What Kind Of Repertory Does The Veterinarian Need?
If we compare veterinary work to that of the practitioners on human beings, we see that the perspective is, by necessity, different. In the work with human beings, this information is important to determine, and as completely as possible:
- Symptom
- Location
- Sensation
- Time of occurrence
- Periodicity
- Extension of symptom (to other parts)
- Amelioration
- Aggravation
- Accompanying symptoms (concomitants)
- Etiology
- Emotional state
- Mental functioning
We veterinarians work with a modified list:
- Symptom (sometimes observable but often reported by client, therefore interpreted)
- Location (sometimes apparent, but often not definable)
- Sensation (occasionally can be guessed at but not reliably known)
- Time of occurrence (limited to the waking or visiting hours of the client)
- Periodicity (if the client observant enough)
- Extension (subject to same limitations above)
- Amelioration (often available though not necessarily in a useful form—as in what drugs relieve)
- Aggravation (often available but subject to assumption and projection of the client)
- Accompanying symptoms (usually obtainable, though limited by client’s memory)
- Etiology (sometimes known, often speculated)
- Emotional state (with broad interpretation, often misunderstood)
- Mental functioning (difficult to assess unless grossly malfunctioning)
So, as veterinarians, we have very limited information which is often reduced to common symptoms and pathology, especially if the animal has been ill very long and already had extensive suppressive allopathic treatment. The mental symptoms, so important in human prescribing, are marginally useful but may not be clearly defined. A state such as “anxiety” has so many remedies in the appropriate rubric that it becomes basically useless. What we find most helpful and most reliable are physical symptoms as modified by modalities. If this is coupled with concomitants the information may be enough to find a similimum even in chronic and difficult cases. The repertories designed for human use, often emphasize those aspects which are not available to us. It is not that the information is not in the materia medica, but rather was not entered into the repertory. In this talk we will consider a few of the major repertories, how they were developed by the authors and how applicable they are to veterinary work.
What Is The Purpose Of A Repertory?
Our first question is basic. Why do we use a repertory? Let me answer this by quoting from Jahr’s preface to his book, Therapeutic Guide: The Most Important Results Of More Than Forty Years Practice. “It was in the year 1827 when I made my debut in the practice of homeopathy, at a time when the only resources at our command were the Materia Medica Pura…and a few cures reported. With these scanty means we had to get along as well as we could, and, by a diligent and attentive study of the drugs with whose pathogeneses we had become acquainted with at that time, familiarize ourselves with the characteristic symptoms of each drug and its special indications…. This was no small task, which could never have been accomplished, if the Materia Medica of that time had contained the large number of drugs that are offered at the present time to the beginner in homeopathic practice. Since the number of drugs known at that time did not exceed 60, and among these only 20 had been proved with exhaustive perseverance and correctness, we had it in our power to study them thoroughly without too much trouble…and apply them as such in accordance with their symptomatic indications. At this time such a careful study of our Materia medica is unfortunately not possible to the beginner in homeopathy. Overwhelmed by the accumulated mass of drugs and clinical observations, he scarcely knows which way to turn for at least one ray of light in the chaos spread out before him.”
Jahr’s Problem Relevant Today
Here we see the problem well described—that it is beyond our means to memorize the large mass of data available to us now. A repertory thus organizes information for us. It is a decided advantage to look up a symptom of interest and find listed the several remedies known to display this symptom in provings. In addition, Boenninghausen, in his repertory development, introduced the idea of grading remedies. This he did in 1832, with the production of his first repertory, The Repertory of the Anti-psoric Remedies, and brought a new tool into development for our use. We can often match the grading of the remedy with the intensity of the symptom in the patient, thus honing in more accurately to what the patient requires.
Thus, we have two advantages with a repertory:
- A rubric (symptom) lists all the remedies known to produce that symptom.
- The grading of remedies indicates those which have the symptom most frequently or prominently.
The Development of Repertories
Repertories have gone through an evolutionary development, along with the general progress of homeopathy as a science. With repertory use we have learned what remedies are polychrests and also which remedies are most suitable for treating chronic diseases. On the clinical side, we have correlated the repertory information with what is seen in patients. We have learned how to accurately translate the language of the proving into the language of the sick patient. We can say that over the 200 years we have been using homeopathy we have sifted out the information that is of most use to us in our work. The repertories will reflect this, as they are compilations, extractions, of the more complete, but less organized, information in the materia medica. Though the repertories were developed along certain lines, recent expansions of these works have, to some extent, changed the original purpose in their construction and use.
How Were Repertories Created?
