Homeopathic Treatment in Patients at a Gastroenterology Institute
Abstract
Introduction: Aphthous stomatitis (AS) is the most common human disease of the oral mucosa with high prevalence and recurrence. Homeopathy is a very effective medical and scientific doctrine for acute and chronic diseases. Materials and Method: 22 outpatients with Recurrent Aphthous Stomatits (RAS) were treated. A homeopathic clinical detailed anamnesis was done. The homeopathic remedies chosen were generally administered at 200 CH potency. Patients had a monthly follow-up during 6 months or one year. Results: 50% of the patients had suffered aphthae during two thirds of their lives. We decided to include in this work the study of the miasm (background field) that prevailed in their family or personal antecedents. In family disease antecedents of the patients, the syphilis miasm prevailed as well as in the miasmtic sequence of the medications administered. From the beginning of the treatment, patients began to improve with regard to duration, size and frequency of aphthae. [59% of the patients were free from aphthae, in a permanent way, at two months of follow-up and 100% at 10 months.
Discussion: The predominance of the syphilitic miasm gives us clarity that treatment should give this miasm priority. The good results in patients with this miasm corroborates it. Conclusion: We consider that individual homeopathic treatment bearing in mind miasms, was very effective in RAS patients.
Key words: Recurrent aphthous Stomatitis, Homeopathy, miasms
Introduction
Aphthous stomatitis (AS) is the most common human disease of the oral mucosa (1-4) with 10 to 25% prevalence in general population and recurrence rates of even 50% in three months (1, 2, 5, 6). It occurs more frequently in women (7-9). Approximately 30-40% of patients with aphthous stomatitis have family past history of this disease (10).
Here we give some important definitions:
“Aphthae” means ulcer, and this term has been widely used to describe ulceration in mucous membranes.
AS is characterized by almost always painful little ulcerated areas in mouth mucosa. AS, in the acute stage, is a stomatology urgency (11). It is an acute inflammatory disease, characterized by one or more painful ulcers which may vary in form, number and size. They can be found anywhere on the keratined oral mucosa. Clinically we see one or various spherical vesicles, circumscribed, that break out suddenly after 24-48 hours and are replaced by a painful mucosal ulcer, that is yellowish with red edges (12-13).
Aphthae heal spontaneously in one or two weeks. Recurrent Aphthous Stomatitis (RAS) is characterized by recurrent tendency, multiplicity and chronicity, which distinguishes this disease from others that also have similar oral lesions, like, for example, viral exanthemas. Ulcers in RAS are not contagious and do not spread from one person to another.
RAS is a somewhat challenging pathology for stomatologists as well as for internists and gastroenterologists, mainly with regard to its etiology and treatment. The exact cause of aphthous ulcer is unknown. Multiple factors are suggested, such as stress, fatigue, hormonal changes, alimentary allergies, the foamy ingredient of toothpastes (sodium laurel sulfate), iron, zinc, vitamin B 12 and folic acid deficit (14-21). Even Helicobacter pylori is currently involved in the etiopathogenicity of ARS (20-22). Together with the factors explained previously, there is an alteration of the immunologic system in RAS, characterized by an exaggerated and continuing inflammatory response that favors the formation of the oral aphthae. Once the immunologic system is stimulated by the etiologic and precipitating factors, the immunocompetent cells that participate in the inflammatory response are activated and begin to liberate immunoglobulins and chemical substances that act as mediators of the inflammation (cytokines, complementary system components and free radicals, etc)(23-28).
Concerning treatment of Aphthous stomatitis, topical medications are generally the most commonly used (mouthwashes with diverse agents and topical remedies) to reach the immediate objective of relief from pain and to shortening the time of cure. However, these agents do not improve the recurrent rates (29). In RAS, it is necessary to use systemic medication.
Local treatment : Multiple medications of natural or synthetic origin have been used, such as local treatment with extracts of plants: Alchemilla vulgaris, Calendula officinalis, Symphytum officinale, Aloe vera, Commiphora molmol, Berberis vulgaris, Hamamelis virginiana, Baptisia tinctoria, Zanthoxylum clava-herculis, Sanguinaria, Thuja plicata, Melaleuca alternifolia, Satureja khuzistanica, Myrtus communis (Myrtle), Rhizophora mangle, glycyrrhiza (licorice), Hypericum perforatum (6, 30-53). Other local treatments are propolis tincture (54), steroids (55), Amlexanox (56,57), antibiotics ( 58,59) (doximicine,, penicillin), silver nitrate (60), ultrasound (61), laser(62), cryotherapy (63), etc.
Systemic treatment. Such is the uncertainty of its etiology that seventeen systemic medications have been prescribed for RAS in a compilation carried out by the Cochrane Oral Health Group (64) published in September 2012:
Beta-glucan (65) Clofazimine (66), Colchicin (66), Levamisol (67-74), Montelukast (75) Pentoxiphylline (76), Prednisone (75,77), Sulodexide (77), Camelthorn (an acasia type)(78), Homeopatía (79), LongoVital with vitamin(80) or alone (80,81), Propolis (82), Doxicicline (83), Tetracicline(84), B12 vitamin(85), Multivitamines (86).
To the above-mentioned, we can add:
Thalidomide, Azathioprine, Lactobacilus, Interferon, Vitamin C, Zinc, Copper (87-93) among others.
Another option of RAS treatment, very favored, are homeopathic medications.
Homeopathy (of homeos=similar and patos=disease) was founded by the German physician Samuel F. Hahnemann in 1796 (94).
