The usual personality is an expression of the spirit, and though it can become imbalanced as part of illness, and this can be a guide to treatment, we cannot expect that we can change personality through homeopathic prescribing.
Introduction
 On first learning homeopathy it seems intuitively right when one is presented with the idea that the psychological aspect of the patient is affected by disease just as much as is the physical body. One can’t help but agree especially when we have all had the experience of being sick ourselves. We know how much we are affected by illness at all levels.
On first learning homeopathy it seems intuitively right when one is presented with the idea that the psychological aspect of the patient is affected by disease just as much as is the physical body. One can’t help but agree especially when we have all had the experience of being sick ourselves. We know how much we are affected by illness at all levels.
Soon, however, the situation becomes more murky. What do we mean by mental or emotional symptoms when considering them from a homeopathic perspective? From our experience in this culture, we come to think of mental and emotional illness as something different than other kinds of diseases like infectious illness, chronic degenerative disease, etc. These psychological signs become the province of a different sort of doctor – one who talks to us or gives us “brain chemicals” to correct a functional imbalance.
Even when we begin to think homeopathically we run up against the thinking we absorbed as children and, almost without decision, we tend to put symptoms that are behavioral into a different category. Thus it is an obstacle to us in understanding the same perspective that Hahnemann had.
The purpose of this paper is to explore this topic in more detail – at first, from the perspective of Hahnemann – to try to see what he was thinking when he discussed this type of illness in his writings. Given this foundation, I would like to then add to it what has been learned about the brain and its functions since that time. I hope we can come to a better understanding of how to use this information in our cases.
Hahnemann’s Ideas
The topic of mental and emotional disease is discussed in paragraphs 210 to 230 of the Organon. It is very interesting that Hahnemann starts the discussion by bringing back an idea previously discussed in paragraph 176 – that is the concept of “one-sided” disease. He defines this as being a situation in which “all the rest of the disease symptoms vanish, as it were, before a great, prominent symptom”. He then tells us that the “so-called” (his quotes) mental and emotional diseases are of this kind.
This is an extraordinary perspective is it not? Hahnemann is telling us that illness of this type is not fundamentally different than other types of disease except in its way of manifesting. That is, it tends to gather under a prominent symptom with the rest of the pattern becoming less noticeable.
Here is the sequence of ideas that are discussed by Hahnemann in reference to understanding these symptoms:
- Almost all of the one-sided diseases are outcomes of the psoric miasm.
- Mental and emotional diseases are included in this same category of one-sided or defective diseases.
- They are not fundamentally different from other illnesses affecting the body, as the frame of mind is always altered to some degree in illness.
- The emotional state of the patient often decides the remedy when considering a differential. It is a peculiar symptom.
- These mental and emotional changes are always seen in provings as well as in illness.
- These symptoms seen in provings are unique expressions of each medicine, that is, each medicine expresses individuality.
- This class of diseases are to be treated in the same way as any other (physically) oriented disease, e.g., on the basis of similarity.
- To prescribe for these cases, one must go into the history of prior symptoms looking for physical signs that existed before and also for confirmatory signs that are subtle at the present time but which can be seen once knowing what is in the history.
So here we already have a context in which to consider this type of case. The condition is not really different than any other type of illness, for example, a diarrhea or stomach upset. What is unique is that it becomes focused under one major symptom and, further, that this is typical of the expression of psora.
Relation between somatic and psychic illness
We then come to a very interesting discussion in the Organon.
It is now stated that almost all those diseases that we label “mental or emotional” are physical diseases in the beginning, when they start. They go through a process in which the physical symptoms diminish (slowly or rapidly, depending on the case) while the psychological changes become the prominent symptoms, even the only ones, that remain.
Hahnemann refers to it like this: “finally the disease transfers itself (almost like a local malady) to the invisibly subtle mental and emotional organs.”
There are two things I would like to emphasize in this statement. One is the idea of localization, the other the idea of mental and emotional organs.
Localization
An important concept in the Organon is this idea of the localization of lesions. It is something that the life force does in response to the presence of an inimical influence – a miasm, an infectious disease, etc. It will help us to understand that this tendency to localization is not something that occurs only when there is illness. It is a normal process in the formation of an organism. If we think how the single cell develops into a complex and differentiated adult, we can see how the different functions seen in the mature individual have become localized into particular organs and tissues.
When there is a mental and emotional illness then this same localization happens but it occurs in the organs that determine behavior instead of organs having to do with other functions. For example, if a disease localized in the stomach then we would have digestive trouble, if in the bladder then symptoms having to do with urination. Here we have localization in those parts having to do with behavioral functions.
Organs of behavior
This brings us to the latter part of Hahnemann’s statement, “the invisibly subtle mental and emotional organs.” There are different ways one could understand this. One could think that he means something psychical, e.g., not physical. However, a more accurate way I think is to link this with localization and ask ourselves what these mental and emotional organs would be.
The simplest interpretation is to assume this refers to the central nervous system. This is indeed the place that corresponds to this functioning. It is not to say that this is a complete explanation, but certainly it is the physical structure through which these functions operate.
Let’s take for example the very common symptom, especially in cats, of losing appetite. The great majority of cats that I deal with have this symptom to some degree.
Where is the control of appetite located? Research in physiology shows us that the appetite center in located in the hypothalamus. According to a standard physiology text “stimulation of the ventromedial nuclei of the hypothalamus causes complete satiety, and, even in the presence of highly appetizing food, the animal will still refuse to eat. Conversely, destructive lesions of the two respective areas cause results exactly opposite to those caused by stimulation. That is, ventromedial lesions cause voracious and continued eating until the animal becomes extremely obese, sometimes as large as 4 times normal size. And lesions of the lateral hypothalamic nuclei cause complete lack of desire for food and progressive inanition of the animal.”