How is a repertory constructed? We start with the information from a proving. If that information was simply listed, as a complete symptom, then the repertory becomes cumbersome and of no further use to us than a materia medica. A good example of this approach is Knerr’s Repertory of Hering’s Guiding Symptoms of Our Materia Medica. This is a complete repertory but very difficult to use. Symptoms are kept intact as, for example:
Extremities; KNEES; abscess; small opening over patella, oozing laudable pus, later
profuse, yellow,
serous discharge, particularly early in evening: Iodium
Extremities; KNEES; pain; flexors of left, in, extending
around thigh, immediately above patella, as if
limb were severely grasped: chim. (chimophila)
Extremities; KNEES; rheumatism; inflammatory,
sore to touch, redness, followed by effusion, patella
being lifted up, with elastic swelling underneath and
around: stict. (sticta)
This is all very detailed information and of great use in clearly defining a symptom – but very slow for the process of evaluation and with much reading required.
Another Approach
The other way of processing this information is to break it up and put it in different places in the repertory. Instead of all the information in one long line, we enter each part in a different place in the repertory. When it comes time to work up a patient’s case then what we are attempting to do is to reconstruct the patient’s condition by re-assembling the information found in the repertory into a description that approximates it as much as possible.
How Complete Are The Repertories?
How well do the repertories reflect the information of the materia medica? Not as much as you would expect. Let’s look at a proving of Apis as an example. Using Allen’s Encyclopedia, General Section, which describes the provings symptoms, we can certainly find interesting and useful symptoms. Here is one.
(From effects of a sting) She was found to be in a spasm, generally tonic, but in a measure clonic; her knees were drawn up to her breast, and her hands and arms moved convulsively. Convulsions. The whole nervous system seemed most violently affected.
Now let’s see what we can find in Kent’s Repertory:
She was found to be in a spasm, generally tonic, but in a measure clonic = there is no rubric in Kent for spasms. Closest is “Convulsions, tonic” (83 remedies) in which
Apis is found in lowest grade. The rubric “Convulsions, clonic” (118 remedies) does not contain Apis.
Her knees were drawn up to her breast = not found in Kent.
In the Complete Repertory, we find these equivalent rubrics, but no Apis:
- Generalities; LYING; Amel.; during; legs drawn up (7): bell., cocc., coloc., gent-l., Magp., stram., verat.
- Generalities; LYING; Amel.; during; knee; chest position (2): choc., sep.
Her hands and arms moved convulsively = Kent has
“Generalities, convulsive movements” (73 remedies) with Apis in lowest grade. The rubrics “Convulsion, upper limbs” (45 remedies) and “Convulsion, hands” (31 remedies) do not contain Apis. However, we do find Apis, in lowest grade, here, in these two rubrics.
- Extremities; MOTION.; Upper Limbs; convulsive (15)
- Extremities; MOTION.; Hands; convulsive (7)
So we can see that Kent had to make a decision. Where to put this Apis proving information? It is indeed accurate to list it in the last two rubrics mentioned here, but why not under “Extremities, convulsions”? One could easily look there first, not see the remedy and miss it in a case. Unless you thought of the word “Motion” first instead of spams for convulsions, you could not get to it.
There are several other symptoms, ones we could recognize in animals, that are not accurately found in the repertory. Examples are:
Terrified starting during evening sleep. = only relevant rubric, though not containing Apis, is:
- Sleep; SLEEPLESSNESS; evening; starting, from (1): puls.
A close rubric is:
- Sleep; SLEEPLESSNESS; anxiety, from (21): arn., Arsenicum, bell., bry., carb-an., caust., Cocc., cupr., kali-i., laur., lyss., mag-c., mag-m., merc., nat-c., nat-m., nux v., rhus-t., stram., sulph., thuj.
There is no rubric about sleep issues from fear.
Another one has to do with restlessness, a characteristic of this remedy, Apis. We see this in the proving:
Restlessness; would constantly like to go from one
place to another. An extraordinary restlessness overcomes
him in the afternoon, with as much exhaustion
as if he had done very hard, manual labor. (After smelling the bee poison, when gathering a swarm).
Nervous restlessness. Nervous restlessness, during the latter half of the night.
Kent’s Repertory, no Apis in any of these rubrics.
- Mind; RESTLESSNESS; anxious, etc.; compelling rapid walking (5): arg-n., Arsenicum, lil-t., sul-ac., Tarent.
- Mind; RESTLESSNESS; pacing back and forwards (1): plan.
- Mind; RESTLESSNESS; sitting, while (12): alum., cact., caust., ferr., iod., Lycopodium, mag-c., nat-m., plan., sep., sil., sulph.
- Mind; RESTLESSNESS; walking amel. (3): dios., nat-m., nicc.
- Generalities; MOTION; amel. (119 remedies)
- Generalities; MOTION; continued, amel. (37 remedies).
Apis is found here:
- Generalities; WALKING; amel. (113), Apis in lowest grade.
- Generalities; WALKING; fast agg. (65), Apis found in second grade, which is only confusing in regard to this symptom.
As for the exhaustion as if very hard, manual labor, Kent does not have any rubric for “Exhaustion”, the closest being “Generalities, weariness”. Apis is not there.
