After studying intensively for 15 years, from every book I could lay my hands on and from every Master that I had the opportunity to see at work in seminars, I somehow came to my personal understanding of homeopathy, which I refer to as “The Vital Approach”. At first it was a little word game as my initials are AV and I called it the AV method or the VA, both of course meaning the same thing. The reason for this was that in 2005, understanding the essentials of homeopathy better, (see “The Charm of Homeopathy”, pub. B.Jain), I felt that a way of working required its own name.
This is the reason why
My quest to understand the nature of things is canalized by homeopathy, but another path, method or field could have served my profound philosophical endeavor. This blended with a lifelong interest in health, physical as well as mental, as a condition for sanity, harmony and happiness. And besides a lot of other interests, my background in linguistics and literature had its unavoidable influence. Having started writing at age ten and never stopped, I am the author of 9 novels and some short stories. I never stopped being amazed at the system, the power and the magic of language.
Is the Vital Approach classical homeopathy?
It sure is!.(although it might not always look like it). Classical homeopathy is what underlies it and it will be hard, if not impossible to grasp the depth of the VA without it. With classical homeopathy I mean the spirit of the teachings in the Organon. As a teacher I had to read it over every year for more than 15 years and as the cliché says: it becomes better with every reading..because clichés are also true. It also goes without saying that I consider knowledge of Materia Medica, familiarity with repertorisation and provings as necessary basic skills of every homeopath.
Is the Vital Approach not a version of the Sensation method then?
Rajan Sankaran has been my most important teacher for 15 years and when he launched his insights on the sensation level in 2002, it was but the logical next step in his evolution. It was clarifying and I gladly incorporated it in my anamnesis and analyzing techniques. Now, about 7 years later I’m able to see the advantages and disadvantages of it.
Then why not just call it the Sankaran method?
It is because the followers of Sankaran would say I don’t do it properly, and they are right. There are important differences I will explain in a minute. On top of that, Sankaran is not the only influence or input and I don’t want to be part of the Sankaran or non-Sankaran schism.
What are the differences?
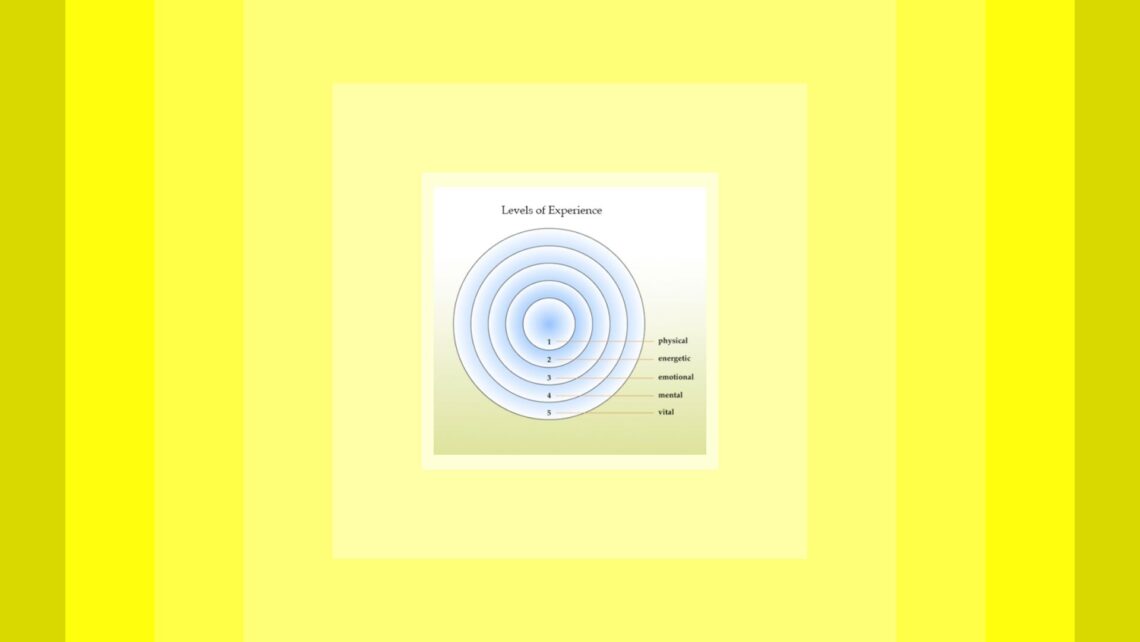
Sankaran works with 7 levels of experience which are divided in even more sublevels. While not denying they exist, I think for pragmatic reasons, 5 suffice. As you see on my diagram there are two levels representing the body and two representing the mind. Beyond that there is one more level (or ‘subtle body’ if you want) which I call the vital level.
