– Deciding not to be a homeopathic Sherlock Holmes
– The Chronic Diseases – a difficult read
– Pathology – a hit and miss affair
– Why did essence take off in the first place?
– Why should a ‘well indicated’ remedy fail to relieve?
– The most effective prescription matches the totality of symptoms and the dominant miasm
– The benefits of HFA
Homoeopathic Facial Analysis (HFA) began from the simple questions: ‘What exactly is a miasm?’ and ‘Does miasmatic knowledge have any real clinical value?’ The nature of these questions also says a lot about what type of practitioner I was at the time. Like a number of homoeopaths, I knew about the miasms and I thought I understood the philosophy behind them, but in reality I rarely employed miasms as part of my clinical prescription.
From the 1980’s and into the 90’s I saw every homoeopathic speaker I could. Regardless of the topic, I was in the audience furiously writing notes and trying to commit the speaker’s information to memory. My aim was to understand homoeopathy and to have it clearly defined in my mind, to be able to use it and be clinically effective. It didn’t matter that many of the speakers were saying different things, nor did it matter that many were contradicting the speaker before them. All that mattered at that time was volume, the quality of information seemed less important than amassing a quantity of it.
Over time there I was with ten years of homoeopathic practice under my belt, mountains of written notes and tapes yet just as confused as ever. New theories were coming in so thick and fast, that I barely had enough time to keep up with them. Then, although I did not know it at the time, I made a life changing decision. I decided after seeing a speaker, yet another one who presented a number of cases in which none of the audience – me included – came even close to selecting the ‘right’ remedy, that I did not have the right type of mind or observational skills to ever be proficient in spotting the ‘subtle differences’ in patients and remedies, that I needed to be a master. This decision although deflating at the time, is one of the best homoeopathic decisions I ever made.
Because I was never going to be the homoeopathic Sherlock Holmes I originally desired to be, I focused instead on being thorough and deliberate. I may not have been able to distinguish one ultra-fine subtlety from another, but I was a hard worker. I decided that while I could never be one of those homoeopathic ‘magicians’, I knew I could be a solid and competent practitioner, provided I followed the homoeopathic ground rules.
At that point in time I was teaching undergraduate homoeopathy with my focus on the classical rather than the intuitive, which suited my personal preference. In my mind, if I was going to be a solid practitioner I needed to focus on the system rather than on the subtlety, and that meant going back to basics – another great homoeopathic decision unrecognised at the time. While going through the 6th Edition of the Organon with one of my classes, I was struck by the emphasis Hahnemann placed on his miasms and how they should form the foundation for each constitutional prescription. Before this point I would have sworn black and blue that I already knew that fact, but there is a vast difference between knowing and really understanding.
At this point I must also confess that I find Hahnemann a difficult read. The Organon is hard enough but The Chronic Diseases are worse. It’s not his philosophical theory so much, but trying to find the miasmatic patterns Hahnemann claimed existed. For me, clarity about the miasms came from authors like J.H.Allen and Herbert Roberts, because they defined the patterns Hahnemann was seeing, more clearly than Hahnemann himself. While Hahnemann’s three miasms remain the foundation, it is Allen and Roberts who are the key to this new system. It was they who showed me Hahnemann’s patterns – the outward motion of psora, the inflammatory and capturing action of sycosis and the inward nature of syphilis. However there was an even more intriguing area these authors introduced me to, and that was the idea of a miasmatic relationship to facial features.
I found this relationship so intriguing that I decided privately to research this idea. If it turned out to be a waste of time – so what, what have I lost? But if it was true it could be a great help to finding the miasm of a patient. Taking a guess at what miasm is dominant via a patient’s presenting pathology, is a very hit and miss affair. Even Boenninghausen, who was Hahnemann’s greatest fan said it couldn’t be done. At the same time, every chronic prescription is meant to start by knowing the miasm of the patient. If facial features could tell me, what a great advantage I would have.
It has now been over nine years since the origins of facial analysis began, and the knowledge and results that have come from it have been nothing short of remarkable. Homoeopathic Facial Analysis is homoeopathy made easy – or at least as easy as something as complicated as homoeopathy can be.
HFA employs all the traditional polychrest remedies together with standard repertorisation techniques so there is no need to re-learn any new concepts. Homoeopathic Facial Analysis is an addition to classical homoeopathy, it is not a replacement. It allows for the traditional homoeopathic system of finding the Simillimum by mentals, generals and particulars rather than by essence. For many, and I am one, essence is too hit and miss and relies on interpretation.