In regard to the restlessness at night, Apis appears in this rubric, second grade:
- Mind; RESTLESSNESS; night (169 remedies)
but not in this rubric, which is more definitive:
- Mind; RESTLESSNESS; midnight; after (9)
General feeling of lassitude, with trembling. = no such rubric in Kent’s.
During continual diarrhoea, weakness increases, and headache diminishes. = there is no rubric for “continued diarrhea” or for “chronic diarrhea” in Kents. There is no rubric for “diarrhea with weakness”.
We do find, under Generalities, this one:
- Generalities; WEAKNESS,; diarrhoea, from (46)
which contains Apis in second grade. What may be misleading here is the idea that the weakness is caused by the diarrhea instead of being a concomitant. There are several symptoms having to do with the serious clinical problem of prostration, the patient being so ill they are lying flat out (or must lie down) and cannot stand or walk. It is seen in very serious infectious diseases, toxic conditions, near death states.
Sudden prostration, with coldness.
Sudden prostration of the vital forces; severe vomiting; profuse diarrhoea; cold extremities; pale face; severe griping pains in the abdomen; pulse weak, scarcely perceptible at the wrist.
Heavy and prostrate in fever.
Was obliged to be led into the house; threw himself on the bed; unable to hold himself up.
Without feeling either weakness or faintness, she is yet suddenly compelled to lie down on the ground.
Sinks quite exhausted at stool.
There is no rubric for “Prostration” in Kent’s. The closest is under Generalities, “Collapse” (44 remedies) in which we find Apis as lowest grade. Apis is not in the subrubric, “Collapse, sudden”.
There are these rubrics:
- Generalities; COLLAPSE; vomiting, during (1): ars.
- Generalities; COLLAPSE; vomiting, after (4): Arsenicum, lob., phys., verat.
But no Apis. Nothing about collapse with a weak pulse, or cold extremities, pale face, with abdominal pains, or with fever. No rubrics for suddenly having to lie down or exhaustion after a stool. There is
- Generalities, weakness after stool (60 remedies)
in which Apis is the lowest grade.
So we see from this short perusal, that the repertory does not have anything like a complete listing of symptoms from provings.
Repertory Overload
Well then, why not put all this information into a more complete repertory? This is the contemporary trend, especially with Synthesis and The Complete repertories. These are expanding on Kent’s repertory and pulling in information from Boenninghausen, as well as other repertories, provings, clinical studies and many other sources. Is this what we need? These larger repertories can be extremely useful for finding unusual or detailed symptoms but they have these disadvantages:
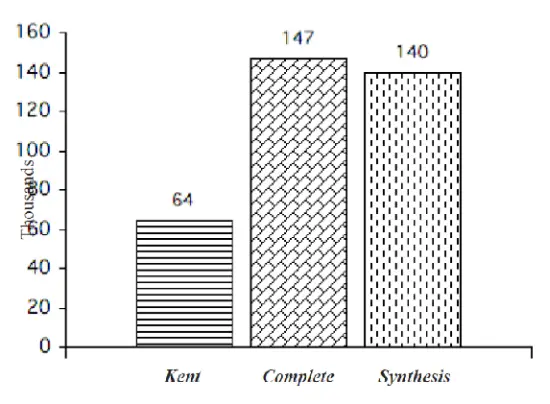
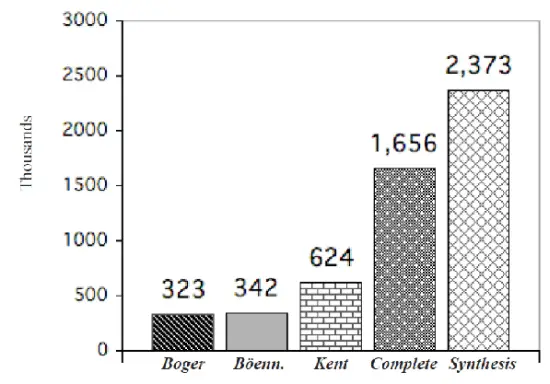
The number of rubrics is increased. There is much more material to look through when trying to find the common symptoms. The number of remedies in each rubric has also increased (see graph below). This results in many more for consideration in our final analysis than with the previous repertories. On a practical note, as the books become larger, physically, they become unwieldy, and too difficult to use. We experience information overload—too much of a good thing.
Comparison of Rubric Number
 Repertory Remedy Numbers
Repertory Remedy Numbers
How The Repertories Affect Case Analysis
Here is an example analysis, a common situation for us, showing us how a large repertory can overwhelm us with possibilities.
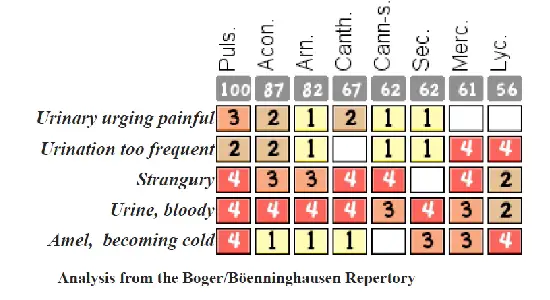
A young cat has developed a urinary condition, going frequently to the litter box, straining, licking the penis after urinating. The urine is yellow with occasional blood. Behavior change is not marked, though not as affectionate and seems anxious. The oddest behavior is that the cat will often go into the bathtub and sit there when having this problem.
