The homeopathic repertory is a very important instrument, but still an instrument. It is not possible to prescribe successfully without knowledge or consulting of the materia medica. The Repertory is about knowledge from the past, but the patient before you is another person than the numerous anonymous patients responsible for the data in the repertory. There are so many things that we don’t know about the Repertory, like: what is the meaning of ‘Herpes about lips’? Is this once a year, or ten times a year? It will make a difference if it is ten times a year. And, if you made the repertorisation with, say, eight symptoms, do you prescribe the first remedy? Many times you won’t, and maybe you take the last remedy, because seeing this suggestion you suddenly perceive that the patient perfectly suits that medicine for reasons that were not in the repertorisation.
We might look at a repertorisation like a weather forecast; there are numerous other variables that influence what you are going to do the next day. But still, you want the weather forecast to be correct. Sadly enough, the repertory is not correct. Over two centuries thousands of cases have been reported and the homeopathic database has grown correspondingly. The data were recorded in the homeopathic materia medica and the homeopathic repertory. As the database grew we lost sight and grip on the prerequisites for entering information into the materia medica and the repertory. As a general rule a symptom or characteristic is entered in the materia medica if it is seen in a patient responding well to a specific medicine, and the medicine is entered in the corresponding repertory-rubric. Therefore, the entries are based on absolute occurrence. Some medicines are used frequently, others seldom. If a medicine is frequently used any symptom will come up eventually in a patient responding well to that medicine, especially if the symptom is also frequently occurring. This is due to mere chance.
One of the well-known problems of the homeopathic repertory, is that especially larger rubrics are unreliable and that especially frequently used medicines are over-represented. As said, this is due to chance. In this respect the computer becomes a major threat to the reliability of the homeopathic repertory and materia medica. Updating these sources has become very easy and all manufacturers of homeopathic programs for repertories and materia medica advertise the completeness and vast number of data they comprise. As yet there are no generally accepted rules for ascertaining the reliability of our data. Such rules should be clear, unambiguous and reproducible. First we need a sound theoretical ground and then a methodology based on this ground. The most elegant and widely used theory is Bayes’ theorem. If we apply Bayes’ theorem the computer becomes our most valuable companion. We need large amounts of data and systematic gathering of these data.
Bayes theorem
Reverend Thomas Bayes (1702-1761) based his theorem on the law of conditional probability and it is explicitly or implicitly used to update prior beliefs in a particular hypothesis after observations or experiments.[4] The founder of homeopathy, Hahnemann (1755-1843), already based his use of the homeopathic medicine Rhus toxicodendron on his observation that ‘Amelioration from motion’ was a symptom that occurred more frequently in patients responding well to that medicine than in other patients. Based on this experience homeopathic physicians will prefer Rhus toxicodendron (and other medicines related to the same symptom) if the complaints are better from motion. We refer to patients who respond well to a specific medicine as ‘medicine population’, the patients that respond well to Rhus toxicodendron constitute the ‘Rhus toxicodendron population’.
The addition ‘more than in other patients’ is a crucial element in finding ways to select reliable entries for the homeopathic materia medica and repertory. This can be translated into Bayes theorem. This theorem has several expressions, one of them is:
Posterior odds = LR * prior odds
LR = Likelihood Ratio = prevalence in target population / prevalence in remainder of the population
Odds = chance / (1-chance); chance = odds / (1+odds)
The Likelihood Ratio (LR) is always larger than zero. If LR>1 the posterior odds increases; if LR<1 (>0) the posterior odds decreases.
Our specification of LR is derived from diagnostic research. In diagnostic research we test for a diagnosis with a certain test and compare the outcome with a reference (gold) standard.
This process gives an outcome like table 1.
| Illness present | Illness absent | ||
| Test positive | a= True Positives (TP) | b= False Positives (FP) | a+b |
| Test negative | c= False Negatives (FN) | d= True Negatives (TN) | b+d |
| a+c | b+d | a+b+c+d |
Table 1: 2×2 contingency table for assessing diagnostic tests
Bayes formula can be applied repeatedly. After the first positive test, the chance that the diagnosis is correct increases. This posterior chance becomes the prior chance for the next test. This process is called sequential updating.
Algorithm for homeopathy
Bayes’ theorem enables us to formulate an algorithm for homeopathy; experience from the past tells us what to do in new cases. People who respond well on a specific homeopathic medicine, have specific symptoms that distinguish them from other homeopathic medicines. In other words: the prevalence of certain symptoms in the ‘medicine population’ is larger than in the remainder of the population.