If essence prescribing is so hit and miss, then why did it take off in the first place? The reason is because finding the Simillimum through signs and symptoms alone is no less of a hit and miss affair than essence prescribing. Both are searching for that needle in a haystack. The Simillimum sounds easy theoretically; all you have to do is match the symptoms of the remedy to the symptoms of the patient, but it is not that easy in practice. The case is taken and the repertorisation completed. You choose the remedy and the match looks good. You select your potency and give it to your patient – then absolutely nothing happens – why?
Historically the answer was unknown, which is why essence prescribing developed. If the symptom totality matched, something else must be missing otherwise the Simillimum would have worked. Some practitioners blamed the system and many left in droves during the late nineteenth and early twentieth centuries. Others had enough success to know that homoeopathy itself was not to blame. Some searched for more remedies, some for better provings. Others claimed the cause of the problem lay in the finesse of the practitioners themselves. These practitioners believed there was a subtle quality to every medicine that could only be understood by true masters of the art, or by those sophisticated enough to perceive it. This was, and still is, the ‘essence’ of essence prescribing. It can be very hierarchical and very conceited.
Over the course of homoeopathic history there have been many who have criticised essence prescribing, but that does nothing to explain why the Simillimum did not work. Why are there libraries of old homoeopathic books littered with the phrase ‘When the well indicated remedy fails to relieve?’ Why should a well indicated remedy fail to relieve? We read it everywhere in the old texts; remedy X completes the action of remedy Y when remedy Y fails to complete the case.
One of my favourites for learning Materia Medica’s back when I was a student, was Clarke’s 3 volume dictionary. I loved it because it was full of vital information such as triangles of remedies, relationships of remedies, what remedies follow well, are followed by and antidote. For years I studied remedies this way and felt I had a good appreciation of materia medica, but that has changed since developing HFA. Before, I accepted that a well indicated remedy may not do the task required of it. Its response could be wonderful, partial, superficial or non-existent, but that theoretically still did not mean that I had chosen the wrong remedy. So un-phased, I would search for my original prescription’s compliment that followed well. I no longer believe this is the right thing to do.
After becoming proficient at analysing facial features the need to ‘follow on’ became less. Rather than applying a philosophical construct to the clinic, HFA techniques developed the other way around and came from clinical results. The philosophy of ‘how and why’ did not develop until later. This is the opposite of many new methods that start from an idea that is then clinically applied. Homoeopathic Facial Analysis began as an experiment to see whether the theories proposed by Roberts and Allen were valid. Later and only when my clinical success became so undeniable, did I develop a philosophical construct to explain the successes I was having.
HFA started by analysing the facial features of patients who had substantial benefits from remedies unquestionably miasmatic. By this I refer to remedies whose miasmatic dominance is universally accepted within the profession. Sulphur is dominantly a psoric remedy while Thuja is accepted as being dominantly sycotic. In these instances dominance implies that while there may be other miasms in the remedy, the majority of a remedies action belongs to one miasmatic group in particular. This was important; I was trying to investigate any link between miasms and facial features, under the assumption that a remedy that is miasmatically dominant helps a patient significantly in the treatment of chronic disease because the remedy and the patient are dominant in the same miasm.
My most important cases were the patients who improved dramatically under the one remedy, but not always the one dose. This philosophy came from Hahnemann, who believed that not only were remedies dominant in one of the miasms, so was pathology, and later according to Allen and Roberts so too were people. Chronic disease is caused by an underlying dominant miasm and facial features are shaped by the same influence. By analysing the facial features of patient’s who responded in a significant way to miasmatically categorised remedies, a catalogue of facial features representing each miasm was eventually formed.