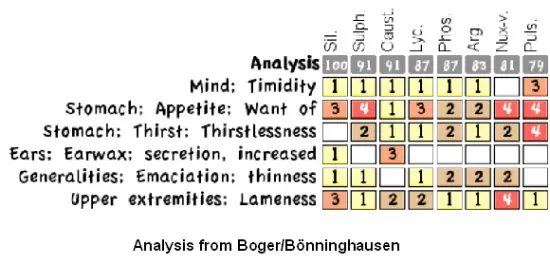
That the cat is going into the cool bathtub for relief tells us this is likely a Pulsatilla case. Let’s do a repertory workup using the Boger/Boenninghausen Repertory and compare it to that of the Complete Repertory.
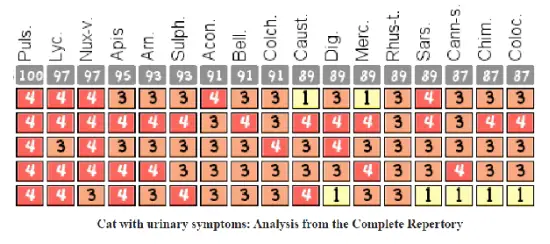 Now compare this analysis, which easily suggests Pulsatilla, to one from the Complete Repertory using the same rubrics (see next page). We see that the larger repertory, with more remedies in the rubrics, will simply give us too much information. Who would really have time to consider each one of these that come up in the Complete analysis? Would it not be of more use to us to have a repertory that will suggest the most likely remedy (as opposed to striving for completeness)? This is the plan of repertories like Jahr and Boger/Boenninghausen. Instead of attempting to have every possible remedy entered in each rubric, we can limit the rubrics to just those that are most frequently (most likely) needed. This gives us much more manageable rubrics, while at the same time maximizing our chance of finding the similimum. However, to do this accurately we must use a particular strategy. Before discussing analysis strategies, let’s next look at the different repertories and how they are designed.
Now compare this analysis, which easily suggests Pulsatilla, to one from the Complete Repertory using the same rubrics (see next page). We see that the larger repertory, with more remedies in the rubrics, will simply give us too much information. Who would really have time to consider each one of these that come up in the Complete analysis? Would it not be of more use to us to have a repertory that will suggest the most likely remedy (as opposed to striving for completeness)? This is the plan of repertories like Jahr and Boger/Boenninghausen. Instead of attempting to have every possible remedy entered in each rubric, we can limit the rubrics to just those that are most frequently (most likely) needed. This gives us much more manageable rubrics, while at the same time maximizing our chance of finding the similimum. However, to do this accurately we must use a particular strategy. Before discussing analysis strategies, let’s next look at the different repertories and how they are designed.
How Repertories Are Planned
Let’s take a look at the strategies authors have used in developing repertories. They are not all the same. For one thing we have had an accumulating body of information that tells us what are the most commonly needed remedies. From this base I identify 3 approaches used in repertory construction.
The Kent Method
From The Development and Formation of the Repertory, by James Tyler Kent. “Not so many years after I was first a homoeopath, there fell into my hands the first Boenninghausen’s Repertory, Lippe’s Repertory, Biegler’s Diary, Minton’s Diseases of Women, and Jahr’s Repertory, which in form was very good. And Lippe’s Repertory, in characteristics and form was very good. I carried Lippe’s Repertory with me for a number of years, until it was not only interleaved but doubly and trebly interleaved, the pages so closely written upon that it was impossible to find what I had written into it; so that ended in confusion. But this was the one upon which my earlier reliance rested. “Then came the time, when I began to teach Materia Medica, in 1883, when I could readily see that we ought to have more. The Symptom-Register
(Allen’s great Encyclopædia), was so limited that it lacked half of the symptoms. Jahr’s Repertory was placed next in importance because it was a repertory of the grand old remedies, It was very good for these, but our pathogenesis had increased so much that it was no longer a satisfactory work ; it did not fill the requirements of my practice. So I began taking up these works and effecting a compilation. Eventually I had a large manuscript of most of the repertory. “I talked with Lee, of Philadelphia, as Lippe’s abridged form of a new repertory was in his hands and Lippe desired me to enter upon the work of helping or uniting with Lee to produce a complete repertory. At that time I had completed a Repertory of the Urinary Organs, of Chill, Fever and Sweat, with other sections partly complete. Lee went to work and got out Mind, and later I helped him to get out Head….” From this beginning the great work that was Kent’s Repertory was developed (1897). As we see, from a compilation of many sources. Yet, it was still not complete enough. From David Warkentin, Kent Homeopathic Associates– Most homeopaths have assumed that Kent contains virtually all of the reliable symptoms. This is far from true. First of all, the task of creating a comprehensive repertory is a huge one and probably impossible. For example, even though Kent intended to add Allen’s Symptom-Register into his repertory, he was only able to add a minority of the rubrics. (Allen’s work is still larger than Kent’s.) And secondly, Kent was in competition with other repertory authors, notably Knerr and Boger, and did not share information with them.
