathic remedies were used? I am 20 weeks and want to reverse his Multicystic in his left kidney 6 cysts