Homeopathy is a medical, philosophical and scientific doctrine based mainly on the Law of Similars (the most important of the 8 basic homeopathic principles or laws) (95) which is enunciated:
“Apply against the illness to cure the medication that is able to cause another artificial illness the most similar possible, and the former will be cured.”
For homoeopaths, illness consists of the totality of symptoms (96). It is necessary that a detailed anamnesis of the totality of patient’s symptoms be taken, because the homeopathic medication is chosen based on that totality. For that reason, the medication that is given is individualized, only for that patient in that moment. The homeopathic remedies are prepared from mineral, vegetable and animal substances. Medications can also be prepared from morbid secretions or tissues such as pus, cancerous tissue, etc. In this case the remedy is called a Nosode (95). Nosodes can be used as any other homeopathic medication, if chosen from the patient´s symptoms, but they also have precise indications when personal or family antecedents of the illness itself exists, for example, tuberculosis (the nosode Tuberculinum), cancer (the carcinosinum nosodes), etc. and b) when a well prescribed homeopathic treatment does not show the expected results. In this case, nosodes acts to stimulate reaction.
Homeopathy treats both acute and chronic disease. Therefore homeopathic remedies are very useful both in the acute and chronic phases of RAS.
With the above mentioned information about homeopathy and its potential for treating RAS, we made a pilot study from 1998 to 2002 of 9 patients with RAS with a follow-up of 1 -2 years with very good results (97). Given the results of that pilot study, we planned this research.
Materials and Methods
Our patients came from several Stomatologic Clinics, from a Gastroenterology Institute or were referred by homeopaths from other centers. We made a clinical, homeopathic anamnesis, taking mental, general and local symptoms, as indicated in clinical homeopathy. We also asked for all the personal and family pathological antecedents. Of these, the most valid symptoms were chosen. Such symptoms were repertorized using the homeopathic software RADAR 7(98) that gives us the best remedies that cover the symptoms. Then we consulted several Materia Medica (it describes all remedies) to choose the most likely one.
The selected remedy was focused on constitutional treatment and it was generally administered at 200 CH potency. When necessary, the patient was also given remedy for the acute stage of illness (Borax or Mercurius solubilis 6 CH) for a few days.
Patients were seen monthly during 6 months or one year, to check symptoms, recurrences and to adapt the treatment to each new situation.
Results and Analysis
53 patients formed this group initially, of which it was necessary to eliminate 31 because they failed the follow-up.
22 patients were useful to be considered in this project.
The 22 patients had the following characteristics:
3.1 Age : The youngest patient was 9 years old and the oldest was 80. (Table 1)
Table 1. Age groups
| Ages | Number of patients |
| Less than 19 years | 4 patients |
| From 19 to 60 years | 14 patients |
| More than 60 years | 4 patients |
3.2 Sex: Female prevailed: 17 patients (77%) (Table 2)
Table 2. Sex
| Female | 17 |
| Male | 5 |
From the 22 patients, 5 (23%) had a follow-up during 6 months and the rest for one year.
3.3 Time of evolution of RAS disease.
It was from as short as 4 months to as long as 70 years suffering from RAS but, taking into account the relationship: patient´s age/disease duration, we point out that 50% of them suffered with sores during two third parts of their lives.
3.4 Previous treatments. Local treatment prevailed with laser or ozone.
3.5 Symptoms: Burning feeling and burning pain, mainly when eating, dryness of the mouth and halitosis.
3.6 Follow-up:
Table 3. Number of patients and percentage of symptom- free each month (accumulative)
Month No. of patients % that
symptom free represents
(accumulative) (accumulative)
| 1 month | 8 patients | 36 % |
| 2 months | 13 patients | 59 % |
| 3 months | 15 patients | 68 % |
| 4 months | 17 patients | 77 % |
| 5 months | 18 patients | 82 % |
| 6 months | 19 patients | 86 % |
| 7 months | 19 patients | 86 % |
| 8 months | 20 patients | 90,5 % |
| 9 months | 21 patients | 95 % |
| 10 months | 22 patients | 100 % |
| 11 months | 22 patients | 100 % |
| 12 months | 22 patients | 100 % |
Gráfico 1. Porcentaje de pacientes libre de síntomas por meses (acumulativo)
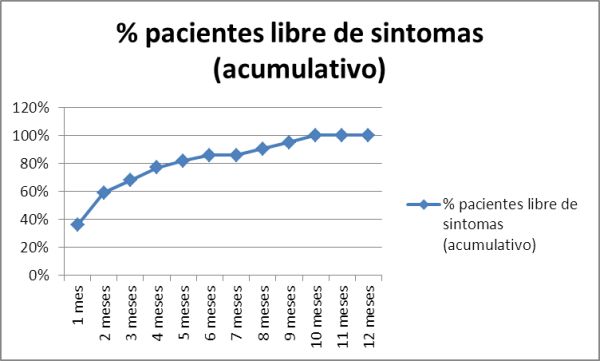
As we can see in the first month of follow-up, 8 patients (36%) were free of aphthae (they did not recur). The accumulative percentage of patients free of sores per month was increasing until achieving 100% at 10 months even though it was above 90% since the 8th month.
The three patients in which the disappearance of the sores was prolonged beyond 6 months (8, 9 and 10 months) were followed during 6 additional months and they remained without recurrence. That means that their cure took longer, but once they achieved remission, it was permanent.
