the other song – International Academy of Advanced Homoeopathy
The success of Homoeopathy lies in practicing it beyond a science as an art. Though every art has its foundation in science but every science is explored in its fullest potential, only through its artistic expression. Every artist gets better and better with time and so does every practitioner who practices Homoeopathy as an art. The beginners just have to have to be patient and perseverant to master this artistic science.
Through this article, I have tried to address the issues that young homoeopaths face and have attempted to solve their difficulties faced in acute cases where there is paucity of symptoms, with the help of homoeopathic laws and concepts in comprehensive and easily reproducible ways.
As one begins the practice, he encounters many challenges. Often, patients just approach when their family physician is not available or when their friends and relatives recommend you for their treatment during acutes. Rarely, does the person approach us with the full understanding about Homoeopathy and its scope during the early days of practice. I shall be sharing 3 cases which came to me with acute illness, who had not already taken some other medication.
This is a case of my 28-year-old friend who is also a homoeopathic doctor and was 8 ½ months pregnant when I saw her first. She suddenly developed a severe headache one evening at around 5 p.m., without any apparent cause. Being aware of the side effects of allopathic treatment, she decided to resort to homoeopathic medicines. Since she was not practicing since a long time, she called me up at 8 p.m. with a hope that I could advise something to help with the headache. I had never received her case earlier, nor had any other homeopath, so there was no chance of knowing her constitutional remedy. Being a homeopath, she was prompt in detailing her symptoms especially the modalities.
She described her headache as severe frontal pain, which was worse movement and any kind of jar, like sneezing and was better by pressure. Her husband, alarmed by the suddenness and severity of the headache, checked her blood pressure which a bit higher, was contemplating to consult her gynaecologist for the same.
Repertorizing a few but clear symptoms that I had, I chose the following rubrics from the Phatak’s repertory:
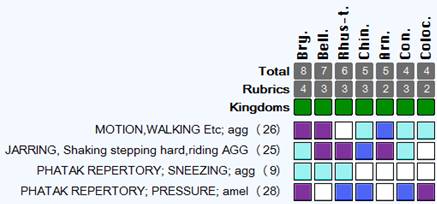
As per my advice, she took a dose of Bryonia 200 at 8.30pm. Within 1 hour I got a message from her that the pain was 30% better and within 2 hours she reported back saying that it was 50% better. Next day morning there was no pain at all. The concern that her family had if she had PIH (pregnancy induced hypertension) was settled. It has been 3 months since then and has delivered a healthy baby boy a couple of months back.
The second case that I would like to share is a case of my sister-in-law who had developed a severe backache of the lower lumbar region. Whilst, asking about the pain and the cause of the illness, it was found that she had suffered from gastroenteritis and had taken modern medicine to address it. Her main symptom during the whole episode was profuse diarrhea and the weakness following. After this episode, she developed the back pain. She could not narrate any other symptoms apart from the fact that the pain was severe and shooting I character. In this situation, I took the following rubrics –
PHATAK REPERTORY; DISCHARGES, Loss of vital fluid; agg (20)
PHATAK REPERTORY; PAIN, NEURALGIA, In general; shooting, darting, lightning,quick (39)

(MacRepertory 8.2.01, Professional, Kent Homoeopathic Associates)
Since the complaints started after loose motions I chose the rubric loss of vital fluids agg and the type of pain which was the only other symptom available and saw the probable remedies. Interestingly one of the remedies that shows up is Kali carb. From our knowledge of materia medica, we know that Kali carb is known for weakness and backache and sweating. In the M.M., we find the symptoms
- Great exhaustion
- SMALL OF BACK FEELS WEAK. Stiffness and paralytic feeling in back.
- Lumbago with sudden sharp pains extending up and down back and to thighs.
Based on these few symptoms, I prescribed Kali carb 200 bd for 2 days. To my surprise the pain disappeared in 2 doses and she was free from pain the very next morning. She also felt more energetic and active than she had done in a long time. This is what happens when we have to treat the relatives or close friends. They don’t wish to give you a detailed case. They seek help immediately without giving a complete case and then expect the result even faster. In such cases, you have to be really sure and have to confirm the few symptoms that are available. When these symptoms are understood correctly and repertorized precisely, they can yield good results especially after references from Materia medica.