To assess the LR of a homeopathic symptom we use the model of diagnostic tests with specification as in table 2.
| Medicine worked | Remainder of population | ||
| Symptom positive | a= True Positives (TP) | b= False Positives (FP) | a+b |
| Symptom negative | c= False Negative (FN) | d= True Negatives (TN) | b+d |
| a+c | b+d | a+b+c+d |
Table 2: 2×2 contingency table for assessing relation between symptom and effect
With Bayes’ formula and sequential updating we can try to describe the decision process in homeopathy. Suppose we have a patient with joint pain and several symptoms and characteristics. The most simple model, is that the belief that one specific medicine could work is updated after a number of sequential informations. We assume that the prior chance that a medicine will work, without any information, is 5%.
| Information | LR | Prior chance medicine A | Posterior chance medicine A |
| Joint pain | 3 | 5% | 13.6% |
| Desire for cold milk | 5 | 13.6% | 44% |
| Wet weather aggravates | 3 | 44% | 70.2% |
| Restlessness | 3 | 70.2% | 87.6% |
Table 3: homeopathic diagnostic model 1; simple sequential updating of chance of effect, regarding only one medicine
Table 3 represents a simplified hypothetical model; we consider one medicine and all information increases sequentially the probability of effect from medicine A. In homeopathic practice all kinds of information could be relevant: complaint, relations to food, modalities (influences on the complaint) and personal characteristics. We assume that all information is mutually independent. Real practice, of course is more complicated, several possible medicines must be compared.
Repertory and LR
To make a comparison with the existing entries of Kent’s repertory we have to translate type (expressing importance of the symptom related to that medicine) into numbers. Such a translation is arbitrary, A cut-off value like LR>1.5 for plain type means that we regard a medicine as indicated if the prevalence of the symptom in the medicine-population is at least 1.5 times larger than in the rest-population. A possible translation from type into LR could be like Table 4:
| Type | LR |
| Plain | 1.5-3.0 |
| Italics | 3.0-6.0 |
| Bold | > 6.0 |
Table 4: Repertory entries translated into LR values
The choice of LR>6 for bold type could be motivated by the opinion of many homeopathic doctors that three good symptoms are enough to prescribe a medicine. Three good symptoms with LR=6 render a combined LR=6*6*6=216. With this combined LR a prior chance of 1% would climb to 69%. With LR=3 we would need 5 symptoms to get the same result. Therefore, LR=3 or entries in italics stand for 5 necessary symptoms to prescribe with confidence. The lower value of LR=1.5 for plain type is rather arbitrary, lower values wouldn’t make much difference for the chance that a medicine could work.
The Committee for Methods and Validation of the Dutch homeopathic doctors association performed prospective research to assess the Likelihood Ratio (LR) of six symptoms regarding homeopathic medicines.
Methods
From June 2004 until December 2007 we conducted an observational study including all consecutive new patients older than two years. Observers were 10 experienced Dutch homeopathic doctors, working as consultants especially for chronic cases. There were no limitations as to disease, the only limitations were the use of single homeopathic medicines and the possibility to evaluate effect. Practices were divided over the Netherlands. Candidates were selected among participants in our materia medica validation project and received a questionnaire in advance, see appendix 1. In the first consensus meeting with the participants the symptoms were defined. Six symptoms were assessed: 1. ‘Diarrhoea from anticipation’, 2. ‘Fear of death’, 3. ‘Grinding teeth during sleep’, 4 ‘Recurrent herpes lips’, 5. ‘Sensitive to injustice’ and 6. ‘Loquacity’. These six symptoms were checked in all patients. Results were recorded for each prescribed medicine, after evaluation according to the Glasgow Homeopathic Hospital Outcome Scale (GHHOS). The use of the GHHOS scale was already trained in the consensus meeting.
Results
In the end 4094 patients were included; 1314 (32.1%) male, 2752 (67.2%) female, 28 (0.7%) missing values. Mean age was 39.62, standard deviation 20.952, range 3 to 95. The male/female ratio by age is shown in figure 5. Females were over-represented between age 20 and 60.