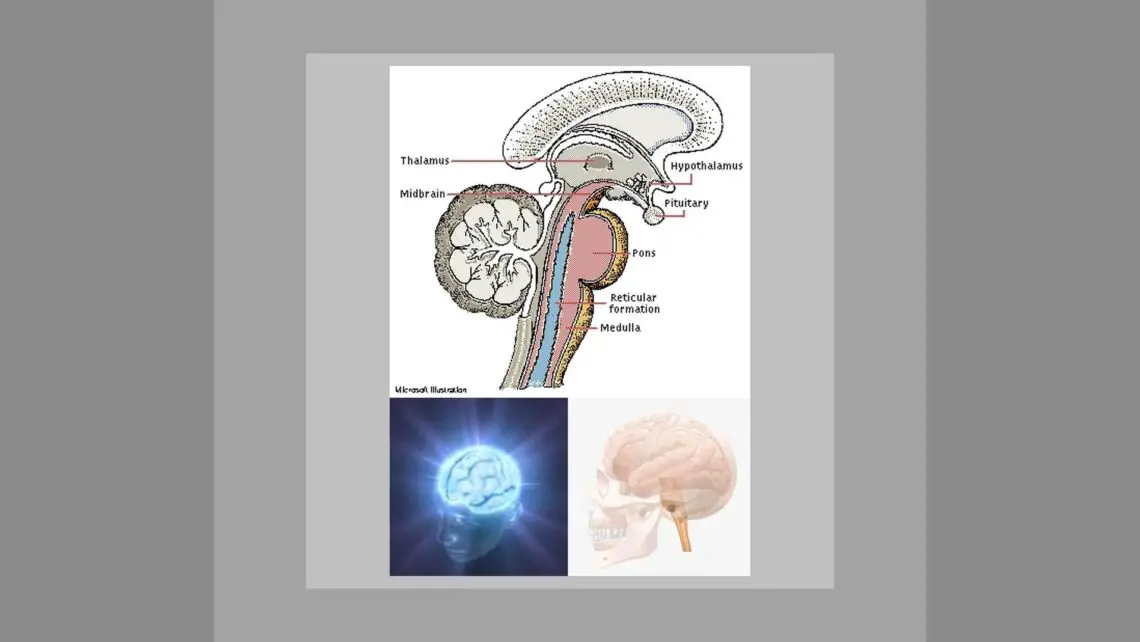
Let’s look at what part of the brain we are considering.
Brain Stem Location 1
This shows the older areas of the nervous system, older in the sense of existing the longest in animals. Note that part that is like a stalk which sits upon the upper spinal cord and below the cerebrum. The large cerebrum is later in development and seen most readily in primates and human beings. The area we are concerned with can more readily be seen in the next picture:
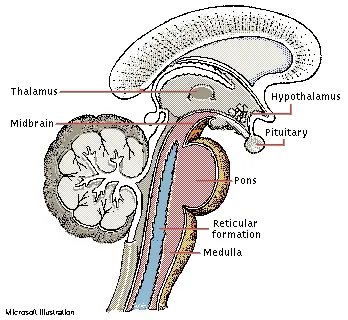
Brain Stem in Cross Section 1
This image is reversed, right to left, compared to the one above. The top curved part is where the cerebrum would come from if it were not cut away to view the underlying structure. The big bump on the left middle is the cerebellum which functions primarily with balance and to coordinate body movements.
The thalamus consists of two rounded masses of gray tissue lying within the middle of the brain, between the two cerebral hemispheres. The thalamus is the main relay station for incoming sensory signals to the cerebral cortex and for outgoing motor signals from it. All sensory input to the brain, except that of the sense of smell, connects to individual nuclei of the thalamus.
The hypothalamus lies beneath the thalamus on the midline at the base of the brain. It regulates or is involved directly in the control of many of the body’s vital drives and activities, such as eating, drinking, temperature regulation, sleep, emotional behavior, and sexual activity. It also controls the function of internal body organs by means of the autonomic nervous system, interacts closely with the pituitary gland, and helps coordinate activities of the brain stem. The brain stem is evolutionarily the most primitive part of the brain and is responsible for sustaining the basic functions of life, such as breathing and blood pressure.
So this most common of symptoms, appetite disorder, is a disturbance of that part of the brain between the nervous system and the endocrine system. In a way we could say it is the first level of brain dysfunction – above that of the spinal cord.
What other symptoms might we see stemming from here? The hypothalamus has these other functions (besides control of appetite) which we can recognize are linked to clinical symptoms commonly seen:
- Regulation of heart rate, blood pressure
- Regulation of body temperature, shivering.
- Regulation of body water (thirst center).
- Feeding reflexes, such as licking the lips and swallowing.
- Pupillary dilation.
- Control of the secretion of thytrophin, adrenocortical, luteinizing, follicle-stimulating hormone, gonadotropic hormones, growth hormone and prolactin (causing lactation).
In many of my chronic cases I see symptoms related to these functions. Some animals have irregular heart rates or a pulse that is too rapid or too slow. It is not uncommon for an animal to have a strong temperature preference when ill, strongly seeking heat or cold places. Thirst can vary, many dogs losing their thirst while cats will become excessively thirsty. Licking the lips and swallowing is described for some cats, usually in terms of “gulping” behavior. The endocrine imbalances are many, ranging from lack of proper growth, to sexual behavior in neutered animals, to producing milk in spayed females and so on. Some cats will have a recurrent dilation of a pupil, often just one eye affected.
Experiments in which the hypothalamus has been stimulated in the lateral area has been observed to cause an “increase in the general level of activity of the animal, sometimes leading to overt rage and fighting”. This is not uncommon in cats often coupled with endocrine disorders such as hyperthyroidism.
Stimulation of the most medial portion of the medial hypothalamus “leads to fear and punishment reactions” that we see in cats that are perpetually “fraidy cats”.
Stimulation of the lateral portion of the medial hypothalamus will increase the sex drive, and thus precedes the influence of the gonads, e.g., will cause this behavior even in neutered animals.
Destruction of the lateral hypothalamus will decrease drinking and eating almost to zero, often leading to lethal starvation. This is associated with an extreme passivity of the animal with loss of most of the usual activities. Think of the cats that go into this pattern of loss of appetite, increasing inactivity and sleepiness as part of their illness.
Another very interesting part of the hypothalamus is what are called “reward and punishment centers”. These are areas that can be stimulated and cause the animal to be very pleased or satisfied or the opposite, to be terribly afraid, fearful, defensive, etc. This is the place from which can originate what is called a “rage pattern” with the animal (1) developing a defense posture, (2) extending its claws, (3) lifting its tail, (4) hissing, (5) spitting, (6) growling and (7) developing erection of the hair with wide-open eyes and dilated pupils. The slightest provocation causes an immediate savage attack. Do we recognize seeing this behavior in our patients? Other anatomically nearby areas will cause fear with the desire to run away and so on.
We see that the hypothalamus is a very important structure being the probable site of lesions leading to some of the common symptoms we encounter as veterinarians. However other areas of the brain, associated with the hypothalamus are equally important. For example, the amygdala, located in the temporal lobes of the cerebral cortex, has abundant direct connections with the hypothalamus. Lesions here can cause a variety of odd symptoms as in raising the head or bending the body involuntarily, or changes in urination and defecation behavior. It can lead to movements such as licking excessively or smelling things abnormally. There are many other changes effected by lesions here, too many to list in this presentation.
One other example, however, is the effect of removing the temporal lobes and the amygdala, both – what is called the Klüver-Bucy Syndrome. This results in the following behaviors:
- Excessive tendency to examine objects orally.
- Loss of fear.
- Decreased aggressiveness.
- Tameness.
- Changes in dietary habits, even to the extent that a herbivorous animal frequently becomes carnivorous.
- Sometimes psychic blindness.
- Often excessive sex drive.