The last case is that of a student who I used to tutor at the other song Academy. During our discussion in the tutorials she discussed a case which she was struggling with. This patient was having chronic cough and she had tried many possible remedies without much or great relief. On asking the modalities of the case she said that there was a very peculiar symptom. The cough would always get better after stools and it was worse at night and on waking. The other symptoms relating to cough were not very characteristic.
So I chose the following rubrics
- PHATAK REPERTORY; DISCHARGES, Loss of vital fluid; amel (29)
- PHATAK REPERTORY; TIME AGG AND AMEL; night; agg (49)
- PHATAK REPERTORY; AWAKENING; after agg (29)
We get the following suggestions –
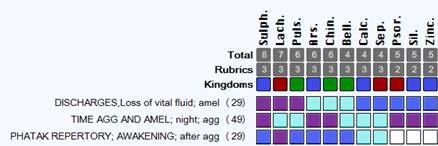
(MacRepertory 8.2.01, Professional, Kent Homoeopathic Associates)
Based on these suggestions, I asked the student to me the 2-3 most peculiar symptoms of the patient with respect to his state of mind. To my joy, she said he was highly loquacious and highly suspicious. This was enough for me to confirm Lachesis. He got just one dose of Lachesis 200 and the chronic cough disappeared.
In all three cases I have used the wisdom of Boenninghausen, analyzing using his concept of grand generalization. The modalities, sensations or clinical findings in a case can be generalized. These symptoms can be taken as general rather than local. These modalities or sensations can be successfully transferred to other locations as well. For example, the first patient has pain in the forehead worse motion. Here one way is to take the rubric head pain forehead motion agg. However generalization means to not restrict this to the location of the head but to generalize it. That’s why I took the rubric motion agg or loss of vital fluids or discharges amel in the cases. So we generalize all the sensations and modalities and then using materia medica differentiate the suggested remedies.
This approach has been of a great help to me in especially in the following situations:
- Acute illnesses when the patient has never been under my treatment
- Acute exacerbation of a chronic condition when the patient is already under my treatment and the constitutional remedy is not indicated.
I thoroughly believe and practice classical Homoeopathy where we need to take a detailed case and perceive what is to be cured in each individual case as Hahnemann mentions in aphorism 3. However, in practice there will be situations where such idealistic methods of practicing might not be possible. How a homoeopath, especially a beginner, can take this challenge as an opportunity to heal and relieve the patient is what I have attempted to demonstrate using this concept of grand generalization. I have been dealing with such situations often and as per my statistics the results are very promising.
Repertorizing the Experience
Dr. Pratik Desai
This is a case of a middle aged woman who came with post operative lumbar pain for prolapsed intervertebral disc (PID) at L3-L4, L4-L5 levels since 5-6 years. She came to clinic donning a lumbar belt and walking very slowly. Due to the pain she could not walk for long distances and was easily tired as she was very weak and had to rest after even the least exertion. She was so weak that she could not even hold any object weighing more than 500 gm and even walking from one room to the other in her home drained her, compelling her to rest for half an hour each time. On asking her to describe the character of pain, she said that she felt stiffness in her back (patient indicated stiffness with closed fist).
Now this is very crucial stage of case taking process. If one gets satisfied with the answer, one may start searching for the rubric stiffness in back and may end up with the understanding that this is the sensation of Anacardiaceae or the Rhus tox family which is typically stiff, tight and restricted. This is the wrong approach on our part, to jump to conclusions right at the start, where the picture is not yet clear and we start judging. In order to avoid any prejudice, I asked her to describe this stiffness, to which after taking a pause for 2-3 minutes, she said, “Doctor you know I feel that piece of wood is there in my back (she moved her palm towards the back)”. I said “Describe this piece of wood a little more?” She replied, “You know I feel that it will break if I make a movement, so I have to walk slowly.” I then asked her, “What do you mean that it will break?” She said “because it is brittle and porous.” So I asked her more about brittle and porous to which she replied that it felt like if you press a little bit it breaks, just like a saucer how it breaks when if falls from a hand.
Here we get the exact description of her stiffness which was like a piece of wood, brittle, porous and easily breakable. So she describes entirely different qualities of stiffness at the experience or sensation level. This is what we need to look into this description, which is more peculiar and an individual expression. This is what we need to look for in the repertory.
When we look in the repertory, delusion, she is made of wood and delusion, brittle she is, we get only the remedy Thuja, which belongs to the plant family conifers, which has the vital sensation of being soft and delicate and brittle, breaks easily.