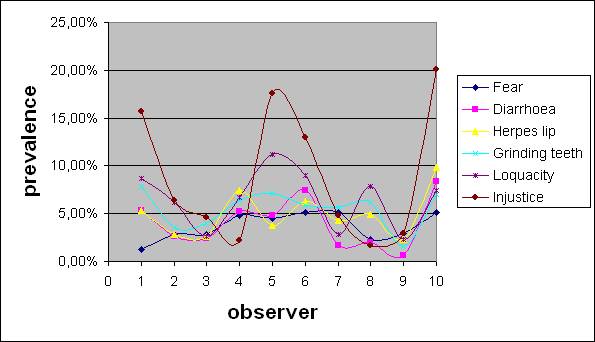
Despite the consensus meeting to define symptoms and feedback on differences between doctors, differences in prevalence of symptoms remained. These differences were most pronounced for the vaguest symptoms, sensitive to injustice and loquacity. See Figure 1.
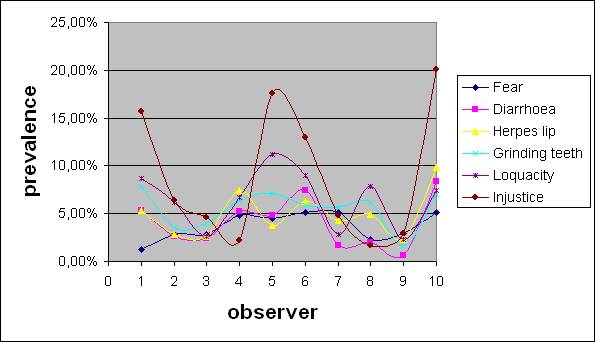
Figure 1: inter-observer variation of prevalence of symptoms
Prescriptions
All together, 421 different medicines were prescribed, but in different frequencies. The 10 most prescribed medicines were responsible for 38% of the successful prescriptions; the 20 most prescribed medicines rendered 53% of the successes. The mean success rate of all prescriptions was 51%. There was no clear difference in success rate between frequently and seldom prescribed medicines. Table 4 shows the most prescribed medicines, their frequency and their success rate.
| Medicine | n | success% |
| nat-m | 248 | 63 |
| Sep | 177 | 53 |
| Sulph | 175 | 50 |
| Lyc | 161 | 53 |
| Calc | 143 | 52 |
| Phos | 127 | 60 |
| Puls | 105 | 56 |
| Merc | 94 | 57 |
| Caust | 88 | 52 |
| Carc | 79 | 54 |
| Staph | 73 | 44 |
| nux-v | 70 | 57 |
| Ign | 67 | 49 |
| Lach | 65 | 65 |
| Sil | 65 | 51 |
| Thuj | 63 | 38 |
| calc-p | 60 | 47 |
| arg-n | 56 | 46 |
| Graph | 54 | 50 |
| nit-ac | 49 | 39 |
Table 4: 20 most prescribed medicines and success percentage
LR values
Calculating LR rendered 48 significant values for LR+ regarding six symptoms. Table 5 shows the results for the symptom ‘Fear of death’.
| LR+ | 95% CI | |||||
| Fear | N=159 | |||||
| acon | 10.6 | 4.87 to 22.93 | ||||
| am-c | 5.8 | 1.69 to 19.87 | ||||
| anac | 11.1 | 5.57 to 22.02 | ||||
| ars | 5.92 | 2.88 to 12.2 | ||||
| cench | 6.49 | 1.18 to 35.67 | ||||
| lac-c | 6.52 | 1.95 to 21.88 | ||||
| naja | 6.49 | 1.18 to 35.67 | ||||
| tab | 8.65 | 1.73 to 43.19 | ||||
| verat | 8.7 | 2.78 to 27.27 | ||||
| zinc | 6.49 | 1.18 to 35.67 | ||||
Table 5: significant LR values for the symptom ‘Fear of death’
There are some medicines where we could not calculate LR for ‘Fear of death’ because no patient had fear of death. With sufficient numbers we can state that it is unlikely that the entries of these medicines in the existing repertory-rubric are correct. We can calculate the chance that LR>1.5, for some medicines this is way below p=0.40. These medicines are Calcarea phosphorica, Medorrhinum, Mercurius and Staphisagria (see table 6).
| Medicine | N | Fear | P |
| calc-p | 28 | 0 | 0.182 |
| Med | 24 | 0 | 0.232 |
| Merc | 54 | 0 | 0.037 |
| Staph | 32 | 0 | 0.143 |
Table 6: medicines probably not indicated by the symptom ‘Fear of death’
What does statistical variance mean for the repertory?
