Sunirmal Sarkar
with Aafreen Chunawala and Pratik Jain
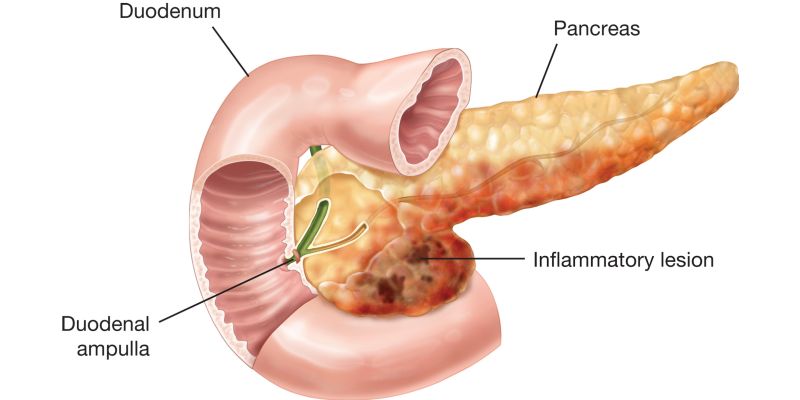
A 27 years old male patient presented with the complaints of Acute Necrotizing Pancreatitis of idiopathic onset, which started around October 2015. He came to Dr. Sarkar on 17th March 17. On a detailed evaluation done on Nov 2015, when admitted in Asian Institute of Gastroenterology Hospital the MRI showed multiple heterogenous ill-defined fluid collection around pancreas with loculated sub pulmonic collection on the left side. He was treated conservatively and discharged after symptomatic improvement. He was then again admitted on 2nd Jan 2016, with symptoms of pain in abdomen, fever & vomiting since 20 days. One Jan 2016, the blood investigation showed anemia, with normal RFT, LFT with hypoalbuminemia. USG abdomen showed altered echotexture of pancreas with pseudocyst in epigastric region. UGI endoscopy showed a smooth bulge at anterior wall of stomach. CECT abdomen showed an ill-defined fluid collection in tail of pancreas (6x 4.5 cm) and a large fluid collection in sub capsular portion of left hepatic lobe (20 x 12 x 8 cm). He underwent PCD placement to sub capsular hepatic collection on 6th Jan 16 which drained clear fluid with fluid amylase levels being 42.150 u/l. PCD continued to drain till 18th Jan 16 with reduction in amount of fluid, however then he started with mild to moderate fever. CT Scan showed decrease in sub-hepatic collection after which PCD was removed & second PCD placed in pancreatic collection. PCD fluid amylase was 61.850 u/l. He improved symptomatically after PCD placement.
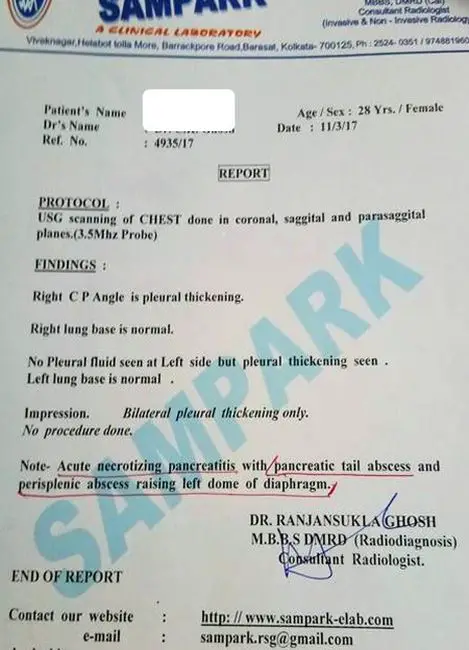
USG scanning of chest done on 11th March 17 suggested Bilateral pleural thickening because of acute necrotizing pancreatitis with pancreatic tail abscess and perisplenic abscess raising left dome of diaphragm.
In March 2017, haemoglobin was 12.2 gm/dl & ESR was 105 mm.