This results in the characteristic picture “of an animal that is not afraid of anything, has extreme curiosity about everything, forgets very rapidly, has a tendency to place everything in its mouth and sometimes even tries to eat solid objects, and finally, often has a sex drive so strong that it attempts to copulate with immature animals, animals of the wrong sex, or animals of a different species.”
It would be interesting to go through all the details of the lower brain structures to see what kind of symptoms would result from lesions in each part. However, what we have covered here is sufficient to see that it makes a great deal of sense for us to consider that mental and emotional diseases, as Hahnemann describes them, can be a result of localization of the disease to these specific structures.
Instinct
Let’s now consider the more complicated, what we may call “higher order”, behaviors, that have to do with the animal’s functioning in a broader sense. What I want to do is to address the issue of instinct vs. individual learned behavior.
We might all use the word instinct to refer loosely to behavior which is like a reflex, somewhat involuntary one might say. It is more than that. Instinct refers to a very specific pattern of behavior, sometimes a very complicated sequence of behaviors, that is not learned but is innate, that is inherited. These behaviors come with the territory so to speak and are not voluntary for these animals. They can be blocked or over-ridden by a stronger stimulus, such as fear but they cannot consciously or voluntarily be put aside. If the stimulus is there, the instinctual behavior will happen.
This is of great importance to us as veterinarians because, except for primates, almost all the behavior we deal with in our patients is of this type.
Where does instinctual behavior originate? This is associated with the higher centers, above the level of brain stem and associated structures we have already discussed. It is seated in the cerebral cortex.
The cerebrum is small in many animals and is gradually larger as we move towards the primates and human beings. This is associated, from the primates on, with the emergence of individual conscious functioning in these terms: ability to perceive and remember what are the relations between cause and effect with that knowledge taking precedence and overriding instinct. I will give you some examples of this in a moment.
Let’s first look at the size of the cerebrum in a few animals.
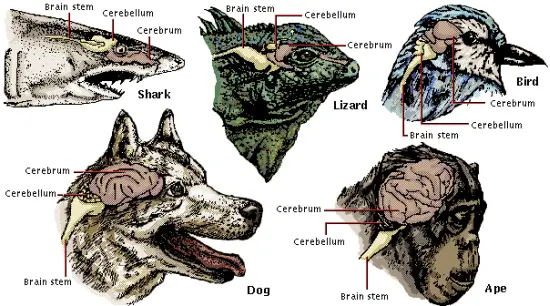 Cerebrum Sizes in Animals 1
Cerebrum Sizes in Animals 1
For most of the animals pictured, the cerebrum is a rather small structure. The ape in this picture shows the largest cerebrum of those illustrated, with the dog showing a much smaller cerebrum in proportion to the rest of the nervous structure. If we compare this with the lizard we see that it is very small. Now compare this to a picture of the human cortex and we see how extraordinarily large it is especially as compared to the animals in the above picture.
The Human Cerebrum 1
What do we mean by instinct? We all have the experience of seeing a fly repeatedly butt its head against a window glass in an attempt to reach the outdoor light. This may happen right next to an open door and yet any attempt to get the fly to move towards the open door and freedom is doomed to failure as the fly eludes our every effort and returns determinedly to its useless head butting behavior. We could say the fly is stupid, but more accurately, this is an example of instinct in which a perceptual/earning process that would over-ride that behavior is not possible.
Does this same instinct operate in larger animals, that is, larger than a fly? Indeed it does and here is an example that shows how that instinctive behavior is hereditary. It is taken from the work of Eugene Marais and his study on the instinctive behavior of termites and other insects.
Studies of the Weaver Bird
There is a bird that forms an extremely intricate nest requiring great skill in assembling the materials. It is called the “weaver bird” for the way it puts the nest together. Here is what it looks like.

Weaver Bird Nest 1
Eugene Marais studied instinct in these birds in a unique way. I quote him directly in what follows.
“Let us return again to the psychology of instinct. I said that the memory which constitutes this instinct is hereditary in the same way that the physical organs of the organism are hereditary. The following experiment which I myself carried out will explain what I mean.
The well-known yellow South African weaver bird, there are many kinds, but any kind may be used for this experiment, plaits a wonderful little nest at the extreme tip of a flexible branch, generally over water. You often see their nests at the end of the thin drooping twigs of the graceful weeping willow, but have you ever taken the trouble of watching to discover how the very first piece of grass is tied to the twig and what kind of knot the little bird uses ? The full-grown bird is a seed eater, but the little ones are fed on worms until it is nearly time for them to leave the nest. Remember these two instinctive memories:
- How to build the nest, and
- How to feed the fledglings.
I hatched the eggs of the yellow weaver under canaries, for four generations. The new birds were forced to lay eggs each time without being able to build their characteristic nest. This is the most difficult part of the experiment, but it can be done. Every time these eggs were hatched under canaries, the young ones were fed on a synthetic diet and were never allowed to see a worm or an insect. Nor did they ever see a piece of grass which might be utilized for building. Then I took this fourth generation and provided them with everything which they would need in their normal environment.
Remember now that for four generations they have not seen a plaited nest or tasted a worm. From personal experience the bird cannot possibly know what to do. There can be no question of individual memory. I expected at least that there would occur some deviation from normal behavior, but it was not so. When the time arrived for nesting, the birds began plaiting vigorously. They made more nests than they required. This often happens in nature as a means of protection. The eggs were hatched and the young ones were fed on worms! This experiment shows what I mean by the inherited memory of instinct.”
This little experiment shows how persistent is instinctive memory and also how that memory is not corrupted even though it was not expressed for four generations.
This instinctive behavior can be a disadvantage when there is very dramatic and rapid change in the environment if the rapidity of the change does not allow time for evolutionary adaptation. Here is an example of the inability for individuals to adapt (as opposed to the change in the species) led to extinction of the animals.
Extinction of Springboks
“I also said that the psyche of inherited memories is aforce which cannot be turned aside even by death if escape means behavior which conflicts with the race memory. As an example of this I will tell you about the case of the springboks on the Springbolakte in Waterberg. This lakte or plain is an island of open veld in the middle of the Transvaal bushveld.
The springbok is highly specialized for life on the open plain, in other words all his inherited memory is of open plains. He knows how to escape the perils which threaten him there; he knows which is the best food for him there and how he can find this; he knows when and how to change his quarters. He can see and smell over great distances. On this plain there were, twenty years ago, thousands of springboks. Now they have been exterminated.
Slowly but surely people have crowded there, made farms, fenced off camps, and destroyed the springboks. To the west rose the mountains and to the north lay the endless bushveld, where they would have been absolutely safe. Death lay on the one hand and safety on the other, but they could not take the step which would have saved them. Thousands of other big game, less specialized, fled into the bush and saved themselves from extinction. Often it happened that herds of Springbok were chased by hunters into the bushveld. Always they returned – sometimes the very same day – to meet death on the open plain.”
We see from this last example how instinct is an overriding determinant in behavior. Even when there is danger, an animal dominated by instinct will enter into that danger because it does not have the ability to withstand it, or the ability to reason beyond it.