The Kent Plan of Analysis
In Kent we have an emphasis on general and mental symptoms. We use a hierarchy of classification to organize our symptoms in order of importance. The Kent strategy is 3-fold:
- Start with the general condition of the patient. This is what is predicated to the patient as a whole, along with modalities that affect these symptoms.
- We look for and emphasize the mental condition, using this to further characterize our patient.
- We combine particular symptoms to create ones that are characteristic.
- The similimum must fit the general and mental symptoms of the patient yet may not have all the particulars of the case.
Kent decided that, besides the symptoms that are obviously general, we should emphasize also the reproductive symptoms of women and also the details of various discharges. That is, in his plan he elevates these conditions to the level of general symptoms. He bases this on his clinical experience and the conclusion that it is the individuality of the patient that determines this. Hahnemann had emphasized the importance of the mental state and Kent also brought this in as highly important whenever that information is available. He also organized information from the patient into symptoms that would be characteristic by bringing two of them together. For example, our patient could have diarrhea which is common, but having it every morning at 6 AM made it characteristic. In a way, he was reconstructing the patient’s symptoms from the repertory but in a way that made the information more useful. This was a use of Hahnemann’s advice to look for what was “unusual, rare and peculiar”. Lastly, he knew that the remedy, if it matched the essentials of the case could address particular conditions even if they had never been known before to be an expression of that remedy. It was the “general” match that was essential.
The Boenninghausen Repertory
The Repertory of the Antipsoric Remedies was created in 1833 by Boenninghausen and was the repertory that Hahnemann used in his practice. In 1846 Boenninghausen deleted and combined many of the rubrics to create a small concise pocket version: The Therapeutic Pocketbook. The Pocketbook became the standard reference work used by most American homeopaths including Stuart Close, Carroll Dunham, Guernsey, and T. F. Allen.
Boenninghausen created his repertory based on the results of his detailed and careful investigations of both provers and patients in regard to the information they reported. He found that, in both cases, most symptoms were incomplete in terms of containing all the desired information. We want, for example, the location, sensation, functional changes, conditions of aggravation and amelioration, and the concomitants. Yet very few provers or patients were able to give symptoms in this complete form.
From The Art Of The Homeopath In Taking The Case In C. Von Boenninghausen’s Work: “Noting these deficiencies in the Materia Medica, therefore, and realizing the importance of these auxiliary modifying and concomitant symptoms of disease, C. von Boenninghausen for many years diligently observed and collected all such symptoms as they appeared in the cases which came to him for treatment. Every case was examined symptomatically with this purpose always in view, to make every symptom as complete in itself as possible, covering the specific points of locality, sensation, conditions of aggravation and amelioration, and the concomitance or coexistence of other symptoms under the same circumstances.
“He soon learned that symptoms which existed in an incomplete state in some part of a given case could be reliably completed by analogy, by observing the conditions of other parts of the case. If, for instance, it was not possible by questioning a patient to decide what aggravated or ameliorated a particular symptom of the case, the patient would readily express a condition of amelioration of some other symptom.
“In reality the patient is not expressing many symptoms, but only parts of a very few complete symptoms, which the homeopath must bring together and complete. The perceptible symptoms of disease are often broken up and scattered through the different parts of a patient’s organism. The scattered parts must be found and brought together in harmonious relation according to the typical form.
“C. von Boenninghausen tells us in his Preface, From one point of view the indicated conditions of aggravation or amelioration have a far more significant relation to the totality of the case and to its single symptoms than is usually supposed; they are never confined exclusively to one or another symptom, but on the contrary, a correct choice of the suitable remedy depends very often chiefly upon them.
“In reality, then, they are the general characteristics. By observing them and applying this principle he was enabled to complete many symptoms from clinical observation; and experience has borne out the truth and reliability of his method.
So what Boenninghausen found was:
- Symptoms from provings could be completed from the observation of these same symptom fragments in patients.
- The modalities—conditions of aggravation or amelioration—have the status of general characteristics because they apply to all of the patient’s symptoms. (Of course, there will be exceptions.)
- Emphasizing the modalities and concomitants will often solve a case.
In addition, his strategy was to:
- Find what is characteristic of the patient by emphasizing modalities and concomitants.
- Generalize symptoms in the patient, even those affecting parts.
- Minimize use of the mental symptoms, as being difficult of accurate interpretation.