Homeopathic treatment by Dr. Sarkar:
The patient was suffering continuously, and was not helped by Allopathic treatment in Hyderabad, then finally they consulted Dr. Sarkar on 17th March 2017. At that time patient was having Recurrent fever with chilliness. His weight had reduced to 39 kgs from was 62 kgs earlier.
P/h – Recurrent fever during childhood
Hectic rise of temperature
Family history – Father expired due to Cancer.
Desire for eggs
Perspiration – offensive +
Hot patient
Stools offensive
O/E – Pulse – 120/ minute
Fever – 104/105 deg F
Rx on 17th March 17:
Pyrogen 50M 6 doses – 3 hourly for 2 days
Indication: high fever & hectic rise of temperature, pulse out of proportion with fever – fever was around 104-105, pulse is 120/minute – disproportionate pulse, perspiration offensive, on observation – red fiery tongue, profound weakness
On 20th March 17:
Fever had reduced
Pulse was still out of proportion
Offensive smell from mouth
Offensive sweat
Bodyache
Rx: Echinaceae MQ
Indication: helps in blood purification if there is history of infection.
On 27th March 17:
Lycopodium 1M for 2 days
Indication: Constipation, anorexia +++, flatulence, better by passing flatus, agg in afternoon
After 2 days-
Rx: Azadirachta Indica 30 for 2 days
Indication: fever decreased; Patient goes from Chilly to hot after every few days, otherwise all symptoms of Lycopodium
After 3 days – Rx: Andrographis Peniculata 30 for 2 days
Indication: Too much bitter taste in mouth
On 3rd April 17:
Complaints of Fever – maximum reaching to 105 degree F and also complaints of cough with expectoration like raw egg albumin.
On a mental level, Emotional +3, cries very easily. He has desires to become a singer since childhood, but the desire had to be suppressed. He says, he feels better in all ways, if he diverts his mind into singing.
He feels severely depressed because of his diagnosis.
Generally, his appetite is good, but unable to eat. Stools – not clear, semi-solid, can hold.
Sleeps on right side
Desire – for everything cold
Weight – 41 kgs
Rx: Carbo Veg 1M 6 doses – 3 hourly for 2 days
Indication: Offensive expectoration, expectoration ameliorates, aggravation in afternoon
On 17th April 17:
Desire for cold things
Desire for ice cream
Desire salty food
Prefers to lie on right side
Rx: Phosphorus 200– 2 doses
Indication: Sleeps on right side, desires everything cold, haemoptysis, expectorates frank blood
After 2 days – Pancreatinum 30 – 1 dose
Indication: As an organ remedy – Tautopathy
On 15th May 17:
Pancreas normal
Fever subsided
Bleeding decreased
Wt – 2.5 kgs increased
Stool – 3-4 times/ day
Rx: Phosphorus 1M– 2 doses
Indication:
Sleeps on right side, desires everything cold, haemoptysis, expectorates frank blood
Result:
In May 2017, Hb – 11.9 & ESR – 48 mm. LFT was completely normal in May 2017, with serum albumin also normal.
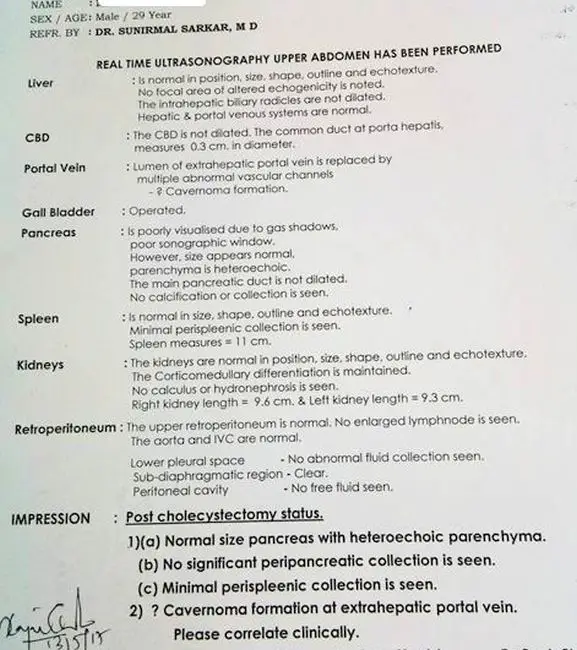
On 13th May 17, the real time USG of Upper Abdomen suggested a normal sized pancreas with heteroechoic parenchyma. No significant peri-pancreatic collection is seen, and minimal peri-splenic collection is seen.
