Keywords: Bipolar Disorder, drug addiction, case report, homeopathic treatment
Abstract:
Bipolar disorder (BD) is a complex, chronic, dynamic condition with onset typically in early adulthood. It consists of pathological mood swings that include varying intensities of mania and depression. The aetiology of bipolar disorder remains unknown, and no reliable biological markers have yet been identified.
Conventional medicine employs a range of treatments which aim to reduce the severity and number of episodes of depression and mania. Homeopathy is a highly systematic method of stimulating the organism’s natural ability to restore order and balance at mental, emotional, and physical planes. This is a case report of a patient who was under psychiatric care for 13 years and the course of homeopathic treatment over the period of 3 years.
Introduction:
To be diagnosed with bipolar disorder (BD) (also known as manic depression), a person must have experienced at least one episode of mania. During manic episodes people feel exaggerated elation and a sense of invincibility.
It is often followed by an episode of depression, apathy and despondency. Lack of stability in mental-emotional state significantly affects sufferers’ quality of life – impairs many of their relationships, limits employment-ability and financial situation1. Suicide is an ever-present danger because some people become suicidal even in manic states2, 3.
The prevalence of bipolar disorder across the world varies from 0.3 to 1.2 percent by country. Globally, an estimated 46 million people in the world had bipolar disorder in 2017, with 52 and 48 percent being female and male, respectively4. Studies have shown that while both men and women can develop the disorder, there are gender differences in predominant polarity5, 6.
Cannabis use is linked with earlier age of onset of BD7, prolonged or worsened manic episodes8, and increased likelihood of suicide attempt9. A study conducted in Australia found that cannabis use was associated with decreased likelihood of long-term remission in BD10.
Conventional medicine employs a range of treatments which aim to reduce the severity and number of episodes of depression and mania. Treatments involve prescriptions of antidepressants, antianxiety, antipsychotic, mood-stabilising medication.
Longitudinal studies have observed that even patients who receive intense pharmacotherapy have lengthy and debilitating periods of subthreshold depressive symptoms after major episodes of mania or psychosis11, 12. While effectiveness of the drugs is questionable13 – 16, the reported side-effects create additional burden to already suffering patients17, 18.
In conjunction with pharmacological prescriptions, involvement of psychologists, psychotherapists, counsellors, family therapists and social workers is recommended19. Also, electroconvulsive therapy (ECT) is used for treatment-resistant acute mood episodes, especially when people experiencing depression with psychotic features20, 21. Admission to psychiatric wards is a common occurrence22, 23.
By using the individualised approach and highly systematic method of stimulation of the organism’s natural ability to restore order and balance at mental, emotional, and physical planes, homeopaths have successfully treated patients who were diagnosed with BD24 – 27. However, the possibility of relapse for marijuana users is 80% 28.
We present the case of a 32-year-old man, who was diagnosed with BD at the age of 19 and was under psychiatric care since then. Aside from occasional psychotic episodes, he continued to swing between mania and depression for the past 13 years.
Until recently he was a marijuana user. He struggled to hold employment. With family members keeping their distance afraid of his unpredictable, erratic behaviour, he felt isolated and unsupported.
Initial consultation – 06.01.2020
Male, 32 years old
Main complaint: Mood swings, manic episodes (occasional psychosis) followed by long periods of depression. Insomnia, could go on for many days without sleeping.
Background information
Eczema in early childhood and adolescence. Treated with cortisone creams.
Diagnosed with Bipolar Disorder at the age of 19 years old after having a psychotic episode.
Medicated for mood swings, psychosis, depression, and insomnia ever since.
Marijuana user since late teens. He has not smoked weed for the past 9 months.
Cigarette smoker.
History of sexual abuse.
Was committed to mental institution for 6 months in 2019.
Could not remember last fever.
Prescribed medication*:
Olanzapine/Zyprexa 15mg (antipsychotic agent) nightly
Lamotragine/Lamictal 200mg (antiepileptic drug used as mood stabilizer) nightly
Klobopin/Clonezapam 5mg (antianxiety agent) as needed (up to 3 times a day)
Melatonin 3-5mg (sleep medication) as needed
*The patient was still taking the prescribed medication.