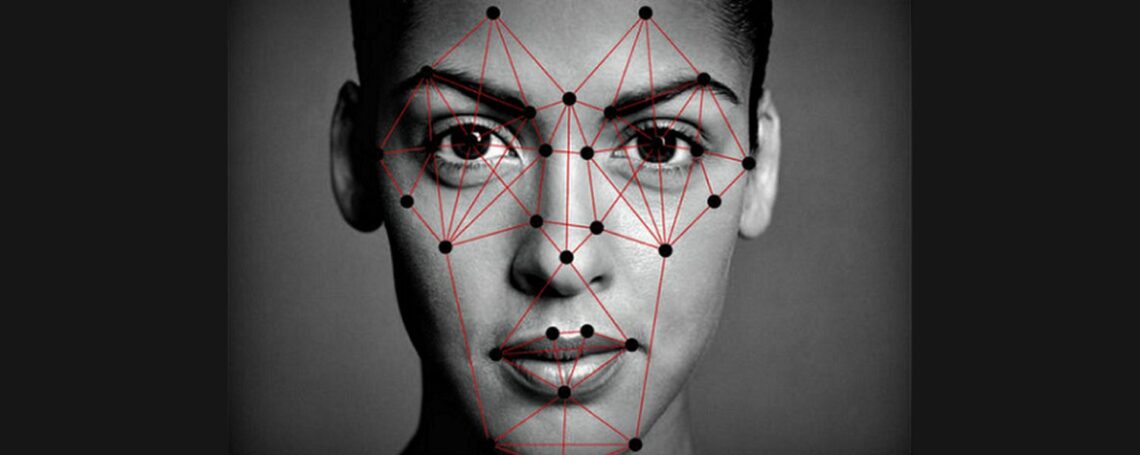
Here is how HFA works. By analysing the facial features of sycotically dominant patients, we can catalogue what features they all have in common. The practical value is that these same features can be used in reverse to identify sycosis. Finally homeopaths have an objective diagnostic miasmatic tool that can be easily applied in the clinic.
Common sycotic facial features include; a single line between the eyes, a straight hairline from one temple to the other and gums that show on smiling. By observing these features in a patient, we can tell before giving our prescription that a sycotic remedy is required. This makes prescribing much easier and far more effective, and here’s why. The miasm is the driving force behind chronic disease. This means the most effective prescription is the one that matches the symptom totality as well as the underlying dominant miasm. Usually practitioners just rely on symptom totality alone but with Homoeopathic Facial Analysis we can do both.
The benefits of using HFA are numerous. Some of these benefits include:
-
· Reliability – Homoeopathic Facial Analysis is completely reproducible
-
· Speed – case taking is much quicker using HFA
-
· Observation – HFA is one of the few objective confirmatory tools available to contemporary homeopaths
-
· Improved results. Because each prescription includes the totality of symptoms together with the dominant miasm, clinical results in chronic disease improve markedly and rapidly
-
· Generals : While mental rubrics are important, the generals are vital because they lack the interpretation needed to make mental rubrics accurate. While the origin of a mental state can be speculative, generals are always obvious. Practitioners can agonise over the cause of a belief but, “aggravation after eating” is straightforward.
-
· Simplicity – with HFA homeopaths can re-employ standard case taking the way it was practiced in the past
Without a definitive way of defining a miasm, diversion from traditional mentals and generals prescribing was inevitable, due to the historically random nature of symptom totality prescribing in chronic disease. One or two mentals combined with four to five generals may have been the foundation of homoeopathic prescribing for chronic disease, but it left too many possible remedy choices despite its ease and safety. This is no longer a major problem when using facial analysis to determine the dominant miasm. Standard repertorising usually leaves ten or more possible remedies. The key to HFA is observing and knowing the dominant miasm of the patient before selecting the remedy.
If for example, of our ten possible choices only three of those remedies are sycotically dominant, and we can tell by the facial features of our patient that sycosis is their dominant miasm, then our remedy choice has been narrowed down from ten possible remedies to three. This is vital for practitioners, because while a number of patients are prepared to give us few attempts without success, hardly any will give us ten.
Homoeopathic Facial Analysis has not only been good for my professional esteem, it is a vital component for any homoeopath trying to build their business.
————————————————–
Grant has been working and studying in various fields of natural therapies since 1987. Grant’s qualifications include Homeopathy, Naturopathy, Clinical Hypnosis and a Post Graduate Diploma in Eriksonian Psychotherapy. Grant is the current Principal and senior lecturer of the Victorian College of Classical Homeopathy, a position he has held since 1995.
His first book, Appearance and Circumstance(2003) details the nature of miasms and how facial analysis can be used to determine the patient’s dominant miasm. Homeopathic Facial Analysis (2006) continues this work with detailed descriptions and examples of facial analysis. Soul & Survival (2008) defines how miasms influence us in our daily lives and define our individuality.
Grant has lectured in Australia, New Zealand, the Middle East, USA and Europe.
Further information about Grant Bentley’s research and his books can be found on the Victorian College of Classical Homeopathy website http://www.vcch.org/miasm.html and the Soul & Survival website http://www.soulandsurvival.com/


In India study of facial features, and entire body is a very old art. But detailed information may not be available in any of the Indian Universities, but one may be able to find in the Himalayas. More over I am not sure whether this art has been used for clinical purpose. There are people who can read mind also. I have come across technique through which one can see the internal emotional picture of a person. This I have tried once and it works.