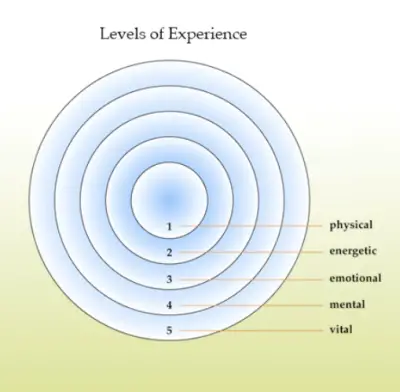
In the most simplified reading of the Organon, Hahnemann defines disease as a disturbance of the Vital Force, expressing itself with signs and symptoms (in sensations and functions) on mind and body. Because of that the seat of disease must be beyond mind and body and in deference to Hahnemann I named it the Vital level.
Sankaran’s level 1 represents the ‘Name’ of the disease while level 2 are the ‘Facts’. If the problem is gastritis (level 1), the facts (our ‘modalities’) make it individual: it’s ‘my gastritis’ and that is why different patients get different remedies for the same medical condition. On that level we can make a clinical prescription.
In my scheme level 1 is Physical, but always individualized pathology: you can only have your own gastritis; it isn’t possible to have somebody else’s and thus making a diagnosis only on the basis of a name is a non-existing reduction, not an actual level of experience. That’s why I left it behind.
My level 2 is called the Energetic level and is missing in Sankaran’s scheme. It is the invisible but measurable aspect of the physical body. It’s the level of the energy systems, the neurological, hormonal and immunological system in the body. They are not directly observable under the microscope but their effects in the physical body are. Disturbances lead to functional problems, rather than or before they become materialized in physical tissues and organs. Because doctors have no solution for these complaints of their patients (pain, sleeplessness, lack of energy, hormonal disturbances, itch, twitching, fatigue, chronic mild inflammation, flu like symptoms) they often search for alleviation of the suffering with us.
As far as I understand, the Hahnemaniann miasm theory is based on observations of what we would now call constitutional weaknesses. They are almost always expressed first on the energetic or etheric level before they manifest in the physical.
Level 3 in Sankaran’s scheme corresponds to mine (Emotional) but level 4 differs again in that in Sankaran’s scheme it is called Delusion, while I would prefer to call it the Mental level. It equals the Mind, and this is, believe it or not, a word you can’t translate to my language! So I have to call it the Psyche. It is structured and divided in the Conscious, Subconscious and Unconscious layer. Delusions belong to the unconscious mind. But our patients will also talk rationally, from their conscious mind and swop from one layer to the other during consultation, without realizing it. The bulk of our useful information comes from the subconscious layer. When we get information we don’t understand, it often signifies we moved into the unconscious.
Level 5, whether called Sensation or Vital, is more or less the same in Sankaran’s scheme and mine. Maybe one difference is that Sankaran’s, level 6 which he calls the Source or the Energy level, is somewhat incorporated in my level 5. Sometimes the patient will use gestures to emphasize his sensation or he almost ‘becomes’ his remedy. I would still consider it as level 5. I agree gestures are preverbal but in itself they don’t give us a clue as to what remedy to prescribe, except when it comes together with the words the patient uses to convey his sensation. (which in itself is a function of the mind and comes from level 4). The medium of the homeopath is language, words or body language, but language all the same. And Sankaran divides level 5 into another 3 sublevels.
Okay, a few modifications as to the levels, but are there more differences?