Family history:
Mother had breast cancer
Table 1: Repertorisation of symptoms on 06.01.2020
| Mental/Emotional | Physical | Generalities |
| LOQUACITY 3
VERSES makes 2 DELUSIONS, hallucinations, illusions Christ, thinks himself to be 2 INJUSTICE, cannot support 2 THEORIZING 3 UNTIDY 2 LAZINESS 2 SADNESS, mental depression 2 PREACHING, religious psychotic 2 DELUSIONS, hallucinations, illusions floating in air 2 |
BLADDER URINATION frequent 2
BLADDER URINATION retarded, must wait for urine to start 2 BLADDER URINATION dribbling (by drops) urination after 3 STOMACH THIRST 3 EXTREMITIES NUMBNESS Foot 1 SLEEP SLEEPLESSNESS 3
|
FOOD and DRINKS sweets desire 2 |
Assessment of the Level of Health: According to Prof Vithoulkas’ Levels of Health theory [29], the patient was evaluated to be at Level 9-10, as he was suffering from severe mental disturbance; was heavily medicated with allopathic drugs for many years; had a history of substance abuse; and there was absence of acutes with high fever. These factors point to lower levels of health with poor prognosis.
Figure 1: Results are based on repertorisation using the online Vithoulkas Compass software.
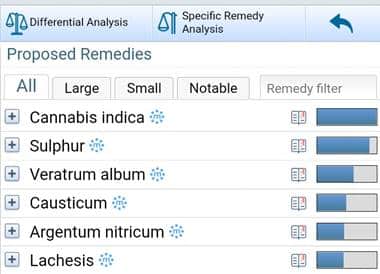
Prescription: Cannabis Indica 15C once a day until further notice (repeated doses of low potency are recommended in cases of low level of health and for those who are taking allopathic medication29).
Table 2: Follow ups*
*Below is a record of formal follow up consultations. However, the patient was in regular contact on a weekly basis.
| Date | Follow up | Prescription |
| 6.02.2020
|
Response to the remedy was immediate. He needed to sleep straight away. Was very sleepy for a couple of weeks.
Skin eruptions emerged on arms, legs and groin area. Would get itchy while in the shower. Frequent urination > Excessive perspiration. Feels a lot calmer. Talks less. Doesn’t mention issues of social injustice. Says that he feels less impulsive. Remorseful for causing his family so much grief. Laziness < Energy level is not excessive as it used to be. Reducing doses of allopathic medication (on his own accord)
|
Continue with Cann. I. 15c once a day
|
| 7.03.2020 | Feels as if he is starting life anew.
Stopped taking all allopathic medication. Theorizes. Overall feels content. He is surprised that he can be happy without feeling excessively elated. Sleep is good. Energy level good. |
Wait and watch. |
| 5.03.2021 | Organised himself a place to live independently.
Repaired his relationship with his parents. “Best it’s ever been.” Does not rely on his parents’ financial support. Employed on casual basis. No mood swings. Mourned the loss of his brother without falling into depression.
|
Wait and watch. |
| 3.05.2021
|
Overwhelmed by injustice, which is taking place all over the world.
Needs to follow through with his mission and save the world. Prays a lot, often in public. Preaches (on social media). Increased eructation. Desires meat and pickles. Thirsty. Dry skin.
|
Verat. Alb. 200C
20 minutes after taking the remedy, “I feel high!” Speech was noticeably slurred.
|
| 10.05.2021
|
Unexplained severe pain in right shoulder which lasted for a couple of days.
Skin eruptions agg. Perspiration increased. Frequent urination < A lot of energy. Feels happy, like “back in my own skin”
|
|
| 7.06.2021
|
Extremely talkative.
On the mission to save the world. Writes verses (a few a day). Doesn’t sleep. Manic, on the verge of psychosis (according to mother) Reveals that he smokes weed again. Complete relapse.
|
The patient is informed that he cannot be treated due to his drug use. |
| 15.07.2021
|
The patient called in panic reporting that he has a ‘cyst’ on the right side of his face.
The abscess is large, red, hot and painful to touch. Makes it difficult to open his mouth. Feels panicky, doesn’t know what to do. He has not smoked marijuana since previous follow-up.
|
Cann.i. 15c twice a day |
| 20.07.2021 | After taking the first dose, felt calmer and started sneezing.
After the 5th dose, the abscess opened up and started weeping. (No more doses as instructed) The abscess cleared and the wound healed in a couple of days. Sleep >
|
Wait and watch |
| 5.09.2021
|
Acute: Mild fever. Perspiration offensive. Increased thirst. Head and feet hot. | Sulph 30C
|
| 7.09.2021 | After taking the remedy, perspiration increased. Overall felt better.
Completely recovered from acute within 48 hours. |
Wait and watch. |
| 19.11.2021 | Sleeplessness.
Suppressed sexual desire due to celibacy (not in a relationship). Inclined to mast-urbate occasionally, followed by feelings of disappointment. Feeling of loneliness yet overwhelmed by company. Apathetic. No desire to work, even basic chores. Desire for salt. |
Con. 30C
|
| 30.11.2021 | Sleep improved significantly.
Overall feeling more confident and optimistic. Skin eruption agg. on elbows, underarms, legs, groin area. Energy level improved. |
Wait and watch. |
| 17.02.2022 | Anxiety over health, especially in the evening.