Table 7 shows some results of our research concerning the symptom ‘Fear of death’ as we did formerly using absolute occurrence of symptoms.
| Medicine | Fear of death |
| Acon | 4 |
| arg-n | 2 |
| Ars | 6 |
| Calc | 4 |
| Caust | 2 |
| Gels | 1 |
| Ign | 3 |
| kali-p | 2 |
| lac-c | 2 |
| Lach | 4 |
| Lyc | 4 |
| mag-c | 2 |
| nat-m | 3 |
| nux-v | 2 |
| Phos | 4 |
| Puls | 2 |
| Sep | 6 |
| Sil | 2 |
| Sulph | 1 |
Table 7: the absolute occurrence of the symptom ‘Fear of death’ in patients with good results by various medicines.
According to this table 4 patients with good results on Aconitum had fear of death, a confirmation of the repertory-rubric. All medicines in this table, except Silicea and Magnesia carbonica, are mentioned in the repertory rubric. There seems to be very little difference between the distinctive medicines; Natrium muriaticum seems as much indicated as Aconitum if the patient has a fear of death. Probably many experienced homeopaths will doubt this outcome; experience tells us that fear of death is less related to Natrium muriaticum than to Aconitum. Now let’s look at table 8.
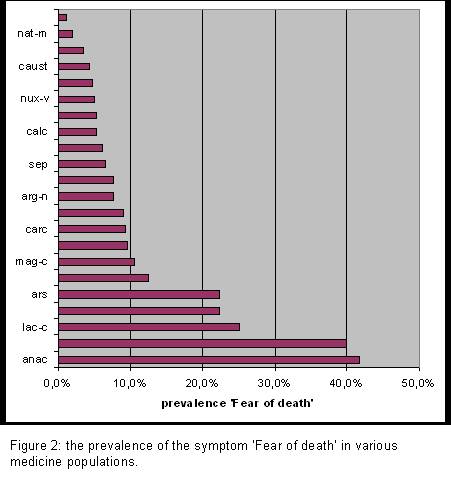
In table 8 we compare the occurrence of the symptom ‘fear of death’ with the total number of patients cured by that medicine, this is the prevalence of this symptom in the respective populations. Now we see much more difference and the results agree more with our experience: The prevalence of fear of death in the population cured by Natrium muriaticum is only 2%, and 40% in the ‘Aconitum population’. If Natrium muriaticum would have been prescribed only ten times, we probably would have seen no natrium muriaticum patients with fear of death.
The graphical representation of table 8 (figure 2) shows the difference more clearly. Considering the graph we would prefer Aconitum over Natrium muriaticum; we would even prefer Silicea over Natrium muriaticum if the patient has a fear of death.
A number of questions come up considering figure 2, like: why should we consider Silicea more than Natrium muriaticum while Natrium muriaticum is in the repertory-rubric and Silicea is not? One could say that the repertory has proven itself over a century, but we all know that there are many mistakes in it. It appears now that there are even systematic failures. So far the entries in the repertory were based on absolute occurrence of symptoms; if the symptom is seen in a case that responded well to the medicine, that medicine is added. We were simply not able to produce the relative occurrence (prevalence) of symptoms because we didn’t record all cases and all symptoms. Our example shows that we should use prevalence and not absolute occurrence.
| medicine | prevalence | Fear of death | total |
| Acon | 40,0% | 4 | 10 |
| arg-n | 7,7% | 2 | 26 |
| Ars | 22,2% | 6 | 27 |
| Calc | 5,3% | 4 | 75 |
| Caust | 4,3% | 2 | 46 |
| Gels | 7,7% | 1 | 13 |
| Ign | 9,1% | 3 | 33 |
| kali-p | 12,5% | 2 | 16 |
| lac-c | 25,0% | 2 | 8 |
| Lach | 9,5% | 4 | 42 |
| Lyc | 4,7% | 4 | 86 |
| mag-c | 10,5% | 2 | 19 |
| nat-m | 1,9% | 3 | 156 |
| nux-v | 5,0% | 2 | 40 |
| Phos | 5,3% | 4 | 76 |
| Puls | 3,4% | 2 | 59 |
| Sep | 6,5% | 6 | 93 |
| Sil | 6,1% | 2 | 33 |
| Sulph | 1,1% | 1 | 88 |
Table 8: the prevalence of the symptom ‘Fear of death’ in patients that had good results from various medicines.
|
|||
A new repertory
We have seen that it is better to use prevalence than absolute occurrence of symptoms. But when should we enter the medicine into the rubric? Intuitively we say “When the prevalence is more than average”, or “When the prevalence is more than in the average of the remainder of the population”. The last expression comes closest to the question if we should prefer a certain medicine over the average other medicine.