3.7 Remedies prescribed:
Following the methodology that we have pointed out to choose the constitutional medication, the remedies chosen were: (Table 4)
Table 4. Remedies prescribed
| Constitutional remedy(in order of frequency) | No. ofPatients |
| Lycopodium | 7 |
| Arsenicum album | 4 |
| Nux vomica | 4 |
| Natrum muriaticum | 3 |
| Sulphur | 3 |
| Staphysagria | 2 |
| Calcarea carbonica | 1 |
| Carcinosinum | 1 |
| Ignatia | 1 |
| Mercurius solubililis | 1 |
| Phosphorus | 1 |
| Pulsatilla | 1 |
| Sepia | 1 |
Eight patients required a second homeopathic medication (that is why the sum was 30 patients, 13 remedies) since aphthae diminished without disappearing in a permanent way, and this was achieved with the second medication. The potency used most often was 200 CH.
From the beginning of the treatment, even with patients whose sores continued, these began to space out in their appearance, to be smaller and with lighter symptoms. Patients described this amelioration repeatedly with the statement : “Never like before.”
3.8 Miasmatic study.
Another important principle of Homeopathy is that of miasms. As complementary study, for their importance, we decided to include in this work the miasmatic results of the study.
A miasm is defined as the constitutional, inherited chronic morbid state that predisposes a person to suffer in a certain way. Basically it is the background we bring when born, ie., our inheritance.
3 well defined miasmas exist (99-101).
- Miasm 1: Psora when symptoms denote defect or hypofunction
- Miasm 2: Sycosis where symptoms express excess or hyperfunction
- Miasm 3: Syphilis whose symptoms suggest perversion or dysfunction
People are basically tri-miasmatic, but one or two of the three are always predominant. The consensus is that to treat a chronic disease, the homoeopath should take into account the so-called active miasms in the patient.
3.8.1 Predominant miasm
A general miasmatic analysis was made and the predominant miasm (102-104) was identified in:
- Family pathological antecedents because, since miasm is inherited, it is important to know the family miasmatic background that we may manifest when born. So, we have classified the diseases suffered by each relative as it expressed lack (psora), excess (sycosis) or distortion or perversion (syphilis) which indicated at the end, the predominant miasm, the one found most often.
The syphilitic pathologies prevailed greatly, being found in 80% of the family antecedents of the patients: neoplasias of several organs or viscera, heart attack, peptic ulcer, ictus, syphilis, schizophrenia, glaucoma, suicide. Then sycosis: arterial hypertension, allergy, tuberculosis, polyps, lithiasis, hepatitis, pancreatitis, bronchitis, prostatic enlargement. Later on psora: asthma, parasitism, diabetes.
- Personal pathological antecedents. We proceeded in similar form as in 3.8.1.1 because this defines our miasmatic tendency to fall ill.
In personal pathological antecedents sycosis prevailed: arterial hypertension, renal infections, tonsillitis, appendicitis, arthrosis, pneumonia, pneumonia, uterine fibroma, polyps. They followed the syphilític and psoric diseases in the same proportion: Syphilis: neoplasias, ischemic cardiopathies, glaucoma, anal fissure, congenital anomalies. Psora: Giardiasis, colds, diabetes, asthmas, hyperthyroidism.
- Present day symptoms. Besides aphthosis, that is a syphilitic sign, we found that in 18 patients sycosis prevailed, in 2 psora and in 4 equally psora-sycosis. Sycosic symptoms: showing desires for specific foods or drinks, palpitations, restless sleep, changing mood, particular fears, susceptibilities, sensitivities, behaving as in a hurry, anticipatory anxiety, emotionally explosive, dogmatic, capricious, demanding, perfectionist, irritable, optimistic or full of cares. Psoric symptoms: thinness, chilly, insomnia, irritable, weeping easily, sympathetic, anxious, loneliness, introspection, sadness, full of cares, perfectionistic and having fixed thoughts. Syphilitic symptoms: heartburn, water-brash, capricious.
Note: Some symptoms are shared by two miasmas (105).
There were 3 patients in whom remission was not achieved until after 9 months of treatment, possibly because the first remedy administered was not the most appropriate or from a miasmatic taint that blocked the cure. However, once these aspects were addressed, remission of the disease was permanent.
3.8.1.3 Miasmatic sequence of homeopathic remedies prescribed. Medications can also be classified miasmatically. The miasmatic sequence of remedies prescribed was (Table 5):
Notes:
- a) 1 = Psora 2 = Sycosis 3 = Syphilis
- b) Equilateral trimiasmatic: No miasm prevail: the 3 miasms are in equal proportion.
Table 5. Homeopathic remedies use ant its miasmatic sequence.
| ConstitutionalRemedy (in order of frequency) | Miasmatic sequence (106-110) |
| Lycopodium | Equilateral trimiasmatic |
| Arsenicum album | 3-1-2 |
| Nux vomica | 2-1-3 |
| Natrum muriaticum | Equilateral trimiasmatic |
| Sulphur | Equilateral trimiasmatic |
| Staphysagria | 3-1-2 |
| Calcarea carbonica | 1-3-2 |
| Carcinosinum | 3-1-2 |
| Ignatia | 2-1-3 |
| Mercurius solubilis | 3-1-2 |
| Phosphorus | 3-1-2 |
| Pulsatilla | 2-1-3 |
| Sepia | 3-1-2 |
Discussion
RAS is a destructive disease; it is syphilitic, homeopathically speaking, and as such it is clinically expressed.
We note that 80% of treated patients had an important syphilitic background in their family antecedents.
We have reviewed the national and international bibliography with respect to homeopathic treatment of aphthous stomatitis. Four research papers have published in our country.
Pena et al111 made a revision of the entity and they treated patients in acute stages with three homeopathic remedies and followed their evolution until the disappearance of the lesions. 98% of the lesions had disappeared by the 5º day of treatment.