Difficulty focusing. Fear that something bad will happen. Nocturnal emissions. Disappointed when it happens. Pain in the right shoulder. Retarded urination, must wait for urine to start. Frequent urination. Desire fried eggs. |
Nat.Phos. 30C |
| 17.03.2022 | Calmer. Does not panic if an ambulance passes by. In the past it would make him worry about the emergency that would be taking place.
Sleep improved. Urination issues improved. Skin eruptions are not as painful as before. Quit cigarette smoking. |
Wait and watch. |
| 9.07.2022 | Acute: Itchy and painful skin eruptions. Inflamed multiple nodule-looking rash on covered parts of the body. The patient suspected scabies.
Anxious. Secretive – wouldn’t tell his family because he was afraid that they would accuse him of wrongdoings and blame him for spreading it to the family (while using their laundry) Cool application amel. |
Thuja 30C |
| 14.07.2022 | No new eruptions.
Old eruptions have calmed down. |
|
| 21.07.2022 | The rash has returned.
Worse at night. Intense restlessness. |
Rhus. Tox 30C |
| 29.07.2022 | After temporary amel. the rash has returned.
Up until this point, flare up had a seven-day pattern. Warmth of bed agg. Washing agg. |
Sulph. 30C |
| 2.08.2022 | Emotional agitation and skin eruption have calmed down. | Wait and watch. |
| 22.08.2022 | Anxiety over health. Anxiety about health of loved-ones.
Fear something bad will happen. Restlessness. Desire for company. Thirst for cold drinks. While the ‘scabies’ eruptions have healed, the earlier eruptions on the elbows, underarms, groin area have not improved.
|
Phos. 30C |
| 20.09.2022 | After taking Phos. 30C the patient experienced immediate sense of calm. This allowed him to be more focused and he was able to accomplish a lot more.
Energy level – good.
|
Wait and watch |
| 20.11.2022 | The patient has remained calm and collected.
In the past months he had no difficulty sleeping. Skin eruptions improved significantly. Reduced in size. No longer itchy or painful. |
Wait and watch |
Outcome: No psychotic episodes in the past 18 months. No episodes of mania or depression. Health-related anxiety significantly reduced. The patient has repaired relationships with his family. He holds permanent employment. He has organised and participated in big community projects, which required him to overlook many different tasks and work with many people. He remained focused and was able to work through difficult situations. For almost 3 years, he stayed free from allopathic medication.
In course of treatment, the patient was able to address old skin-related symptoms, which have since improved significantly.
Discussion:
Homeopathy considers a person in a diseased state, not a disease in a person. This approach seeks to understand the depths of the suffering in all three planes of a human being: physical, mental, and emotional. With thorough case-taking and repertorisation of symptoms, careful analysis and prescription precision, a homeopath aims to help patients to restore their natural ability to regain good health.
Aside from needing to identify the correct remedy, when treating a patient with a mental disorder, there is an additional challenge related to the level of support the patient may require. Hahnemann has warned that, “The physician and the attendants must always behave as if they believe such patient to be sane…. The cure of insane, raging, and melancholic patients can be accomplished only in an institution expressly appointed to that end, and not at home with their family.” 30
With the absence of homeopathic hospitals the job of attending to the patient as he or she moves forward in his/her healing falls on the homeopath. In this case, the patient reached out on the weekly basis (sometimes more often) just to update on what was happening and to be reassured that he was making progress.
The initial prescription of Cannabis Indica 15C has successfully addressed the core of the state the patient was in at the time. On the mental/emotional plane the patient has felt relief, which he hasn’t experienced in all the years he was under psychiatric care.
At the same time, there was an appearance of old symptom of skin eruption. The return of an old symptom and/or an aggravation of the skin, indicates that the case is moving in the direction of cure, provided that there is evidence of improvement on deeper level31, 32. It is important to note that mistreatment of skin eruptions with cortisone over a prolonged period can cause mental disturbance33.
Veratrum Album was prescribed based on the symptoms presented. However, it was assumed that the patient was no longer smoking marijuana (which he hasn’t done for over a year). The immediate “I feel high” feedback exposed what was really going on at the time. The return to marijuana smoking consequentially brought on the relapse (as expected in 80% of such cases28).
When the patient returned to be treated for an abscess, which appeared on his face, it was his mental/emotional state that directed to the correct remedy. While Cannabis Indica does not have many skin symptoms in its picture, it was the remedy the patient needed to treat the acute.
Later, when the main complaint was sleeplessness, Conium was identified as the required remedy. The prescription was based on the fact that the patient was experiencing deprivation of regular sexual activity34. Again, aggravation of skin symptoms and improvement of mental/emotional state, sleep, and energy level show that the remedy was correct.