The Cyrus Maxwell Boger’s Edition Of The Boenninghausen Repertory
Thirty five years later, in 1899, Cyrus Boger made a new translation of the original Repertory of the Antipsoric Remedies into English. It was 232 pages. He continued to enlarge it until his death in 1935. He added so many additions and new rubrics that ist final size was almost five times bigger: 1040 pages. It is probably more correct to call this “Boger’s Repertory” than “Boenninghausen’s”.
David Warkentin: “This is the one of most valuable repertories ever created. Much of the information is more up to date than Kent’s and it contains many rubrics that aren’t included in Kent.”
From Rubrics In (Boger-) Boenninghausen Not In Kent, by Elizabeth Wright Hubbard, MD (Journal of the American Institute of Homeopathy, August, 1956. Vol. 49, No. 7, pages 203-206):
“Boenninghausen’s is most factual and classified: every symptom that refers to a part may be predicated of the whole. The interrelationship of symptoms and of remedies and the sequence of remedies are brought out. It opens a way into the wide fields of combinations. For Boenninghausen, the totality is made up of the general characteristics of the particular symptoms plus the condition, under the four general categories of locality, sensation, modality (aggravations or ameliorations) and concomitants.
“Roberts in his brilliant Principles and Practicability of Boenninghausen’s Therapeutic Pocket Book says it is based on the doctrine of concomitants, a concomitant being an attendant circumstance existing or occurring with other symptoms, having always a relation in time. The concomitant is the differentiating factor.
“Hahnemann says that ‘the characteristic symptoms represent that which is curable in each case of disease,’ in other words the common symptoms of the diagnosis do
not point the way to cure. Boenninghausen called chronic symptoms concomitants in acute ailments and often prescribed exclusively on them, although a drug should be findable covering both acute and chronic.
“The Boenninghausen method shines in cases without many mental symptoms; without rare, strange and peculiar symptoms; with few particulars; in cases where modalities predominate and concomitants are marked; cases showing pathological symptoms and objective symptoms.” That is, a very useful repertory for veterinarians.
Jahr’s And Boger’s Repertories
Jahr’s work was at the same time as Boenninghausen, but he emphasized (I believe) the known remedies as confirmed by clinical experience. In his book 40 Years Practice we see his emphasis on using what he was able to confirm himself. He developed rubrics that were smaller, yet contained the chief remedies for each symptom. The idea is to limit the rubrics to a usable size, yet make the accuracy of the rubric (in terms of containing the needed remedy) as high as possible. Thus we will see rubrics that are much smaller but ones that are developed from clinical experience.
Boger took a similar approach in his Synoptic Key. For example, if we take a common symptom, like fever, we find that in the Synoptic Key is listed 27 remedies. Compare this to the Complete Repertory where there are 700 remedies listed for the same rubric. Your first reaction may be that Boger is very limited and is therefore useless. But what if fever was very prominent in your patient and there was a 99% probability that the remedy needed was in this list of 27? You can see immediately the practical advantage to keeping the rubrics small and accurate.
These are the types of decisions that determine the plan of repertory construction, which in turn influences the size of the rubrics. Boger chose to be concise, to avoid excessive information while retaining a high degree of accuracy. This approach is very useful to veterinarians.
How Cases Are Worked
Let’s look at how the various repertories will work out cases. As these repertories were designed to be used with human beings, let’s start with a human case. Then we can compare that with animal cases to see what the differences are. From Harvey Farrington, described in his book Homeopathy and Homeopathic Prescribing, 1955—
This is the authentic history of a young woman of twenty, who contracted malaria while traveling with her family in Italy. Massive doses of quinine, prescribed by an Italian physician, stopped the chills and she was able to continue her tour. Not long after her return home she required a dose of Bromine, her constitutional remedy. Later, whether from the action of the Bromine or otherwise, the chills reappeared. Arsenicum alb. was prescribed by a local homeopath without result. The symptoms became alarming, and he gave quinine in massive doses, this time with only temporary palliative effect.
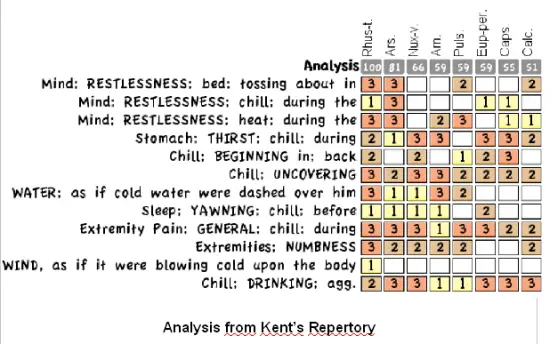
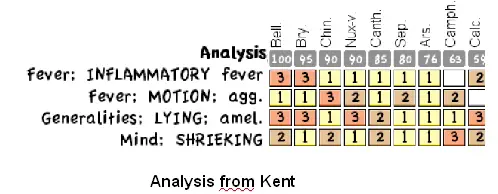
In prescribing for malarial patients homeopathically, the exact similimum must be found if a cure is to be expected. Since Arsenicum had been prescribed by a man of many years’ experience, and the case presented a number of Arsenicum indications, the physician who was called at this juncture worked the case out with great care, using Kent’s Repertory.