Casanova et al112 used only the homeopathic remedy, Borax, also in patients in the acute stage, versus a group with conventional treatment. In the group treated with homeopathy, lesions were cured in half the time of the control patients using conventional treatment.
Del Puerto et al113 carried out a bibliographical revision of RAS, pointing out the homeopathic medications used most often, recommending the personal study of all patient´s symptoms, which is, in fact, what we have done in this paper: the individualization of the treatment.
Finally, Perez and Rodriguez114 made a revision of all types of treatments used in RAS, including homeopathy.
In the international bibliography found, they only make a general revision or they mention the homeopathic medications most often used in the treatment of RAS but without clinical cases 115-119
We only found a clinical trial carried out by Mousavi and Mojaver120 in which patients with Aphthous Stomatitis were treated with homeopathy, treating them individually (just as we did) but this author only treated the acute stage of the illness. Some other papers reported treatment of RAS with Levamisole with a 2 to 4 months follow-up, rarely 6 months. Results varied from very good67,69 to not significant between Levamisole versus placebo or even better results with placebo73. Hashemi Manesh, from Iran published in 2012 a meta analysis (his thesis paper) 121 using Levamisole vs Placebo. His conclusion was that Levamisole was better than placebo but without specifying time of follow-up of any of the 12 cases analysed.
We have not been able to find clinical trials similar to ours (RAS treatment with Homeopathy) in order to establish comparisons.
In our results it becomes evident that taking into account miasms was of decisive importance, as the syphilitic miasm was often present, dominating the family pathological antecedents. This same condition prevailed in the miasmatic sequence of remedies prescribed (there was a high predominance of the syphilitic miasm when they were not equilaterally trimiasmatic). This coexistence of preponderance of the same miasm under both conditions, in our opinion, favored the healing effect of the medication.
The fact that RAS ethiology is not defined brings about the multiplicity of elements used in its treatment throughout the world. Nevertheless, when we look for effective treatments to prevent long term relapses, we found a lack of papers in this respect, which tells us about the difficulty that exists in treating this disease successfully. That is, aphthosis, in its acute stage can be controlled with effectiveness by multiple medications or measures, but remission of RAS in a permanent way is very difficult, if not almost impossible, to reach. It is for this reason that this disease becomes a problem of health for patients, physicians or stomatologists who try to find a solution as permanent as possible for the condition.
Conclusions
We consider that homeopathic treatment individually, taking into account the miasmatic aspect in each patient, is the most suitable and effective, as we have verified in this paper. High remission percentages were reached from the second month of treatment. As a conclusion, we can say, as Hahnemann described in his masterpiece “Chronic Diseases Treatise” (99) – when we are going to treat chronic diseases, if we want to obtain a cure, we should bear in mind the miasmatic condition.
Acknowledgements: To Pilar Cardoso, Stomatology specialist for her cooperation by sending me patients with Aphthous Recurrent Stomatitis.
REFERENCES
- A. Ship. Recurrent aphthous stomatitis: an update. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 81 (2) (1996) 141-147
- W. Barrons. Treatment strategies for recurrent oral aphthous ulcers. Am J Health Syst Pharm 58 (2001) 41-50
- Eisen, D.P. Lynch. Selecting topical and systemic agents for recurrent aphthous stomatitis. Cutis 68 (2001) 201-206
- R. Kerr, J.A. Ship. Management strategies for HIV-associated aphthous stomatitis. Am J Clin Dermatol. 4 (2003) 669-680
- S. Natah, Y.T. Konttinen, N.S. Enattah, N. Ashammakhi, K.A. Sharkey, R. Häyrinen-Immonen. Recurrent aphthous ulcers today: a review of the growing knowledge. Int J Oral Maxillofac Surg 33 (2004) 221-234
- Shrivastava, W.J. Gareth. Treatment of Aphthous Stomatitis with Topical Alchemilla vulgaris in Glycerine. Clin Drug Invest. 26(10) (2006):567-573
- S. Rogers. Recurrent aphthous stomatitis: clinical characteristic and associated systemic disorders. Semin Cutan Med Surg. 16 (1997) 278-283.
- T. Dermacase. Recurrent aphthous stomatitis. Can Fam Physician 40 (444) (1994) 628.
- B. Zain. Oral recurrent aphthous ulcers/ stomatitis: prevalence in Malaysia and an epidemiological update. J Oral Sci 42 (2000)15-19.
- Wikipedia, the free encyclopedia. Available on line at: http://en.wikipedia.org/wiki/Aphthous_ulcer. January 2008.
- M. Chinea, H. de la Rosa, D.R.Morales . Etiology and pathogenicity of acute and chronic periodontal diseases. At: E.M. Chinea, M.E. González editors. Periodontal Compendium. La Habana, Cuba; 2006, pp. 165-166 (in Spanish)
- M. Chinea, M.E. González, editores. Diagnosis, prognosis and treatment of inflammatory periodontal acute disease. At: E.M. Chinea, M.E. González editors. Periodontal Compendium. La Habana, Cuba. 2006. pp. 187-191. (in spanish)
- Doncel, M. Martínez, A. López, Z.T. Ilizástigui . Epidemiological behaviour of Recurrent Aphthous Stomatitis in Military Medicine Superior Institute “Dr. Luis Díaz Soto” patients. Rev Cubana Med Milit 38 (in Spanish) Available on line at: . 2009
- Wray, M. Ferguson, W. Hutcheon, J. Dagg. “Nutritional deficiencies in recurrent aphthae”. J Oral Pathol 7 (1978) 418–423.