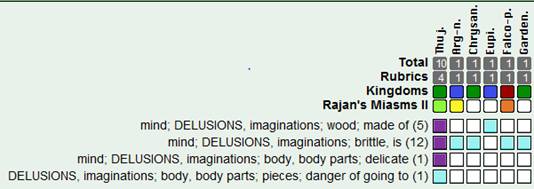
(Complete Repertory, Roger van Zandvoort, MacRepertory 8.2.01, Professional, Kent Homoeopathic Associates)
The remedy given was Thuja 200 followed by 1M later on (after 3 Months). Within a month, her pain had reduced by 60% and she was able to walk freely and she put on her lumbosacral belt only when she went out of her home. Her weakness had reduced too and she was more active. After 6 months, she reported that she was feeling great and that she was able to walk daily for 2 kms. Her energy levels were remarkably better and the fear of falling and getting hurt had disappeared. In her words, “Doctor, I am so strong now that I can face anything.”
The characteristic or peculiar symptoms of a remedy are nothing but the very sensation felt or experienced by the provers during provings and that were noted exactly by our masters. Our job as homoeopaths is to match the peculiar and characteristic symptoms of the patient with the characteristics of the remedy. So such peculiar symptoms are nothing but the vital sensation or experience of the substance from which they derived.
Here, I will give you another case example, of a 27-year-old male patient, who complained of alternating, severe pain in hip joints pain due to arthritis which started 2 months after he fell off a bike, around 2 years ago. Over the past 6-7 months, his pain was getting worse each day both in terms of intensity and duration, and each episode of pain now lasted for around 6-7 days.
The pain was worse at night, winter or cold weather and rising from sitting position. He described the pain as very intense and unbearable, as if someone was beating him or had punched him very hard, like it was bruised. It was very difficult for him to even turn in the bed or while changing the position. Even stooping is difficult and if he has to pick something from the floor, it takes half an hour. The pain is worse when he stretches his leg; it feels as if someone was dragging and pulling at his leg, as if his legs would detach themselves from the hip joints.
On asking further about the exact experience of the pain, he said that he felt as if something was twisting or turning inside the hip clock-wise or anti-clock wise. When asked further to describe the experience of twisting and turning, he said that he felt as if something was squeezing and twisting his leg from one side clock wise and anti-clock wise to the other, and it exerted such pressure that it felt as if the hip joints would break from the attachment, just like how you twist and squeeze a wet cloth to remove the stains. (showed with hand movement).
Now having such an exact detailed experience in the patient’s words, we need to search the exact expression in the repertory. When we do that, we get the following chart.
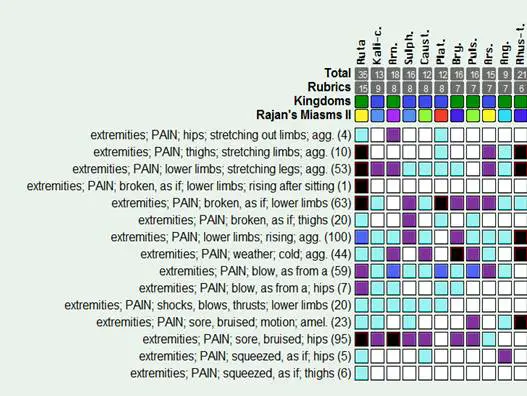
(Complete Repertory, copyright @Roger van Zandvoort, MacRepertory 8.2.01, Professional, Kent Homoeopathic Associates)
All the characteristic symptoms are covered by the single remedy Ruta g which belongs to the plant family Rutaceae, where according to the Sensation approach the experience is: squeezed and then broken/ crushed, squeezed and compressed, twisted and break/crush. The passive reaction is weakness or drained and the active reaction is stretching, desire, but it either aggr or amel.
The patient had received Ruta graveolens 200 a single dose. He was much better in a month’s time and the pain had disappeared 2 days after starting the remedy to never come up again. He was able to do all his work quite well. He was sleeping well and he also reported being more confident when meeting senior managers like he did earlier.
Here, we see that exploration of the exact experience or sensation of the disease or the sickness helps us reach the simillimum, by charting it out and seeing the possible rubrics that cover the sensation. The efforts should always be at trying to chart out the closest rubrics, and not merely the ones that describe the overall / state or the feelings. This exercise surely goes a long way in finding the right remedy which relieves greatly. My colleague Dr. Rishi Vyas, has given a few helpful pointers in the next section about how to effectively convert the expressions of a patient into the most appropriate rubrics.