The symptoms were as follows: Chill daily at 6 or 6: 30 p. m.; beginning between the scapulae, as though ice water were dashed down the back; preceded by faintness and yawning; accompanied by intense thirst, great restlessness with tossing about, coldness, numbness and aching of the extremities, cold buttocks, and a sensation as though a wind blew on the feet and legs. The chill was worse from drinking cold water and from the least movement under the covers.
Fever without thirst was accompanied by throbbing headache, faintness, nausea, moaning, oppression of the chest, gasping and restlessness. The face was flushed, the skin hot and dry, and there was chilliness from lifting the covers. The temperature during the heat rose to 104. 5 F. Restlessness was the most marked mental characteristic; therefore, it was given first place in the repertory study.
Farrington used Kent’s repertory with these rubrics (see below). A single dose of Rhus tox. was given. For three days there was no change. Then the chill was lighter and the fever not so high and there was less aching of the limbs. The next day there was only a slight chill in the evening, and from then on the symptoms gradually abated. The patient’s general condition improved and by the sixth day all symptoms had disappeared, and years have elapsed with no return.
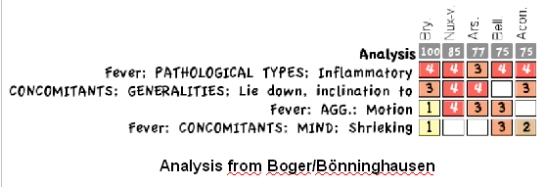
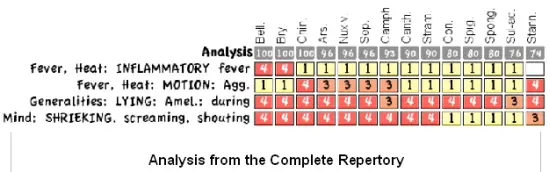
Let us compare how the analysis would have gone with the Boenninghausen repertory.
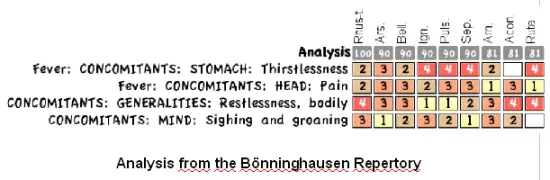
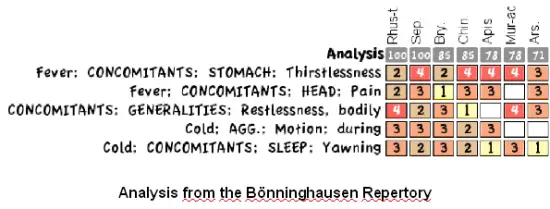
We see that the analysis, using concomitants, can be much simpler, much more focused. Here is another analysis from Boenninghausen. This next analysis introduces a modality along with concomitants and with same result.
For comparison, let us look at a simple analysis using Boger’s Synoptic Key Repertory.
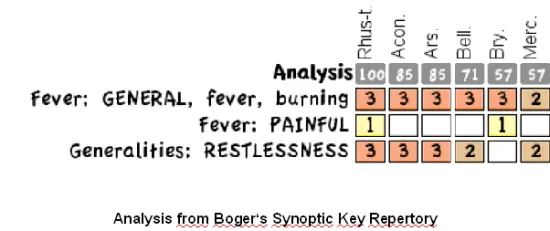
We see that it is possible to come to the same remedy using different approaches, yet with different degrees of efficiency.
An Animal Case
Moses, a 5 year old male cat, has become recently ill. He is very lethargic and completely lost his appetite. If made to stand he cries out. He has not moved for 24 hours. There is a fever going from 103.5 F. (39.7 C) to 105 F. (40.6 C). Blood analysis shows a normal WBC count, normal neutrophil levels but very low lymphocyte and monocyte numbers—suggesting a marked migration of these cells to some extravascular site. These values are also elevated:
SGOT, CPK (very high), direct bilirubin, & blood glucose. The SGPT is normal as are BUN and Creatinine.
Bryonia 30c, one pellet, was given every 4 hours for 4 doses. He recovered over the next 2 days and was completely normal afterwards. He remained free of illness over the next 2 weeks, after which contact with him was lost. For comparison, here is the same analysis from Kent:
And from the Complete Repertory:
We see that Bryonia shows up in all the analyses, yet to me, is more easily recognized in the first Boenninghausen analysis.
Animal Case
Star is a 7 months old, female, Harlequin Great Dane. She presents with a history of poor appetite and a thin condition. She is growing quickly but at about the proper rate for this breed. She is shy, doesn’t want touch of strangers. Physically there is limping in the left front leg though no lesion can be found. The ears are excessively waxy, and there is a red, dry, patchy area at the place where the abdomen joins the rear leg, mostly on the left side. Client had already given Arnica 200c for the limp and there was some temporary improvement for 5 days at which point the limp returned.