- Wray, T.P. Vlagopoulos, R.P. Siraganian. Food allergens and basophil histamine release in recurrent aphthous stomatitis. Oral Surg Oral Med Oral Pathol 54(1982)388-395
- Endre. Recurrent aphthous ulceration with zinc deficiency and cellular immune deficiency. Oral Surg Oral Med Oral Pathol 72(1991)559-561
- S. Henson, M. Sarmadi. Recurrent aphthous stomatitis. Quintessence Int 31(2000)95-112
- Herlofson, P. Barkvoll . Sodium lauryl sulfate and recurrent aphthous ulcers. A preliminary study. Acta Odontol Scand 52 (5) (1994) 257-259.
- Healy, M. Paterson, S. Joyston-Bechal, D. Williams, M. Thornhill. The effect of a sodium lauryl sulfate-free dentifrice on patients with recurrent oral ulceration. Oral Dis 5 (1) (1999) 39–43.
- Oda. Helicobacter pylori (HP) may be involved in the pathogenesis of recurrent aphthous ulcers in children and adolescents. J Evid Based Dent Pract. 5 (2005) 45-46.
- Mansour-Ghanaei, M. Asmar, A.H. Bagherzadeh, S. Ekbataninezhad. Helicobacter pylori infection in oral lesions of patients with recurrent aphthous stomatitis 11(2005)CR576-579. Epub 2005 Nov 24.
- Didem Arslan TaşTolga Yakar, Hakan Sakalli, Ender Serin. Impact of Helicobacter pylori on the clinical course of recurrent aphthous. Available on line at: stomatitishttp://onlinelibrary.wiley.com/journal/10.1111/(ISSN)1600-0714/earlyview
- N. Maksomovskaia, V.N. Tsarev, M.M. Davydona, V.M. Shishchenko. The clinico-inmunological characteristics of the course of recurrent aphthous stomatitis. Stomatologia (Mosk) 74(1995)16-19 (In russian with abstract in english)
- Vicente, A. Soria, A. Mosquera, J. Pérez, A. Lamus, Castellano T, et al. Inmuglobulin G. Subclass measurements in recurrent aphthous stomatitis. J Oral Pathol Med 25 (1996) 538-540.
- R. Bazrafshani, A.H. Hajeer, W.E. Olliex, M.H. Thornhill. IL-1B and IL-6 gene polymorphisms encode significant risk for the development of recurrent aphthous stomatitis (RAS). Gen Immunol 3 (2002) 302-305.
- J. Buno, J.C. Huff, W.L. Weslon, D.T. Cook, S.L. Brice. Elevated levels of interferon gamma, tumor necrosis factor alpha, interleukins 2,4 and 5 but not interleukin 10, are present in recurrent aphthous stomatitis. Arch Dermatol 134 (1998) 827-831
- Guranska, B. Urbaniak, P. Lewkowicz, H. Tchorzewski. Recurrent aphthous ulcers: the etiology with special reference to immunological theories. Pol Merkuriusz Lek 8(2000)113-117 (in polish)
- Sun, C.T. Chu, Y.C. Wu, J.H. Yuan. Mechanisms of depressed natural killer cell activity in recurrent aphthous ulcers. Clin Immunol Immunopathol 60 (1991) 83-92
- Femiano, A. Lanza, C. Buonaito, F. Gombos, M. Nunziata, S. Piccolo, N. Cirillo. Guidelines for diagnosis and management of aphthous stomatitis. Pediatr Infect Dis J. 26 (2007) 728-732
- A. Mitchell. Plant Medicine. Preparatory Manuscript; Seattle, WA; 2000.
- Tilgner. Herbal Medicine-From the Heart of the Earth. Wise Acres Press, Inc.; Creswell, OR; 1999.
- Andriani, T. Bugli, M. Aalders, S. Castelli, G. De Luigi, N. Lazzari, G.P. Rolli. The effectiveness and acceptance of a medical device for the treatment of aphthous stomatitis. Clinical observation in pediatric age. Minerva Pediatr 52 (2000) 15-20
- L. Ogletree, R.G. Rischer. Physician’s and Pharmacist’s Guide to the Top 10 Scientifically Proven Natural Products. Natural Source Digest; 2nd Ed. Brandon, MS; 1997.
- Chevallier. The Encyclopedia of Medicinal Plants. DK Publishing; New York, NY; 1996 pp. 55.
- T. Murray. The Healing Power of Herbs. 2nd Ed. Prima Publishing; Rocklin, CA, 1995.
- Ellingwood. American Materia Medica, Therapeutics and Pharmacognosy; Botanical Vol. II. Eclectic Medical Publications; Sandy, OR, 1994.
- W. Felter. The Eclectic Materia Medica, Pharmacology and Therapeutics, Botanical Vol. 1. Eclectic Medical Publications; Sandy, OR, 1994.
- Scalzo. Naturopathic Handbook of Herbal Formulas. 3rd Ed. Kivaki Press; Durango, CO, 1994.
- Ody. The Complete Medicinal Herbal. Dorling Kindersley; New York, NY, 1993.
- E. Stansbury. Botanical Medicines Acting on the Respiratory System. Preparatory Manuscript; Battleground, WA, 1992.
- E. Stansbury. Pharmacognosy for the Herbal Practitioner. Preparatory Manuscript; Battleground, WA, 1992.
- Thomas. 10 Essential Herbs. Hohm Press; Prescott, AZ, 1992.
- F. Weiss. Herbal Medicine. Beaconsfield Publishers LTD; Beaconsfield, England, 1991.
- Hoffman, The New Holistic Herbal. Element Inc; Rockport, MA, 1991.