This is significant because many of the behaviors we are asked to help with are of this type. Some examples that come to mind for me are:
Cats
Urinating outside a litter box.
Spraying urine on walls, furniture.
Grooming excessively, to the point of creating lesions.
Attacking new cats (or people) entering the home.
Killing kittens that are not theirs.
Crying out (yowling) in the night or when alone.
Eating cat litter, paper, plastic, indigestibles.
Vomiting foods that are not agreeable.
Refusing to eat or drink when ill.
Dogs
Suspicion of strangers entering their territory.
Attacking cats and other small animals.
Aggressive behavior to other dogs.
Desire for company.
Digging holes in the yard.
Scratching/digging behavior in the house, on carpeting.
Escaping confinement and wandering about.
Rolling in decayed animals.
Eating stool or drinking urine.
Scratching the ground after a bowel movement.
Understanding that these are instinctual behaviors helps us to realize that, when these behaviors are inappropriate, that some inflammation or irritation in the cerebral cortex is triggering this behavior and it is not voluntary for the animal. It may be possible to inhibit it with another stimulus, fear or distraction or by training (conditioning) that will interfere with the sequence of actions. But this happens not because they have reasoned it out and seen the relationship between cause and effect.
How does this contrast with what is more familiar to us, voluntary behavior? Eugene Marais gives us an excellent comparison in a parallel experiment in which an otter and a baboon were raised artificially and away from their natural conditions.
An Experiment Comparing Instinct With Learned Behavior
“Both baboon and otter were taken away from their mothers shortly after birth. The baboon was reared under our own supervision by a human foster-mother. The baby otter, whose captured mother died from wounds immediately after its birth, was placed among a litter of puppies and accepted by the bitch. Both were carefully kept from all contact with their own kind and all knowledge of their natural environment.
The otter was reared thirty miles from the nearest running stream. The only water supply in the vicinity was in a deep well, and it never, at any one time, saw more water than was necessary to quench its thirst. It never saw a fish or crab and was fed exclusively on raw meat. Then fully grown, it was taken for the first time to a river pool. It ran down to the water, smelled it and drank some. Then it struck the surface two or three times with its paw and immediately plunged in, diving, swimming and ‘playing’ just as a wild otter does. It had not been fed for some considerable time, and within half an hour it had captured a small fish and then a crab.
Our artificially reared baboon came from a district where its natural food supply would have consisted almost exclusively of insects and wild fruit. The wild baboon obtains insects by turning over all big stones in its line of march and is especially fond of the very abundant scorpions. This is a delicacy relished by wild baboons throughout South Africa and they show great ingenuity in catching them. The scorpion is rapidly beaten about with the hand until half-dazed, and is then turned on its back by a flick of the fingers and seized by the legs. In this position it cannot sting. The tail containing the sting and poison sac is carefully removed before eating. I have never seen a wild baboon stung by a scorpion during this process.
Among the wild fruit commonly eaten there are several tempting-looking drupes and berries which are poisonous. Two species of fruitbearing shrubs are remarkable because of the very close resemblance they bear to each other. These are the sandappel or the grysappel and gifblaar. The fruits are very different in colour and size, but the plants themselves can hardly be distinguished from one another. The fruit of the gifblaar is bright red in colour and very tempting in appearance—but the plant secretes a strictuous poison of extreme virulence and the fruit is especially rich in the deadly substance. The fruits of the two plants are far less conspicuously coloured. Both are edible and much esteemed by wild baboons and their human neighbours. I have never seen a wild baboon meddle with a poison plant or attempt to pick a poison fruit. They carefully avoid them. Quite small youngsters seem to know the danger. How the individual acquires this knowledge I am not sure, but not even in their case would I care to suggest purposive maternal tuition.
To this, its natural environment, our captive baboon was suddenly introduced for the first time when it was nearly full grown. It had been deprived of food for long enough to make it extremely hungry, but although it was in the midst of unturned stones covering innumerable insects, it had no idea of turning them over, nor could direct suggestion awake any hereditary memory. When a stone was turned exposing a number of scuttling beetles and scorpions, it leaped away in terror and for a long time it showed the greatest fear of a scorpion. After a great deal of coaxing it was at length induced to eat two from which the stings had been removed. It was then shown a third one under a stone and this time it greedily seized the insect and was promptly stung in the palm of the hand. Each kind of wild fruit it handled with the greatest caution, first smelling it repeatedly and then nibbling small bits. When it was eventually introduced to the two plants mentioned, its confidence had grown to such an extent that it plucked and ate a grysappel without hesitation. There was just a little hesitation when it reached the poison plant. It picked a fruit and at once placed the whole of it in its cheek pouch and when it was prevented from plucking another, it at once commenced chewing the one it had. It was only then that the sense of taste must have come to the rescue, as the masticated fragments were at once ejected with every sign of distaste and fear, and never after that could our (baboon) be induced even to handle the leaves or fruit of the gifblaar.”
We see the striking deficiency in the animal that does not inherit active instinct and the necessity to have individual experience and learning. Yet, the advantage of immediate perception and learning is apparent to us. The animal immediately has learned to avoid a poisonous fruit and will never eat it again as a result of this one experience. Contrast that to the slow learning of a species (in contrast to the individual) that can take centuries.
For example, in a footnote to this experiment with the baboon is this observation:
“All wild ruminants in the district where this plant grows avoid it instinctively, but domestic animals never learn its danger either by direct individual experience or through heredity and large numbers of cattle, sheep and goats are killed annually. Even the native cattle, which have probably had centuries of experience, eat it just as readily as the newly imported animals. Those that recover are often repeatedly poisoned by the gifblaar and dogs are sometimes also killed through eating the ripe fruit.”
What Happens To Instinct In The Higher Animals?
A question that comes up is what has happened to instinct in primates and human beings? Is it completely gone? We know that there is some instinctual behavior seen in human infants and hints of this in some areas of our experience. Almost all instinctual behavior has to do with eating or sex in animals and in human beings there are some residual instinctual actions that can still be recognized as in this category. An example is the preference or aversion to certain foods or the craving of foods, or even indigestible material like will happen in children that eat paint.
The interesting finding is that instinct is not really gone but submerged or dominated by a completely different function, the conscious learning mode. Every now and then, under certain unusual circumstances or in idiot savants, one will see evidence of instinct once more coming to the fore.
Here is a very interesting story of the return of an animal quality sense of smell in a young man. It has special relevance to us because the sense of smell is the primary sense in animals, while vision is the most important for us.
The Boy Who Could Smell Like A Dog
Stephen, a 22 year old medical student and high on cocaine, PCP and chiefly amphetamines had a major shift in this perceptual world.