There are! The most important is that in my understanding we don’t have to guide the patient along the levels to reach level 5, but we can discern the sensation or the disturbed vital force or vital information on all levels. Because the expressions of the vital disturbance are on all levels all of the time. In Sankaran’s model the disturbance is The Other Song in a person. It is as if the Lion, the Arnica or the Arsenic is talking instead of the patient. And with the homeopathic remedy we try to turn the volume down of this stranger, in order to hear our own human song clearly again. In my understanding, the vital disturbance is nothing but an aspect of the patient. It belongs to him; it belongs to his most characteristic makeup, his essential being, to his very core. One might call it his soul. It’s like one instrument in his orchestra is out of tune and thus spoiling the whole play. If we give a remedy that resonates with that, it will tune up the patient and create harmony again (“restore” was Hahnemann’s word in his first aphorism, not “remove”)
One of the consequences of this theory, is that we listen in a different way. I found students trying to master the Sensation method often were bored as long as the patient was giving them information from levels 1 up to 4. As long as it was no sensation, they thought it worthless. Hence many times, although they tried hard, they couldn’t elicit the sensation, or they didn’t reach the sensation level and considered their case useless. Either they had (the delusion they had) a fabulous sensation case or they had a feeling of failure because they didn’t make it. On top of that, often the patient was blamed for not be willing, wanting, or capable enough to get to that deep a level and could only give ‘superficial’ data.
If you, on the other hand, know or believe that the vital disturbance or sensation is on all levels all of the time, then you can’t miss it! The patient can’t but give it to you, because he can’t hide himself. Even if he is not talking he will give expression to himself and the state he is in.
If you can get the vital experience directly, it is without any doubt the most reliable information to prescribe on. And our questioning should be aimed at that level. But my main advice to students in the Vital Approach is to listen very carefully to everything the patient says, because everything can be valuable information. The crucial thing is to discern vital from non-vital information on all levels, and that is what I am teaching for many years with live cases. Then I can explain clearly what in the patient’s words comes from which level and why.
All levels all of the time
There are many things to take into consideration which can’t be discussed in the limited scope of an article, but in general we can say that :
On level 1 we can’t use the pathology as such, but the way in which the pathology is experienced.
Level 2 will tell us about the generals of the case.
Level 3: We don’t prescribe on the story, but the message in the story; in other words, what is the story an example of. All common human emotions like grief, fear, anger, guilt, feeling of inadequacy and failure, not being appreciated or loved (enough) are no basis for prescription (aphorism 153).
Level 4: the rational explanations tell us something about the personality, but we don’t prescribe on that either. The subconscious information contains the real, intense, true, strong and unacceptable feelings and shows us the direction. But we still need the vital experience to be able to discern the kingdom for instance and make a sure prescription.
The unconscious level, container of myths and the experiences of all humanity often is confused with the sensation level. When we ask a patient to close his eyes and go deep into himself, the possibility exists that he makes contact with this layer, especially if he is encouraged to disconnect or enter a dreamlike state. He might then start talking from a source that doesn’t belong in his daily life, and the homeopath might think this is the Other Song in him. But it might be his ‘personal myth’ as well, written in his manuscript of this life story, or even some karmic imprints. But they belong to the psyche and thus to level 4.
By the way I’ve seen quick and fantastic cures taking place after administering a remedy on that level. Sometimes in no time symptoms disappear. But it is still treating the symptoms, not the patient. You know, when I taught students homeopathy for five years, the main thing they should have grasped is the difference between an effect and a cure. Many treatments, including homeopathy have good effects, but few really cure. And that I see on a daily basis is the potential of the VA.
From my point of view, only level 5 remedies touch the core of the patient and cure his soul.
More Advantages?
As mentioned before, to be able to discern the kingdom of the remedy that the patient needs, is invaluable in solving a case. It makes it possible to make a choice after we repertorized, because we can filter the outcome or restrict it to a particular kingdom (or miasm or both).For those who are not yet familiar with the kingdom theory, I’ll explain in short.