- Mabey et al. The New Age Herbalist. Collier Books, Macmillan Publishing Company; Richard Mabey Editor. New York, NY, 1988. England, 1988.
- E. Tyler, L.R. Brady, J.E. Robbers. Pharmacognosy. 9th Ed. Lea & Febiger; Philadelphia, PA, USA. 1988 pp 65.
- C. Wren. Potter’s New Cyclopaedia of Botanical Drugs and Preparations. The C.W. Daniel Company Limited; Essex, 1988
- Beyer. The Master Book of Herbalism. Phoenix Publishing; Custer, WA, 1984.
- Amanlou, N. Babaee, M. Saheb-Jamee, A. Salehnia, H. Farsam, Z. Tohidast Akrad. Efficacy of Satureja khuzistanica extract and its essential oil preparations in the management of recurrent aphthous stomatitis. Daru 15 (2007) 231-235.
- Babaee, A. Mansourian, F. Momen-Heravi, A. Moghadamnia, J. Momen-Beitollahi. The efficacy of a paste containing Myrtus communis (Myrtle) in the management of recurrent aphthous stomatitis:a randomized controlled trial. Clinical Oral Investigations 14 (2010) 65-70.
- de Armas, Y. Sarracent, E. Marrero, O. Fernández, C. Branford-White. Efficacy of Rhizophora mangle aqueous bark extract (RMABE) in the treatment of aphthous ulcers: a pilot study. Current Medical Research and Opinion 21 (2005) 1711-1715.
- D. Martin, J. Sherman, P. van der Ven, J. Burgess . A controlled trial of a dissolving oral patch concerning glycyrrhiza (licorice) herbal extract for the treatment of aphthous ulcers. General Dentistry 56 (2008) 206-210.
- Motallebnejad, A. Moghadamnia, M. Talei. The efficacy of Hypericum perforatum extract on recurrent aphthous ulcers. Journal of Medical Sciences 8 (2008) 39-43.
- Bello, X.M. Calzadilla. Propolis effectivity in Apfthous Stomatitis treatment. Rev Cubana Estomatol. 44 (2007) ISSN 0034-7507.(In Spanish with English Abstract)
- W. Savage, M.J. Mc Cullough. Topical corticosteroids in dental practice. Aust Dent J. 50 (2005) S40-44.
- W.B. Binnie, F.A. Curro, A. Khandwala, R.G. Van Inwegen. Amlexanox oral paste: a novel treatment that accelerates the healing of aphthous ulcers. Compendium 18 (1997) 1116-1125
- Murray, N. McGuinness, P. Biagioni, P. Hyland, P.J. Lamey. A comparative study of the efficacy of Aphtheal in the management of recurrent minor aphthous ulceration. J Oral Pathol Med 34 (2005) 413-419.
- Ylikontiola, T. Sorsa, R. Hayrinen-Immonen, T. Salo T. Doxymycine-cyanoacrylate treatment of recurrent aphthous ulcers. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 83 (1997) 329-333
- Ross Kerr, C.A. Drexel, A.L. Spielman. The efficacy and safety of 50mg penicillin G potassium troches for recurrent aphthous ulcers. Oral Medicine 96 (2003) 685-694
- R. Alidaee, A. Taheri, P. Mansoori, S.Z. Ghodsi. Silver nitrate cautery in aphthous stomatitis: a randomized controlled trial. Brit J Dermatl 153 (2005) 521-525
- L. Brice. Clinical evaluation of the use of low-intensity ultrasound in the treatment of recurrent aphthous stomatitis. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 83 (1997) 14-20
- Nasrin Zand, Mohsen Fateh, Leila Ataie-Fashtami, Gholamreza Esmaeeli Djavid, Seyyed-Mostafa Fatemi, Afshan Shirkavand. Promoting Wound Healing in Minor Recurrent Aphthous Stomatitis by Non-Thermal, Non-Ablative CO2 Laser Therapy: A Pilot Study Photomedicine and Laser Surgery. Available on line at: http://online.liebertpub.com/doi/abs/10.1089/pho.2012.3301. Oct 2012
- K. Arikan, A. Birol, F. Tuncez , E. Erkek , C. Koc . A prospective randomized controlled trial to determine if cryotherapy can reduce the pain of patients with minor form of recurrent aphthous stomatitis. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 101 (2006) 1-5.
- Brocklehurst , M. Ticke, A.M. Glenny, M. Lewis, M.N. Pemberton, J. Taylor, P. Riley, J.M. Yates. Systemic interventions for recurrent aphthous stomatitis (mouth ulcers). Editorial Group: Cochrane Oral Health Group. Available on line at: . Aug 2012
- Koray, G. Ak, E. Kürklü, H. Tanyeri, F. Aydin, F.S. Oguz et al. The effect of beta-glucan on recurrent aphthous stomatitis. Journal of Alternative and Complementary Medicine 15 (2009) 111-112.
- A. de Abreu, C.H. Hirata, D.R. Pimentel, L.L. Weckx. Treatment of recurrent aphthous stomatitis with clofazimine. Oral Surgery, Oral Medicine, Oral Pathology, Oral Radiology, and Endodontics 108 (2009) 714-721.
- de Cree, H. Verhaegen, W. de Cock W, F. Verbruggen. A randomized double-blind trial of levamisole in the therapy of recurrent aphthous stomatitis. Oral Surgery, Oral Medicine, and Oral Pathology. 45 (1978) 378-384.
- J. Drinnan, S.L. Fischman. Randomized, double-blind study of levamisole in recurrent aphthous stomatitis. Journal of Oral Pathology 7 (1978) 414-417.