“In a vivid dream one night, he dreamt he was a dog, in a world unimaginably rich and significant in smells. (‘The happy smell of water…the brave smell of a stone.’) Waking, he found himself in just such a world. ‘As if I had been totally color-blind before, and suddenly found myself in a world full of color.’ He did, in fact, have an enhancement of color vision (‘I could distinguish dozens of browns where I’d just seen brown before. My leather bound books, which looked similar before, now all had quite distinct and distinguishable hues’) and a dramatic enhancement of eidetic visual perception and memory (‘I could never draw before, I couldn’t “see” things in my mind, but now it was like having a camera lucida in my mind—I “saw” everything, as if projected on the paper, and just drew the outlines I “saw”. Suddenly I could do the most accurate anatomical drawings.’) But it was the exaltation of smell which really transformed his world: ‘I had dreamt I was a dog—it was an olfactory dream—and now I awoke to an infinitely redolent world—a world in which all other sensations, enhanced as they were, paled before smell.’ And with all this there went a sort of trembling, eager emotion, and a strange nostalgia, as of a lost world, half forgotten, half recalled.
‘I went into a scent shop,’ he continued. ‘I had never had much of a nose for smells before, but now I distinguished each one instantly—and I found each one unique, evocative, a whole world.’ He found he could distinguish all his friends—and patients—by smell: ‘I went into the clinic, I sniffed like a dog, and in that sniff recognized, before seeing them, the twenty patients who were there. Each had his own olfactory physiognomy, a smell face, far more vivid and evocative, more redolent, than any sight face.’ He could smell their emotions—fear , contentment, sexuality—like a dog. He could recognize every street, every shop, by smell—he could find his way around New York, infallibly, by smell.
He experienced a certain impulse to sniff and touch everything (‘It wasn’t really real until I felt it and smelt it’) but suppressed this, when with others, lest he seem inappropriate. Sexual smells were exciting and increased—but no more so, he felt, than food and other smells. Smell pleasure was intense—smell displeasure, too—but it seemed to him less a world of mere pleasure and displeasure than a whole aesthetic, a whole judgement, a whole new significance, which surrounded him. ‘It was a world overwhelmingly concrete, of particulars,’ he said, ‘a world overwhelmingly in immediacy, in immediate significance.’ Somewhat intellectual before, and inclined to reflection and abstraction, he now found thought, abstraction and categorization, somewhat difficult and unreal, in view of the compelling immediacy of each experience.
Rather suddenly, after three weeks, this strange transformation ceased—his sense of smell, all his senses, returned to normal; he found himself back, with a sense of mingled loss and relief, in his old world of pallor, sensory faintness, non-concreteness and abstraction. ‘I’m glad to be back,’ he said, ‘but it’s a tremendous loss too. I see now what we give up in being civilized and human. We need the other—”the primitive”—as well.’
Sixteen years have passed – and the student days, amphetamine days, are long over. There has never been any recurrence of anything remotely similar. Dr D. is a highly successful young internist, a friend and colleague of mine in New York. He has no regrets – but he is occasionally nostalgic: ‘That smell-world, that world of redolence,’ he exclaims. ‘So vivid, so real! It was like a visit to another world, a world of pure perception, rich, alive, self-sufficient, and full. If only I could go back sometimes and be a dog again!”
Reading the account of the emergence of smell as the primary sense gives us somewhat of an idea of how different the animal experience is from ours and also how immediate and impulsive it is. It also allows us to realize how many of the animal behaviors have become submerged in us.
An Example of Higher Order Functional Change
When we come to the level of human functioning and study the details of behavior that can appear during illness then we can extrapolate back to our animal patients to some limited degree. We can realize how interests and preferences can change – though in animals it is more difficult to see the detail that is possible in the human being. Here is an example of what I mean. It is the report of a 52 old man who changed drastically after losing his wife.
“At the time of his wife’s death, John Carter was a shy and conservative 52-year-old man whose most distinguishing traits were an uncanny ability to remember numbers, a two-stroke golf handicap, and a profound devotion to his wife. So the prolonged grieving that followed her death surprised no one. But when John decided to leave his brokerage firm and become an artist, his family and friends were shocked. To their knowledge, John had never before shown any interest in art whatsoever; indeed, he might have been the only man in his Connecticut suburb who had never visited an art museum. To his college-age twin daughters, John explained that he was feeling bombarded by colors and sounds. His life, he said, had to change. He moved to a simple loft and started dating art students, many younger than his daughters. He gave up eating meat. He began wearing loud purple shirts and yellow pants, attire that seemed silly to those who knew the former John. He began to fill canvases with streaks of purple, yellow, red, and green. They impressed no one. Still, no one doubted that John was in great mourning, and if the price of being an artist was living with an extreme intensity of feeling, then he was paying that price.
John began to tell friends of his new ability to see not only colors but sounds. Sometimes, he explained, he felt open; during these periods, colors bounced through his head like notes of music, and each shade of the rainbow vibrated with a clarity that could bring him to tears. On these open days, John was warm and mellow, spending many hours painting in solitude, leisurely capturing on canvas the beautiful hues and images of flowers and animals that raced through his mind. When he felt closed, though, he was sad and irritable, grimacing at the bark of a dog or an intrusive shaft of sunlight.
No one can remember exactly when John’s paintings began to appeal to the eye, but it seemed to happen around the same time that he began to have trouble remembering the meaning of words. At first people assumed that John was kidding when they would say a common word like key, and John would repeat back, “Key, key, what’s a key?” With time, John comprehended fewer and fewer words, and the words he chose to convey his own thoughts became more and more simple. John had been an articulate man. But within three years there was little trace of his formerly rich speech. He conversed in short, simple phrases, like “I feel open” or “I feel closed.”
As his speech became more impoverished, John grew more flagrant in scorning social rules. One day the police called his daughters to bail their father out of jail after he had appeared nude in a public swimming pool. Other days, John walked the streets of the city, intentionally bumping into and berating strangers. His temper grew so vicious that he began kicking his dog. His daughters began finding pens that John had swiped, and they noticed his tendency to steal tips off restaurant tables. Soon John required caretakers around him 24 hours a day to prepare his meals, wash his clothes, calm his moods, and keep him out of jail. His compulsions grew stronger. He often dragged his caretakers past banks, phone booths, Laundromats, and restaurant tables, hunting for dropped coins.
Unexpectedly, as John’s social skills and language abilities eroded, his visual senses became more acute. He found coins that no one else would have found, and he became exquisitely sensitive to sudden changes, such as subtle shifts in the weather. John devoted these new visual skills to his painting.
Over the years the complexity of John’s art increased. His early paintings had featured simple colored lines; now he was exploring interesting rounded shapes. For several years, he painted richly colored flowers, boldly laid over a stark monochromatic background. At age 58, some five years into his illness, John spent three weeks in Hawaii, where he felt open almost every day. After returning home, he re-created from memory the beautiful birds of Hawaii, usually in purple and yellow. These tropical birds-perhaps his most attractive pieces-evoked the feeling of another world. Several won prizes at local art shows. Yet this accomplishment seemed to give him little pleasure, and by the time he received the awards, John was a shell of what he had been. His daughters sought medical opinions about his condition; diagnoses ranged from Alzheimer’s disease to depression to schizophrenia. No medication helped.”