Conversion of Patient Expression into Rubrics
- Rishi Vyas
Most of the time when we are done with the case, we start searching for symptoms; now-a-days the symptoms are replaced by rubrics. We just start typing the words in the search engine and look for rubrics. Let us really understand what a rubric means.
What is a rubric?
The word rubric has originated from the Latin word “Rubrica” which means
- Heading or Guiding rule, a title,
- A part of a manuscript or book, such as a title, heading, or initial letter, that appears in decorative red lettering or is otherwise distinguished from the rest of the text.
- A title or heading of a statute or chapter in a code of law.
So Rubric is a term applied to each Heading or main heading of symptoms with a list of a larger number of medicines, and many rubrics have under them smaller sub rubrics.
So rubric is basically a Keyword, which you search for. You will not find the exact words of a prover in the repertory but you have to search for the closest meaning as there is a difference between the prover’s language and repertorial language. This is often why we experience difficulty in finding the rubric for a symptom. This becomes much easier in repertories which are directly based on prover’s expressions, as in the case of philosophy based repertories.
Let us understand through examples:
A young patient in his mid 20’s came with the main complaint of pain in the head and stomach. Describing his stomach pain he said that there was a lot of burning in the abdomen and he could not bear it. Further describing it, he said, “It is as if some object is revolving in the stomach, as if something will come out just now. It is like a heavy thing inside, with great heat. Feels burnt inside, like a ball of fire is there inside and it is rotating within. It is very heavy, burning, and rotating inside and wants to come out.”
We see here there are a few elements to describe the pain – namely – pain, burning, ball, heavy, fire, stomach, abdomen. On using the repertory for a search of the closest symptoms, we come up with:
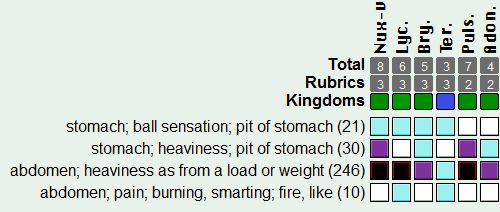
(MacRepertory 8.2.01, Professional, Kent Homoeopathic Associates)
On looking at this chart, we know that we have just gathered the elements to select the closest rubrics. Still they hardly match the exact expression of the patient’s symptoms, with little similarity between the two. The key here when we want to have a more precise description of the symptoms reflecting in the repertorization is to look for them in repertories which cover the specific kinds of expressions. For example, in this case we can use “Sensation as if – By Herbert Roberts”. This repertory gives you a detailed description of the provers’ symptoms and is very a good repertory to look for physical sensation. So on searching the elements from the above case in this repertory, we have
In Stomach:

In Abdomen

Another element you should also look for is “fire”
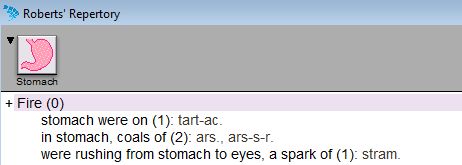
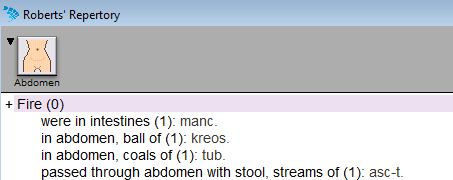
So the closest we get is:

(MacRepertory 8.2.01, Professional, Kent Homoeopathic Associates)
In other repertories, you may get rubrics – like pain burning like fire, or ball-like sensation in stomach / abdomen, but you will not be able to find the rubric which represents, ball which is like fire. For this you have to use ‘H. Roberts – Sensation as if’.
From the above examples we conclude that while converting the symptom into the rubrics, first it is necessary to chart out the elements of the symptom, the key words and then search for those, always looking to find which comes the closest. For this you shouldn’t only limit your search to your usual repertories, but extend it to other repertories. Each and every repertory has its own benefits and limitations. We need to be open, inquisitive and enquiring till we get the right expression. The patient was given Kreosote and he was greatly relieved in a month’s time.