First Prescription was Phosphorus 10M, one dose.
Three week follow-up: More friendly, not so shy. “Very friendly in society.” Client emphasizes the great increase in energy. Still thin, though appetite all right. Still some ear wax. No limping. No skin lesion at prior location but some redness between the thighs where they rub together. We wait longer.
Seven weeks after first prescription: Client gives a dose of Parvovinum 200c in lieu of vaccination. (I am not sure if this was her idea or mine.)
Eight week follow-up from Phosphorus: Greenish discharge from the inner canthus of both eyes, worse on going in the sun. Back roached. Appetite not good, only “picks” at food. Still not as shy as before. Drinks almost no water. Skin eruption gone. Second Prescription was Pulsatilla 10M, once.
One week after Pulsatilla: Has not eaten for 3 days, a gradual decrease in appetite. Now wants to go off by herself. Acting more “cowardly”. Less eye discharge. She is looking thin.
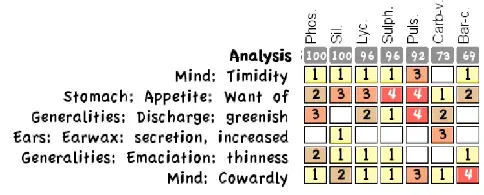
Analysis from Boger/Boenninghausen
Third Prescription was Silica 200c, one dose.
One week follow-up of Silica: She is acting normal and eating well. She became well 3 days after the remedy given. She is slowly gaining weight. All skin irritation and redness is gone. There is no eye discharge. Not very shy now but client can see “there is that tendency”.
Six weeks follow-up: “She looked fantastic.” Skin normal, temperament very good. Sold to Finland and contact with her lost.
It is interesting to compare this complicated case with analysis from a larger repertory. Here it is from the Complete Repertory:
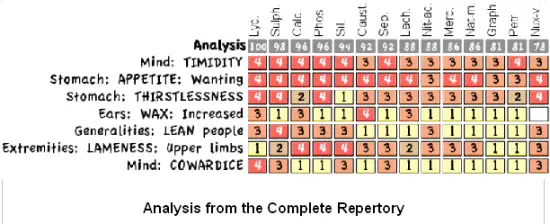
We can see a similar remedy group with this analysis, but many more remedies to consider, thus to my eye, a more complicated workup than is necessary.
Discussion
We can see that all 3 remedies used in this case came up in the first analysis that was done. This was apparently chronic disease, likely inherited, so it took more than one remedy to work through it. This is, of course, not an unusual situation for many of our cases.
What Repertory Then?
I have found the most consistent usefulness, for animal cases, is to start with the Boger/Boenninghausen repertory, at times supplemented by Kent. With unusual symptoms, when I want to search most extensively, I use the Complete Repertory or Synthesis—or just as often ReferenceWorks for a materia medica search.
The advantage of the Boenninghausen method is the emphasis on information we are most likely to obtain with our animal patients—symptoms, yes, but also modalities and concomitants. This method de-emphasizes the mental symptoms (though they are there) in favor of physical conditions as modified by these other factors. In addition, there are some very useful rubrics not found elsewhere.
I also value the repertory by Jahr, which is smaller, simpler, but often adequate. One of my projects is developing the Jahr repertory for veterinary use. I am using this smaller repertory as a base and adding in rubrics from Boenninghausen and Kent to make it a more useful reference for our work. If we streamline the repertory for veterinary use and emphasize modalities and concomitants, a lá Boenninghausen’s method, I think we will have a very useful and unique tool for our work.
References
The charts for comparison of different repertory rubric numbers and remedy numbers is from Roger Van Zandvoort, and compares the Kent repertory (version not specified), the Complete Repertory 4.5 and Synthesis 9.1 (information from Archibel’s website).
Rubrics In Boenninghausen Not In Kent, by Elizabeth Wright Hubbard, MD is from the Journal of the American Institute of Homeopathy, August, 1956. Vol. 49, No. 7, pages 203-206.
Repertories used in my analyses are the Boenninghausen repertory, the Kent repertory, and the Complete Repertory 2005, as provided by Kent Homeopathic Associates with the MacRepertory program.
Analyses shown are configured by calculating both totality and number of rubrics, so that those remedies appearing in the most rubrics and having the highest grading come up first.
www.drpitcairn.com

Hi Dr Pitcairn,
Thanks for your ‘Towards A Veterinary Repertory’ you understant the animals pain.
with reg.
Prof Shaikh Shamsur Rahman
Abu Dhabi
UAE
In my humble opinion we should try to make Kent’s repertory more user friendly by highlighting rubrics verified in animals .This will serve two purpose it’s confirmation on animals and make veterinarian’s search easy .I find his repertory very helpful in my most difficult cases .