With time, John deteriorates even further as to use of language and in his behavior but his art develops in extraordinary ways. After several years imaging studies “revealed diminished function in the front of his temporal lobes – a region that is involved in many social and perceptual tasks.”
“The rear part of the temporal lobe is involved in our ability to visualize images; the rear part of the parietal lobe is involved in our ability to put those visual images on paper. That helped explain John’s unusual condition.”
Though much more could be described about this condition, what I wanted to point out here is how the condition in this man was localized as a lesion in the cerebrum and resulted in a shift in both how perception was experienced and also what was of interest to him. He made the rather dramatic switch from a man who worked with stocks and numbers to one completely focused on color and art.
Can we see these kinds of changes in animals? Theoretically, at least, I think we can. Now and then we run into the animal patient that has made a noticeable shift in personality, developing interests and activities not seen before. Perhaps what we are seeing is the effects of a lesion that has focused in the cerebrum.
A Most Interesting Footnote of Hahnemann
I have one more thing I want to address that I think is especially interesting. In this same section of the Organon on mental and emotional diseases, there is this footnote containing advice on temperament changes in patients.
“…One often encounters patients with the most painful, protracted diseases who have a mild, gentle emotional mind such that the medical art practitioner feels impelled to bestow attention and sympathy upon them. If the physician conquers the disease and restores the patient again, the physician is often astonished and startled at the dreadful alteration of the patient’s emotional mind. The physician often meets with ingratitude, hard-heartedness, deliberate malice and the most degrading, the most revolting tempers of humanity – qualities that were precisely those possessed by the patient in former, healthy days (my italics).
One often finds that people who were patient in healthy times become, in disease: stubborn, violent, hasty, and even insufferable, self-willed and in due succession, impatient and despairing. Those who were formerly chaste and modest often become lascivious and shameless. Not seldom, one finds that bright people become dull-witted, those who are usually feeble-minded become more clever (as it were, more sensible) and the slow-witted occasionally become full of presence of mind and rapid resolve.”
Isn’t this an extraordinary statement by Hahnemann? Most of us would think just the opposite, that the nasty person that emerges from successful homeopathic treatment is what needs a remedy! What Hahnemann is stating here, as he has elsewhere, is that the guide to treatment is not the usual, normal personality but the changes that occur in association with the illness.
Still, an explanation is needed here. How can we explain this alternation of almost different personalities? From “gentle & emotional” to “ingratitude, hard-heartedness”, from “feeble-minded” to “more clever”? I have seen these things myself and been surprised at them.
In an attempt to provide an explanation for what is happening, I will draw on some recent findings in brain research that may provide an answer for what Hahnemann observed.
Split Brain Studies
In the 1970’s a new and drastic surgery was performed on some patients for which no treatment had been effective. These were people like children that had continued epileptic seizures, or people that had tumors that required resection in their removal. What was done was to split the brain into two parts by cutting the connection between the right and left cerebrum. If we look at this picture of the human brain from the top we can see how the two sides are naturally divided.

Human Cerebrum, Top View
Though the brain is divided the two sides are joined at the base (not visible here) by a broad thick band called the cerebral commisure. It is this structure that allows communication between the two sides of the brain.
We have all probably learned that the two sides of the brain have somewhat different functions and though there can be exceptions for most people it is like this.
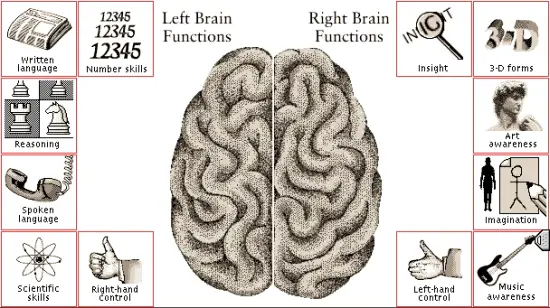
Right vs. Left Brain Functions 1
Given this arrangement, what happens when the brain is separated so that the two sides cannot communicate with each other? Surprisingly, for the most part you would not be able to see any difference in such a person. As long as the left brain was functional there would still be speech and logical thinking and having a conversation with that person would seem to be normal. However careful study of such individuals has shown a most extraordinary thing – that there exists two different personalities, one on each side, one in each cerebrum.
It is possible to use tests to demonstrate this. For example, the left brain controls the right side of the body and the right brain the opposite side. It is possible to set up a situation that visual information can be given to just one side of the brain, even different information to both sides at the same time! It has been learned that each side functions independently with different attitudes and preferences.
In the normal intact individual one side dominates the other and integrates the information from the other side into its functioning but when they are separated that dominance is removed and both sides function independently. One of the strangest things is how, in some of these people, the two sides can come into conflict. Here are some examples.
- A patient had to wrestle with his left arm (controlled by his separated right brain) to keep it from striking his wife against his (left-sided) will.
- A split-brain patient consciously wanted to smoke, but each time he lit up, his left hand (controlled by his right brain) would grab the cigarette and, to his dismay, put it out.
- A split-brain patient was awakened by a hand slapping her across the face. Her alarm clock was going off, and she realized she had overslept and was going to be late for an appointment. The hand that had aroused her was her own left hand! While her left brain was asleep, her right brain awoke and appreciated her predicament.
When the brain has been separated, then the usual communication is interrupted and the non-verbal brain has to take extraordinary measures to get its message across, literally. It is important to realize that even though the right brain is not verbal, it is still just as intelligent as the left side.
Here is a transcript of an experiment in which a photograph was shown to just the right brain of a person in which the two sides were separated and the left brain was asked to identify it.
“Here LB’s right brain was shown four photographs simultaneously. His right brain could scan the photographs as you or I could if they were placed on the table in front of us.
The experimenter says, “Point to any of these that you recognize.”
After fourteen seconds, LB’s hand points to a photograph that pictures the only person who is recognizable, a well-known figure who is standing with four other people. The other photographs are of people unknown to him.
Experimenter “Do you recognize that one? Is that the only one?”
LB again inspects the photos but does not point to any others.
Experimenter: “Well, on this: is this one a thumbs-up or a thumbs down item for you?”
LB signals thumbs down with his left hand (connected to his right brain).
Experimenter: “Who is it?”
Now LB’s left, verbal mind answers (his right-sided mind can’t speak), “GI came to mind. I mean . . .”
The experimenter notes that LB’s left hand (connected to his right brain) is trying to trace letters on the back of his right hand. That is, his right brain is trying to tell his left brain the name of the person in the picture. The experimenter says, `’You’re writing with your left hand; let’s keep the cues out.”
LB’s speaking left-sided mind says, “Sorry about that.”