Another, example is of a patient who came with the main complaint of imbalance, and sensation that he will fall. He described his complaint in a very peculiar way; he said, “Whenever I am looking down I feel as if I will fall on my back.” Now this is a very strange expression and I was wondering how to go about it. I started by tracing the basic elements of this symptom – fall, looking down, backwards.
If we are now to look in the repertory, we have the following options:
- Generalities; falling; sensation (102)
Or the other option is that you look n the chapter – Vertigo
- Vertigo; Fall Tendency.
- Vertigo; fall, tendency to; backward (56)
But if we are to cover the important modality of looking down, the only representation is under stooping agg. So I selected this rubric
(MacRepertory 8.2.01, Professional, Kent Homoeopathic Associates)
The remedy that helped him was Causticum. Here – we need to see what are other synonyms are used in repertory, like looking down – can be searched as stooping – which is nothing but bend one’s head or body forwards and downwards.
Another patient describes her situation where is she is depressed, and feels very low, doesn’t want to talk to anybody. She said “ I am in a state of depression and I just want to sit in my room, be with myself, do nothing and just keep quiet.” Converting her verbatim into elements, I got sadness, sit, quiet, talk does not want.
Here, we can either search for:
- Mind; quiet; wants to be (195)
- Mind; aversion; everything, to (74)
- Mind; indifference, apathy; everything, to (199)
- Mind; sit, sitting; desires to (200)
- Mind; sit, sitting; desires to; still, silent (78)
- Mind; taciturn, indisposed to talk (460)
But wouldn’t it be great if we were to find all the elements being covered under the same rubric which is very close to the totality which she describes: sit, taciturnity, sadness. So, we also have a symptom under the mind section, which goes as follows:
- Mind; sit, sitting; desires to; wrapped in deep, sad thoughts, as if, and notices nothing (43)
(MacRepertory 8.2.01, Professional, Kent Homoeopathic Associates)
The remedy selected using this rubric, and with other references from the materia helped her tremendously.
Another case example is of a child, who once had a strong urge for urination, but she couldn’t speak out and controlled it for a long time. Since that day she has problems with urination; she cannot control her urine and she often passes it involuntarily. The elements here would be: involuntary, urination, holding.
Now here, if we are to understand exactly, we see a cause-effect relationship. The rubric or rubrics, which cover both of them, will only be able to define the totality closest:
For this, we have options like:
- Bladder; involuntary urination; children, in (46)
- Bladder; urging to urinate, morbid desire; children, in (5)
- Generalities; urination; holding, retaining, on (18): this expression gives you a general affection of urine holding
So what we see is involuntary urine, after holding urine for long. So what happened is, the bladder was full and urine was held for a long time, following which there was no control. So in clinical terms this condition is a paralysis. So the other element is paralysis. Now, with this understanding, if you hunt for a closer rubric you get in Kent’s repertory:
- Bladder; PARALYSIS; over-distension, after (10)
- Bladder; PARALYSIS; forcible retention seems to paralyze the bladder. (8)
Complete Repertory 2015:
- Bladder; paralysis; distension, after (12)
Another interesting example, on observation during the case, if you see that whenever the patient is asked any question he looks straight at a point as if dazed for some time and then answers.
Elements: answer, looking dazed. The other aspect here is to observe the manner in which the patient has answered the question – it is slow
So we have the rubrics:
KENT Repertory:
- Mind; ANSWERS; reflects long (8)
- Mind; ANSWERS; slowly (23)
Complete repertory 2015
- Mind; reflecting; long (22)
- Mind; answer, answering, answers; slowly (46)
This symptom is purely from observation – so how the patient speaks, when he speaks, and what he says is very important – the tone, the intensity the pace all are very important.
First and of foremost in importance is to digest and to understand the symptom in its entirety and what the patient means to convey and then to break it into elements, as that is how the symptoms are represented in the repertories. The key however, lies in searching for those rubrics which have most elements covered and which represent the totality most closely, rather than ones which represent the totality in fragments. After doing this, confirm whether the rubric chosen is actually representing the symptom in its totality. This is the entire process. Most of the time we skip the process and focus directly on searching the rubric and cross reference without even understanding what the symptom is. These cases may be misleading in the selection of similar rubrics. It is important to understand the symptom in its completeness and form a firm base, before we start hunting for rubrics.
the other song is organizing the Repertory series ‘Mastering the Repertory’ which will cover a range of topics including the use of repertory and practical application of repertory demonstrated through cases. The lecture series will also involve case exercises, video lectures and webinars to thoroughly train the students in skillful repertorial application.