- D. Meyer, M. Degraeve, J. Clarysse J, F. de Loose, W. Peremans. Levamisole in aphthous stomatitis: evaluation of three regimens. British Medical Journal 1 (1977) 671-674.
- F. Miller, M.E. Silvert, L.L. Laster, P. Green, I.I. Ship. Effect of levamisole on the incidence and prevalence of recurrent aphthous stomatitis. A double-blind clinical trial. Journal of Oral Pathology 7 (1978) 387-392.
- A. Olson, S. Silverman Jr. Double-blind study of levamisole therapy in recurrent aphthous stomatitis. Journal of Oral Pathology 7 (1978) 393-399.
- Van de Heyning . Levamisole in the treatment of recurrent aphthous stomatitis. The Laryngoscope 88 (1978) 522-527.
- L. Weckx, C.H. Hirata, M.A. Abreu, V.C. Fillizolla, O.M. Silva. Levamisole does not prevent lesions of recurrent aphthous stomatitis: a double-blind placebo-controlled clinical trial. Revista da Associacao Medica Brasileira 55(2009) 132-138 (In Portuguese with English abstract)
- P. Zissis, A.J. Hatzioti, D. Antoniadis, A. Ninika, J.C. Hatziotis . Therapeutic evaluation of levamisole in recurrent aphthous stomatitis. Double-blind comparison of two dosage schedules of levamisole and placebo. Journal of Oral Medicine 38 (1983) 161-163.
- Femiano, C. Buonaiuto, F. Gombos, A. Lanza, N. Cirillo. Pilot study on recurrent aphthous stomatitis (RAS): a randomized placebo-controlled trial for the comparative therapeutic effects of systemic prednisone and systemic montelukast in subjects unresponsive to topical therapy. Oral Surgery, Oral Medicine, Oral Pathology, Oral Radiology, and Endodontics 109 (2010) 402-407.
- H. Thornhill, L. Baccaglini, E. Theaker, M.N. Pemberton. A randomized, double-blind, placebo-controlled trial of pentoxifylline for the treatment of recurrent aphthous stomatitis. Archives of Dermatology 143 (2007) 463-470.
- Femiano, F. Gombos, C. Scully. Recurrent aphthous stomatitis unresponsive to topical corticosteroids: a study of the comparative therapeutic effects of systemic prednisone and systemic sulodexide. International Journal of Dermatology 42 (2003) 394-397.
- Pourahmad, M. Rahiminejad, S. Fadaei, H. Kashafi. Effects of camel thorn distillate on recurrent oral aphthous lesions. Journal der Deutschen Dermatologischen Gesellschaft 8 (2010) 348-352. (In german with English abstract)
- Mousavi, Y.N. Mojaver, M. Asadzadeh, M. Mirzazadeh. Homeopathic treatment of minor aphthous ulcer: a randomized, placebo-controlled clinical trial. Homeopathy 98 (2009) 137-141.
- Kolseth, B.B. Herlofson, A. Pedersen. Norwegian LongoVital and recurrent aphthous ulceration: a randomized, double-blind, placebo-controlled study. Oral Diseases 11 (2005) 374-378.
- Bratel, M. Hakeberg, M. Jontell. The effect of LongoVital on recurrent aphthous stomatitis in a controlled clinical trial. Oral Health & Preventive Dentistry 3(2005) 3-8.
- Samet, C. Laurent, S.M. Susarla, N. Samet-Rubinsteen N. The effect of bee propolis on recurrent aphthous stomatitis: a pilot study. Clinical Oral Investigations 11(2007) 143-147.
- M. Preshaw, P. Grainger, M.H. Bradshaw, .R. Mohammad, C.V. Powala, A. Nolan. Subantimicrobial dose doxycycline in the treatment of recurrent oral aphthous ulceration: a pilot study. Journal of Oral Pathology and Medicine 36 (2007) 236-240.
- A. Graykowski, A. Kingman. Double-blind trial of tetracycline in recurrent aphthous ulceration. Journal of Oral Pathology 7 (1978) 376-382.
- Volkov, I. Rudoy, T. Freud, G. Sardal, S. Naimer, R. Peleg et al. Effectiveness of vitamin B12 in treating recurrent aphthous stomatitis: a randomized, double-blind, placebo-controlled trial. Journal of the American Board of Family Medicine 22 (2009) 9-16.
- V. Lalla, L.E. Choquette, R.S. Feinn, H. Zawistowski, M.C. Latortue , E.T. Kelly et al. Multivitamin therapy for recurrent aphthous stomatitis: a randomized, double-masked, placebo-controlled trial. Journal of the American Dental Association 143 (2012) 370-376.
- Femiano, A. Lanza, C. Buonaito, F. Gombos, M. Nunziata, S. Piccolo, N. Cirillo. Guidelines for diagnosis and management of aphthous stomatitis. Pediatr Infect Dis J. 26(2007) :728-732
- A. Ramirez-Amador, L. Esquivel-Pedraza, S. Ponce-de-Leon, G. Reyes-Teran, M. Gonzalez-Guevara, S. Ponce-de-Leon, J.G. Sierra-Madero. Thalidomide as therapy for human immunodeficiency virus-related oral ulcers: a double-blind placebo-controlled clinical trial. Clin Infect Dis 28 (1999) 892-894
- Porter , C. Scully . Aphthous ulcers (recurrent). Clin Evid. 13 (2005) 1687-1694.
- Sin autores. Lactobacillus sporogenes. Altern Med Rev. 7(2002) 340-342.