An example for the symptom ‘fear of death’, coming from our research:
Prevalence in ‘Aconitum-population’= 4/10; remainder of the population= 154/4084
The ratio between these two prevalences=10.6
Prevalence in ‘Natrium-m-population’=3/156; remainder of the population= 155/3938
The ratio between the two prevalences=0.49
So: Aconitum should be prefered over other medicines, and Natrium muriaticum should not be preferred over other medicines in a case with fear of death.
To show the difference between the old repertory, suppose that you consider to prescribe Natrium muriaticum for a patient with a certainty of 50% and then it appears that the patient has a considerable fear of death.
Old repertory: Natrium muriaticum is in the rubric, so your expected chance that this remedy will work increases (from 50% to 60%?).
New repertory: LR for Natrium muriaticum = 0.49, so your expected chance decreases from 50% to 33%.
Conclusion
Three years of research rendered 121 relevant results: 48 significant values for LR, 73 other values with sufficient probability to validate repertory-entries. Our results differ in 75% of 99 medicine-entries regarding 5 rubrics (excluding ‘sensitive to injustice’) in the original repertory, but if we disregard upgrading or downgrading of entries 56% of the medicines are unjustly entered in these 5 repertory-rubrics or missing from it. For these 5 rubrics 21 results suggest removal and 34 adding of medicines. Most additions are to the smaller rubrics, most removals are from the larger rubrics. These figures represent only 5 symptom-rubrics. We need to assess much more symptoms before we can make a statement about the correctness of the existing repertory.
Our results confirm that the reliability of the repertory can be improved. The application of a sound statistical theory like Bayes’ provides clear criteria, but also increases the scientific basis of homeopathy. However, we must still realise that the repertory is just an instrument like a weather forecast. You like it to be correct but many other variables and intuition will influence which medicine you prescribe.
The doctors participating in this research were Rob Barthels, Hetty Buitelaar, Paul Fruijtier, Gerard Jansen, Jean Pierre Jansen, Stan Jesmiatka, Christien Klein, Roland Lugten, René van der Reijden, Lex Rutten, Erik Stolper, Janny Verhey and Mechtild Wijdeveld.
For further reference read:
Stolper CF, Rutten ALB, Lugten RFG, Barthels RJWMM. Improving homeopathic prescribing by applying epidemiological techniques: the role of likelihood ratio. Homeopathy 2002;91:230-238
Rutten ALB., Stolper CF, Lugten RF, Barthels RJ. Is assessment of likelihood ratio of homeopathic symptoms possible? A pilot study. Homeopathy. 2003;92:213-216.
Rutten ALB., Stolper CF, Lugten RF, Barthels RJ. Assessing likelihood ratio of clinical symptoms: handling vagueness. Homeopathy. 2003;92:182-186.
Rutten ALB, Stolper CF, Lugten RF, Barthels RJ. ‘Cure’ as the gold standard for likelihood ratio assessment: theoretical considerations. Homeopathy 2004;93:78-83
Rutten ALB., Stolper CF, Lugten RF, Barthels RJ. Repertory and likelihood ratio: time for structural changes. Homeopathy. 2004;93:120-124.
Rutten ALB., Stolper CF, Lugten RF, Barthels RJ. Repertory and the symptom loquacity: some results from a pilot-study. Homeopathy. 2004;93:.190-192
Rutten ALB., Stolper CF, Lugten RF, Barthels RJ. A Bayesian perspective on the reliability of homeopathic repertories. Homeopathy. 2006;95:88-93
Rutten ALB. Bayesian homeopathy: talking normal again. Homeopathy. 2007;96:120-124
Rutten ALB., Stolper CF, Lugten RF, Barthels RJ. New repertory, new considerations. Homeopathy 2008;97:16-21
Rutten ALB. How can we change beliefs? A Bayesian perspective. Homeopathy 2008;97:214-219
Rutten ALB., Stolper CF, Lugten RF, Barthels RJ. Statistical analysis of six repertory-rubrics after prospective assessment applying Bayes’ theorem. Homeopathy 2009;98:26-34.
Rutten ALB. Improving homeopathic practice using Bayes’ theorem and likelihood ratio. J Altern Med Res 2009;1(1):
Wassenhoven M van. Towards an evidence-based repertory: clinical evaluation of Veratrum album. Homeopathy 2004;93:71-77