Let us take the example of a female patient suffering from headaches. After taking the case carefully we have the whole story: After a long and unhappy marriage, finally the husband told her he was having an affair and leaving her. Instead of giving Natrum mur on the basis of grief, we can try to understand how the patient experiences this event. If to her, it is like the foundation of her existence is taken away, as if she is incomplete without a partner, we have good reasons to consider a remedy from the Mineral Kingdom. Nat mur could be the remedy she needs. If on the other hand she feels hurt, injured and wounded, then we have to consider a Plant from the Asteriaceae (the miasm will us lead to the right family member). But when the patient feels he abused and degraded her, or he is the winner in this situation and she is the loser and she is full of hatred and revenge, then we are in the Animal kingdom. There are a few more kingdoms to consider but this will make my point clear. If we have the story we can’t make a sure prescription because we have symptoms from all kingdoms. But if we have the experience, we know in what kingdom we have to look for a suitable remedy.
Another advantage is that we can prescribe small remedies with the same certainty as the big ones we know so well, and have many symptoms for. For instance, we might understand we need a mineral remedy for a patient. We saw the Row four issues and the Third Column features and hence we can prescribe Scandium with full confidence. If we would have only repertorized the case, most likely the patient would have been given Calcarea. It is near… but unfortunately not the remedy the patient needs.
Is the Vital Approach hard to learn?
I don’t think so. It requires a whole lot of common sense and a firm basis in classical homeopathy knowledge. I think every earnest student can do that. It also necessitates a clear idea of what one is looking for in a case. Otherwise it will be impossible to evaluate whether it is found or not.
And as I said before, life cases are the best demonstration of the Vital Approach. With a life example it is easier to show how to select the Vital information or how to understand the kingdom. It takes a genuine curiosity from the homeopath, a wish to truly understand what it is like to be the patient. If he has eczema, we listen with full attention to every little detail of it, of how it presents, what aggravates it and ameliorates it, what triggers it, when it started, level 1 and 2 information) what the patient did so far to deal with it, what kind of treatment, with which reaction, (mostly miasm information) what the complaint makes him feel like, what it does to him, how it is experienced, (level 4 and 5). In every problem in the patient’s life, his state is active and expressed. In the part is the whole.
Another important recommendation in my Vital Approach is to not interfere in the beginning of the consultation. Being very cautious not to lead the patient anywhere, the best approach is to not even point in some specific direction. Our questions often are the reason we miss the case: we chose what we think is important instead of just listening attentively and following where the patient is taking us. He will always take us where the treasure is hidden. Once the homeopath has defined the territory, only then he is entitled to dig! Then he knows where the Vital sensation is. He doesn’t know what it is, but he knows where to find it. At that point the homeopath can ask to clarify some specific words or statements of the patient. And always, be it in the beginning or at the end of the consultation, question should be as open ended as possible! (like: can you tell more about…, what do you mean by…, how is it?) It makes case taking exciting again, because we adapt to the patient, taking his personality into account. It doesn’t make sense to stubbornly refuse to ask questions in the beginning of the interview, when the patient is so shy and doesn’t know what to say. The non-interference is meant for patients who spontaneously tell their story. In all cases, we try to make the patient feel at ease.
After having spent some time with the patient, his state will become clear. It will pervade his words, behavior and actions. And the expressions, on different levels will always form a coherent pattern. By this pattern we can understand it all comes from one source, which is the vital disturbance. So even if we didn’t ‘get at’ the vital level, we can make a vital level or sensation level prescription. How’s that for good news?
More information and articles about the Vital Approach can be found at:



DEAR DR,
THE THEORY OF HOMEOPATHY IS DIFFERENT FROM ITS PRACTICE. WE SHOULD NOT INSIST ON FOLLOWING THE CLASSICAL METHOD. WE HAVE TO CURE THE PATIENT MAY IT BE CLASSICAL OR MODERN METHOD. TRIAL METHODS MAKE HOMEOPATHY UNPOPULAR. I THINK COMBINATION OR ALTERNATION OF REMEDIES ARE SOME TIME NECESSARY EARLY AND COMPLETE CURE.
THANKS
DR SHEKHAR