- Oral ulcerative lesions. Available on line at: Agosto 2007
- Castillo, A. Pérez, M.V. Guntiñas. Uso del Inmunoferón en el tratamiento de la estomatitis aftosa en niños. Rev Cubana Estomatol 43(2006) .(In Spanish, with English abstract).
- V. Crouse, J.S. Reily . Aphthous Stomatitis. Copyright 1998 – 2007 (ISSN 1527-0661). Available on line at http://www.naturalopinion.com/nmp/nmp5/Apthstom.htm
- Hahnemann. “Versuch uber ein neues Prinzip zur Suffindung der Heilkräfte der Arzneisubstanzen” (Ensayo acerca de un nuevo Principio para descubrir las fuerzas curativas de las sustancias medicinales). Hufelands Journal. 1796 (In German)
- Jarasuriya. Clinical Homeopathy. B. Jain Publishers Ltd. New Delhi, India, 1988
- Hahnemann. Organon de la Medicina. 6ta. Edición. Parágrafo 6. Ed. de la Biblioteca. Caracas, 1983 (In Spanish).
- Quintero. Recurrent Aphthous Stomatitis. Homeopathic treatment miasmatic focused. In: I Congress of the Bioenergetic and Naturalist Cuban Society Havana, Cuba 2000. (In Spanish)
- Programa RADAR Anniversary CD 7.3 para Windows. Archibel S.A. Belgium.
- Hahnemann. Chronic Diseases Treatise. Firma Press. Asturias, Spain, 1991 (In Spanish)
- Sánchez Ortega. Notes about Hahnemann´s Miasms or Chronic Diseases. Mexicana Press, 1977 (In Spanish)
- Sánchez Ortega. Introduction to Homeopathic Medicine. Theory and Practice. Mexicana Press, 1997 (In spanish).
- Sánchez Ortega. Translation and Definition of mental symptoms of Barthel´s Synthetic Repertory. Mexican Homeopathy Medical College Ed., A.C. 1998 (In spanish)
- H. Allen. Chronic Miasms . Roy and Co. Bombay, India. Reedic.1960. (In Spanish)
- H. Grimmer. Miasms and Remedies. Homeopathic Heritage 20 (1995) 415
- T. Kent. New Remedies, Clinical cases, Lesser writings, Aphorisms and Precepts. Ehrhart and Karl Ed., Chicago 1926
- Ghatak. Chronic disease; its cause and cure, Translated by P.N. Banerjee. Printed in India, 1931
- Patel, P. Ramanlal. Chronic miasms in Homeopathy and their cure. Hahnemann Homeopathic Farmacy. Kottayam, 1996
- Laborde, G. Risch. Chronic Hereditary Diseases. Ed. Verlag Muller & Steinicke, München, 1998 (In German).
- Subramanian R. Miasms, their effects on human organism. New Delhi, 2001
- N. Currim. The collected works of Arthur Hill Grimmer. Ed. AN Currim. Conneticut, 1996
- R. Peña, Gómez MR, Barciela J, Vara A, Más M. Homeopathic treatment of Recurrent Aphthous Stomatitis in acute phase. Camaguey Medical Archives (Cuba) 11 (2006) ISSN 1025-0255. (In Spanish with English abstract)
- Casanova, A. Pavón, M. Santana, A. Cabrera. Effectiveness of homeopathy in the treatment of recurrent aphthous stomatitis. Available on line at (In spanish with English abstract) 2009
- M. Del Puerto, J.A. Pérez, J. Perdomo,E.M. Castro, L. Casas. Homeopathy and recurrent aphthous stomatitis.Bibliographic review Medical Electronic Review 33 (2011). (In spanish with English abstract)
- M. Pérez, A. Rodríguez. Recurrent Aphthous Stomatitis Treatment. . Medicentro 16 (2012). (In spanish with English abstract).
- Femiano , A. Lanza , C. Buonaiuto , F. Gombos , M. Nunziata , S. Piccolo , N. Cirillo. Guidelines for diagnosis and management of aphthous stomatitis. Pediatr Infect Dis J. 26(2007) 728-732
- V. Crouse, J.S. Reiley . Homeopathic remedies (References). All rights reserved (ISSN 1527-0661Copyright Akio Sato, CCN 2005
- A. Ship. Recurrent aphthous stomatitis: An update. Oral Surgery, Oral Medicine, Oral Pathology, Oral Radiology and Endodontology 81(1996) 141-147
- Deshpande. How to get rid of recurrent mouth ulcers? (Aphthous ulcers or stomatitis). Available on line at: http://drshreya.blogspot.com/2010/09/how-to-get-rid-of-recurrent-mouth.html. Sept 2010
- Vijnovsky. Homeopathic treatment of affections and acute diseases. Buenos Aires 1979 (In Spanish).
- Mousavi, Y.N. Mojaver. Homeopathic treatment of minor aphthous ulcer: a randomized, placebo-controlled clinical trial. Homeopathy (2009) 137-141
- Hashemi Manesh, Seyed Reza. The Therapeutic Effect of Levamisole on Recurrent Aphthous Stomatitis: A Structured Review and Metha-analysis Study. Available on line at 2011



Hi,
Excellent work. Thanks.
DEAR DR
YOU HAVE DONE A GREAT LABOUR IN FINDING CAUSES AND REMEDIES FOR RAS. I FEEL IT IS A SYPHILITIC MIASM BECAUSE IT IS CURED BY SYPHILITIC REMEDIES LIKE MERC, NITRIC ACID AND BORAX..BUT IT ARISES ONLY WHEN THERE THERE IS STOMACH DISORDER
THANKS
An extremely well done study. This high level of work benefits us all.
Thank you !
Glenda
Did patients continue to take the medication after remission?