A small glimpse into the content of the course:
- Different chapters of Kent’s repertory
- How to study mind rubrics
- Finding exact symptom in repertory
- Single drug rubric
- Finding the expression of the patient
- Use of Repertory in pathological cases
- Use of Repertory with Kingdoms and Miasms
The faculty of the other song including Dr. Rajan Sankaran, Dr. Jayesh Shah and Dr. Sujit Chatterjee will talk on various topics to provide deeper insights into the subject in weekly lectures over the year.
About the other song International Academy of Advanced Homoeopathy
‘the other song’ is a world class premium medical centre which puts good health and well being at the core of an academic culture dedicated to complete patient care. Situated in Mumbai, this institute is one in its kind where a team of 35 doctors headed by Dr. Rajan Sankaran (the pioneer of the Sensation Approach in Homoeopathy) come together and practice Homoeopathy. At the Academy, the students and practitioners are trained in advanced Homoeopathic practices, using new methodologies in combination with the traditional approaches, all with the use of state-of-the-art technologies. The Academy is also a meeting point for different schools of thought in Homoeopathy, where renowned homoeopaths – national and international are invited, to share their knowledge and experience, so that there is a constant flow of ideas on a common platform.
Dr. Devang Shah
Dr. Devang Shah, M.D. (Hom) is an In-house Consultant and Faculty member at “the other song – International Academy of Advanced Homoeopathy”. As a Faculty member at the other song, he has been imparting knowledge on Sensation Approach and Synergy to students all over the country. He attributes his knowledge to the reputed teachers and masters in current homoeopathic scenario – Dr. Sankaran, Dr. Jayesh Shah, Dr. Sujit Chatterjee, Dr. Mahesh Gandhi and Dr. Dinesh Chauhan. Dr. Devang is known for his lectures on case-taking where he walks the students step-by-step into the very experience of the patient. Empathy to the patient and his suffering, with a passion for healing has rendered him popular among his patients. He is also a visiting consultant at BAPS Hospital, Ahmedabad where he consults with Dr. Sujit Chatterjee, providing expert opinion on complex pathological cases, many of them being cancer. Besides, he is a regular contributor of his successful cases in international journals like HPathy, Homeopathic Links, Homeopathic Heritage and Interhomeopathy.
Dr. Pratik Desai
Dr. Pratik Desai, D.H.M.S., C.C.A.H. is an in-house consultant and faculty at ‘the other song’ Clinic. He is responsible for developing a Homoepathic OPD at Lion’s Tarachand Bapa hospital, Sion. His keen interest in teaching has led him to be a co-ordinator and mentor for the Batras group of doctors. His love for homeopathy propelled him to contribute to the literature by conducting provings of remedies such as Dysprosium metallicum and Carbon Dioxide. He is appointed as a mentor for university courses conducted by MUHS at the other song. He is the master mind behind creation of the homeopathic database software for the other song. He has been sharing his clinical experience and successful cases in various Homoepathic journals such as Heritage, Interhomeopathy, Links, NJH and many others. Before his association with the other song, he was a renowned lecturer in the department of Materia Medica at Ahmedabad Homeopathic Medical college.
Dr. Rishi Vyas
Dr. Rishi Vyas, M.D. (Hom) is an In-house Consultant and Faculty member at the ‘the other song’ clinic. He has worked with Dr. Rajan Sankaran in his charitable OPD, in Mumbadevi Homeopathic Hospital and at the other song. Besides, he has also learnt from prominent homoeopaths and teachers like Dr. Sujit Chatterjee, Dr. Jayesh Shah, Dr. Mahesh Gandhi and Dr. Kamlesh Mehta. He was also the member of WWR I team (Wednesdays with Rajan I – an online homoeopathic training program). He is known for his dedication, hard work, sensitivity and personalized care to each and every case. He is an efficient clinician and an experienced team leader. His thirst for knowledge led him to ardently pursue various schools of thoughts and approaches in Homoeopathy, being able to integrate them effortlessly. His unique style of teaching and application of repertory to case analysis have been widely appreciated. His lectures on Sensation and Synergy and Repertory have been well received as well. His cases have published in various peer reviewed journals like Homoeopathic heritage, National journal of Homoeopathy, and online magazine like H-pathy & Interhomeopathy.