Then the experimenter asks, “Is it someone you know personally, . . . or from entertainment, or . . . historical, or. . . ?”
LB’s left brain (which did not see the picture) interrupted and said, “Historical”.
Experimenter: “Recent or. . . ?”
LB: “Past.”
Experimenter: “This country or another country?”
LB: “Uh-hu-okay.”
Experimenter: “You’re not sure?”
LB: “Another country, I think.”
Notice what has happened. LB’s left-sided mind was speaking. He did not see the picture, but he apparently had a feeling or an intuition “sent” to him from his right-sided mind because his guesses thus far were correct. These feelings were probably sent through the lower brain levels, which were not cut by the surgery.
The experimenter then asks, “Prime minister, king, president, . . .any of them?”
LB has a ponderous look on his face and says, “Gee.”
Experimenter: “Great Britain? . . . Germany. . . ?
LB then interrupts and asserts, “Germany,” and then after a pause,
“Hitler.”
The left brain never saw the picture and without its usual connection to the other side had great difficulty receiving the information. Further research has shown much evidence that the two sides function independently with different interests and preferences in food, clothes, friends, etc. Here is a little example of this.
“Initially, his right mind couldn’t speak, but it could communicate by spelling words with Scrabble chips. The experimenters would ask questions such as, “What is your favorite?” Then they would flash a word such as “hobby,” so it could be seen by only one hemisphere. When the experimenters asked his right mind what it wanted to be when he grew up, it spelled out “auto race,” which the experimenters interpreted to mean that he wanted to become a race car driver. When they asked his left side what he wanted to become, he replied, “a draftsman.”
It is interesting that Paul’s left side appeared to be more conservative, more reasonable, perhaps more mature than his right side, which seemed possibly more impulsive, unrealistic, and immature. When his right side was asked, “Who [are you]?” he wrote, “Paul.” This shows that his right mind had a sense of himself as a person, a personal identity.”
Is The Appearance of Two Minds in the Same Body the Natural State?
It is not too long before the question naturally arises. Does a new personality form at the instant that the commisures are severed, or is it already the case that there are two personalities in the average intact person? Further research suggests that the latter is the correct view, that there are two personalities in every human being and also in animals. Perhaps we could think of the mind as being bilaterally symmetrical, like are the kidneys or the arms and legs!
Some of this work comes from animal studies and is of special interest to us as veterinarians.
Split Brain Studies in Animals
“There is a large body of split-brain studies in animals (without epilepsy, of course), and these studies also show the same duality of mind. Prior to his work on human split-brain patients, Sperry had been experimenting with cats and monkeys in which he would cut the corpus callosum. He also cut the optical chiasm, the point where the nerve tracts from the eyes cross to the opposite side. By this operation, he constructed an animal with not only a split brain but also an eye connected to only one hemisphere. Following surgery, Sperry covered one eye and taught the animal a trick or two. For instance, he could teach the animal that to get a food pellet, it had to push a button with a circle on it rather than the button next to it with a cross on it. What he found was dramatic. He could teach the animal’s left brain, and only its left brain would learn the task; its right brain would remain untaught. He could then teach the right side to do the opposite – that is, to push the cross button to get food. Then, depending on which eye was uncovered, the animal would push either the circle or the cross.
Sperry discovered that the split-brained animal acted as if it had two minds, each unaware of what the other had learned. Each mind was capable of perceiving, learning, remembering, and initiating action. This work in animals dovetailed with the discoveries of two minds in human split-brain patients and proved that the phenomena cannot be attributed to epilepsy or some unspecified, undiscovered brain damage.”
To confirm the existence of two minds in the average person is a difficult thing to do. Few would want their brains severed for the purpose of an experiment! So, another way of finding out more uses temporary anesthesia of one side of the brain. Here is an example of its use.
More Evidence of Two Minds in Ordinary People
“Another piece of evidence that the split-brain findings relate to normal people comes from a variation of a procedure long used by neurosurgeons prior to brain surgery. In order to locate definitively the patient’s centers for expressive language and memory (so they are not removed unintentionally), the surgeon uses a procedure referred to as the Wada test, after the physician who developed it.
It consists of injecting sodium amytal, a short-acting anesthetic agent, into either the left or right carotid artery (these arteries support the parts of the cerebral hemispheres most related to higher mental functions). The brain on the side of the injection becomes anesthetized, and the other half remains awake. Actually, for the first three minutes or so after the injection, both sides of the brain become dysfunctional. Then the side opposite the injection recovers rapidly, while the side of the injection remains anesthetized for another 10 minutes or so. When the right side is injected, the patient, after the initial brief dysfunction, regains his usual consciousness and can converse fairly normally. The left side of his body remains paralyzed for the fifteen minutes or so during which the anesthesia lasts.
When the left side is injected, after the brief period of dysfunction on both sides, the patient’s right brain is awake, even if somewhat groggy, while his left-sided, verbal mind remains anesthetized. Usually the right brain cannot speak.
When the test is conducted in its usual way, it is interesting, but it doesn’t tell much about the nature of the right brain. However, an interesting study by Dr. Risse and Dr. Gazzaniga begins to reveal more about this hidden side. They used the Wada procedure to anesthetize the left brain; while the left side was unconscious, they placed objects in the subject’s left hand (right brain). When the subjects (left brains) woke up, none of them consciously had any idea about whether anything had been placed in their hands. Yet when they were shown an array of pictures of several different objects, they easily pointed to the correct one. This study implies that the right brain functioned independently of the left brain; it was able to appreciate, remember, and retrieve the object – all without any participation of the left brain. In this study the patients were not split-brain patients, but had whole, surgically intact brains.
Another Wada study lends support to the idea that each hemisphere can possess a mind of its own. Dr. Geoffrey Ahern and his associates reported fascinating results in separate Wada tests performed as part of an assessment for epilepsy in two young men. The patients were unusual in that each had demonstrated two distinct personalities, and in each case Ahern demonstrated definitively that one personality was coming from the left hemisphere and the other from the right.
One patient’s usual personality was emotionally withdrawn and sullen, but for an hour or so after a seizure, he became affable and sociable. His family reported that the changes in personality were profound – that he was like a different person.
When the doctors injected the patient’s left carotid artery with sodium amytal and anesthetized his left brain, he smiled and laughed and appeared to the doctors to be much more emotionally spontaneous than he was in his usual state. During the test, he was asked if this was what he felt like when he was in his positive personality, and he responded affirmatively.
During a Wada test, the anesthesia gradually wears off after five to fifteen minutes. As the left brain was coming out of its sleep to wakefulness, the patient said, “I think we just got done with the niceness.” He then indicated that the drug was wearing off quickly and made a chopping motion with his left hand (controlled by his right brain). He then abruptly had a personality change back to his unemotional, unsociable self. His left brain had apparently woken up and taken control.
The doctors then engaged in the following conversation with the patient:
Doctor: “Did you, I mean the emotional part, like coming out here by yourself today?”