Conclusion:
My approach to homoeopathy can be summed up in one word, simple. Most things in life are simple and should be kept simple, and homoeopathic practice is not an exception to this tenet. To be a fine homoeopath, one does not need to be intelligent, wealthy or have good contacts. A fine homoeopath must be honest, dedicated, and most importantly, have a large amount of courage to survive against all odds. My approach is overall very simple – the aim is to find out the most characteristic symptoms in the case and prescribe on these very symptoms. These characteristic symptoms can come in the form of Keynote(s), rubrics, themes, pathologies, or even a sensation. When this characteristic symptom is established and is sure, the remedy is prescribed based on this.
What is greatly needed for prescription is the current symptom totality. I look at the current symptom totality, see which remedy is the closest to this totality, and I prescribe it. I also take into account the pathogenesis of the remedy and the patient.
When I approach a case I begin looking for a chronology of events and ask questions such as, when and how did it start, what were the first symptoms, which organ system affected, what were the characteristics of those symptoms at that time? In addition, I also look at the direction in which the symptoms move – which side did it start, did it move or did it stay in a local area?
I aim to elicit exact symptoms and look for the causative factors – there may be one, or usually, there are many. With each symptom, location, sensation, modality and concomitant are critical to complete the symptom and to aid in prescribing an accurate remedy.
When investigating each symptom, I explore it in depth until I get a peculiar characteristic. This can be in any area of the case, mental, emotional or physical. I emphasize the importance of peculiar symptoms because that is what will ultimately help to match the patient to the remedy. I also place great importance on concomitant symptoms as they will help to quantify and qualify the experience of the patient.
At each level of the case, I choose the symptoms that are factually reliable, dependable and solid. Once I have a good grasp on these symptoms, I have a few remedies in my mind and the rest of the case is just confirmation of one of these very remedies. Eventually I find a remedy that correlates with most aspects in the case.
In summary, when I take a case, I build a solid foundation, addressing the pathology, toxicology, symptomatology and then the mind. It is a hierarchy which helps to organize my approach to cases and case taking.
I also frequently utilize the Ladder of Remedies concept of Dr. Burnett, to assist in chronic, complex cases. A ladder approach uses a series of remedies one after another, which ultimately lead to the restoration of the health in the patient. I find that to effectively help patients, the ladder approach is very beneficial because it targets the patient’s current ailments at the same moment they are experiencing them – with the ladder approach, you can treat the presenting picture of the patient and move on to the next remedy when that picture is no longer present. It should be mentioned that I do not employ or use polypharmacy (prescribing 2 remedies at the same time). Suppose a patient comes with an organ-specific problem, we can simply employ the use of an organ-specific remedy to alleviate their suffering. Once this suffering has been reduced or eliminated, a new picture of the patient will come up – and we can prescribe on the new totality.
To Learn more from the Living Legend himself –Dr. Sunirmal Sarkar – The ‘Man who makes you believe in Homoeopathy even more!’
“Materia Medica Live by Dr Sarkar” -A Grand National Homeopathic Seminar in INDORE
On 12th November 2017, Sunday | 9.30am to 6pm
Highlights of the seminar:
- How to Study different Materia Medica
- How to treat Acute cases
- How to treat fevers like Dengue, Malaria, Chikungunya, etc
- Different approaches in treating Pathological & Cancer cases
- How to use Smaller remedies & Indian Drugs
For More Details & Registration: Contact: 9869508345 | 9823126183 | 8871618593 | 9893200976 : Email to – [email protected]


Sir, dr. I badly need your phone no. To see you as early as possible.