Patient: (turning his head and eyes to the right, indicating that his left brain is talking) “No, not really!”
Doctor: “So you wouldn’t want to come out again, by yourself, without the ‘talky’ [left] hemisphere?”
Patient: “What’s that?”
Doctor: “The emotional part of you. I’m talking to that part of you right now. Would you want to come out by yourself again, or do you like being back in there suppressed and quiet?”
Patient: (with very flat affect, suggesting that his left side is speaking) “I’m just naturally a suppressed and quiet person.”
Doctor: “You’re not going to let him talk, are you?”
Patient: “Who’s that?”
Doctor: “Your other side.”
Patient “It all depends on what the other side says.” (The patient then smiled, but only on the left side of his face, controlled by his right brain. )
The second case Ahern described was also a young man suffering from seizures who had also been observed to have dramatic personality changes. This patient’s usual personality was well adjusted, but after a seizure, his personality became extremely aggressive and disruptive. His seizure activity came from his left hemisphere, and after his seizures, his left brain would be severely inhibited by exhaustion, and his right brain would become dominant. This suggested that his disturbed personality might be associated with his right brain.
During the Wada test, when his right brain was put to sleep with sodium amytal, he remained his usual pleasant, well-adjusted self. When his left brain was made inactive, he again became his belligerent personality. In fact, he became so verbally and physically abusive that the doctors had to inject him with an antipsychotic medication.
The results of these experiments reveal that these two intact people, who had never undergone a split-brain operation, obviously were of two separate minds – one left and one right. In the first patient, the disturbed personality was associated with the left hemisphere. In that patient, an MRI showed some nonspecific scarring, suggesting that his left brain may have been damaged. The doctors speculated that his psychiatric problems might have been related to that possible damage, since his disturbed personality was located on the left side. In the second patient, the disturbed personality was associated with the right hemisphere.
Ahem’s study is remarkable because it is a clear demonstration of two distinct personalities, one in each hemisphere, present in two patients not given split-brain surgery.
An Experiment
I would like to try an experiment here with all of you that would like to see if you can experience for yourselves a difference between the right and left minds. The anatomy is complex to explain but it is possible for us to restrict vision so that one hemisphere is primarily receiving visual images. With that one hemisphere active some of you, about 40%, can feel a difference for yourself. What will it feel like? Comparing one side to the other you will feel a shift in mood, in emotional tone, as in level of anxiety or confidence or happiness.
Here is how we will do it. First cover your left eye completely with your hand. Then, with the other hand, cover the left half of the right eye visual field (the side near the nose) so that you are seeing only out of the right half of the right visual field. Then look to the right so you are seeing only out through that limited view. In this way, you are sending signals only to the left hemisphere.
After you have done that for a minute or so and checking how you feel inside, then switch to the opposite arrangement: cover the right eye completely, and the right half of the left visual field. Turn your eyes so you are looking to the left. Now the right hemisphere is receiving stimulation. Do you feel a difference in mood or emotional state? About 40% of the people that try this feel a distinct difference.
If this finding that there are two personalities or minds in ordinary people is correct, then we can relate this to Hahnemann’s observation of the alternation of personalities in his patients. Just as the dominance of hemispheres has been seen to shift under the influence of drugs or from epilepsy, it may be a common event that this happens during illness from a variety of causes. Some of us have certainly had the experience that our wife or husband will become like another person when ill. Certainly food for thought.
Summation
We have covered a lot of ground with this topic. Let’s see if we can pull it all together. Hahnemann tells us that these mental and emotional diseases start as physical illness and, because of the influence of psora, become one-sided cases with the focus of the disease on emotional symptom. We see that the localization that he refers to can be development of a lesion somewhere in the brain – where it ends up causing behavioral symptoms that can be very frustrating to treat.
In animals, these lesions, if they involve the cerebrum, will trigger instinctual behavior which is difficult to understand out of context with the natural conditions that usually elicit it. In human beings, it is not instinct but voluntary behaviors – interests, preferences, desires – that change with the same cerebral condition. From research we are able to realize that the balance between the different parts of the brain will underlie these changes. As in the case of the man who became a painter, it was the change in balance brought about by loss of temporal function that changed his whole perspective.
Then we looked at Hahnemann’s observation of the change of personality in sick patients, sometimes to the opposite type of character. Linking this to recent discoveries that we each have two independent minds with one of them dominant most of the time, except under certain conditions that allow the relationship to be reversed, we can see how this could have been a true observation on Hahnemann’s part.
I know this last finding seems too strange to be believed and it may be that it is not correct. But for what it is worth, Roger Sperry received the Nobel prize in 1981 for this work with the split brain condition in which he demonstrated the existence of two minds in one body.
Treatment
What does this say for our strategy of treatment? I think one thing is that we need to understand the importance of mental and emotional diseases being a transformed physical condition. Hahnemann says the way to treat them successfully is to look back into the history and find the physical symptoms that preceded the emotional symptom that is dominant now and that the curative remedy must cover both. So, this tells us what we intuitively knew – that we cannot split the patient into physical and behavioral. They are one functioning whole.
Hahnemann attributes these diseases to psora relegating the various triggers such as emotional upset, fright, worry, bad experiences and so on to relatively minor roles, as just that – triggers of an underlying psoric condition that has been latent. So, the successful treatment of these mental and emotional diseases will require the use of antipsoric remedies at some point in the case.
Lastly we must take to heart Hahnemann’s emphasis to treat the changes in temperament that occur in illness and not what was the normal personality before. As in the footnote we discussed, in which the patient can become quite unpleasant after the cure is achieved, we must realize that a return to normal may not be quite what we think is ideal. Hahnemann does make a distinction between the life force and the human spirit which is different.
This latter is not considered to be an object of homeopathic treatment but, rather, is to be addressed, according to Hahnemann, through reason and love. The usual personality is an expression of the spirit, and though it can become imbalanced as part of illness and this can be a guide to treatment, we cannot expect that we can change personality through homeopathic prescribing.
Guyton, Arthur C., Textbook of Medical Physiology, Sixth Edition, W. B. Saunders Company, Philadelphia, p. 902.
Guyton, Arthur C., Textbook of Medical Physiology, Sixth Edition, W. B. Saunders Company, Philadelphia, p. 705.


The most difficult of topics dealt with wonderfully. Hope every doctor makes use of it.
Very good article as an academic and comprehensive point of view, but straight clinical prescribing tips are not found.
Excellent Article. I submit that more such elucidatory writings are required for homeopathy lovers. If clinical tips too are mentioned that would be still better. God bless all.
Very interesting & knowledgeable article.
Brilliant, thank you!
Where can I buy “arthur guyton 6th edition encyclopedia medical physiology?”
I am happy having this interesting & knowledgeable article. I collect it for translation for my future use. It will helpful to understand the mental symptoms of the patients. Thanks to all with websites.