The following prescriptions for his chronic state – Nat. Phos. and later Phos., helped to address his anxiety and restlessness. The most recent prescription also helped to calm the skin eruption without suppressing it.
In the course of the treatment, the patient has experienced acutes. However, none of them were accompanied by high fever. This indicates that while the patient has made progress, he remains in the lower level of health.
Based on the fact that he had aggravations when treated for chronic disturbances, we can conclude that he was at level 9, not 10, at the beginning of treatment. Patients at level 10 and lower are too weak to experience aggravations29.
The limitation of this case report is that there is a possibility that the improvements have taken place due to the patient quitting marijuana use. However, the deep changes in the emotional level indicate otherwise. The return of old symptoms in response to treatment also serve as evidence that the organism was stimulated to act in the direction of cure. The MONARCH evaluation for causality indicates a score of 10.
Table 2: Modified Naranjo Criteria for Homeopathy – for Causality Assessment
| Criteria | Y | N | Not sure/NA | Score in case |
| 1. Was there an improvement in the main symptom or condition for which the homeopathic medicine was prescribed? | 2 | -1 | 0 | 2 |
| 2. Did the clinical improvement occur within a plausible time frame relative to the drug intake? | 1 | -2 | 0 | 1 |
| 3. Was there an initial aggravation of symptoms? | 1 | 0
|
0 | 1 |
| 4. Did the effect encompass more than the main symptom or condition, i.e., were other symptoms ultimately improved or changed? | 1 | 0 | 0 | 1 |
| 5. Did overall well-being improve? | 1 | 0 | 0 | 1 |
| 6 (A) Direction of cure: did some symptoms improve in the opposite order of the development of symptoms of the disease? | 1 | 0 | 0 | 1 |
| 6 (B) Direction of cure: did at least two of the following aspects apply to the order of improvement of symptoms:- from organs of more importance to those of less importance, from deeper to more superficial aspects of the individual, from the top downwards | 1 | 0 | 0 | 1 |
| 7. Did “old symptoms” (defined as non-seasonal and non-cyclical symptoms that were previously thought to have resolved) reappear temporarily during the course of improvement? | 1 | 0 | 0 | 1 |
| 8. Are there alternate causes (other than the medicine) that with a high probability could have caused the improvement? (consider known course of disease, other forms of treatment, and other clinically relevant interventions) | -3 | 1 | 0 | 1 |
| 9. Was the health improvement confirmed by any objective evidence? (in this case by conception) | 2 | 0 | 0 | 0 |
| 10. Did repeat dosing, if conducted, create similar clinical improvement? | 1 | 0 | 0 | 0 |
| Total | 10 |
Conclusion:
This case report serves as an example of the healing process, when the person is considered as a whole. An accurate prescribing can meet the person at the depth of his or her disturbance, which in turn can facilitate restoration of health. Even though patients suffering mental disturbance face a lengthy and difficult journey towards better health, it should not discourage homeopaths in attempting to help these patients.
References:
- Charles Cotrena, Laura Damiani Branco, Flávio Milman Shansis, Rochele Paz Fonseca, Predictors of quality of life in bipolar disorder: A path analytical study, Psychiatry Research, Volume 285, 2020, 112846, ISSN 0165-1781
- Akiskal HS. Targeting suicide prevention to modifiable risk factors: has bipolar II been overlooked? Acta Psychiatr Scand. 2007;116:395–402.
- Rihmer Z, Pestality P. Bipolar II disorder and suicidal behavior. Psychiatric Clin North Am. 1999;22:667–673.
- Saloni Dattani, Hannah Ritchie and Max Roser (2021) – “Mental Health”. Published online at OurWorldInData.org. Retrieved from: ‘https://ourworldindata.org/mental-health‘
- Nivoli AM, Pacchiarotti I, Rosa AR, Popovic D, Murru A, Valenti M, et al. Gender differences in a cohort study of 604 bipolar patients: the role of predominant polarity. J Affect Disord. 2011;133:443–449.
- Cotton SM, Lambert M, Berk M, Schimmelmann BG, Butselaar FJ, McGorry PD, et al. Gender differences in first episode psychotic mania. BMC Psychiatry. 2013;13:82.
- Bally N, Zullino D, Aubry JM. Cannabis use and first manic episode. Journal of Affective Disorders. 2014 Aug 20;165:103-8. 20.
- Gibbs M, Winsper C, Marwaha S et al. Cannabis use and mania symptoms: a systematic review and meta-analysis. Journal of Affective Disorders 2015;171:39-47. 21.
- Carrà G, Bartoli F, Crocamo C et al. Attempted suicide in people with co-occurring bipolar and substance use disorders: systematic review and meta-analysis. Journal of Affective Disorders 2014;167:125-35.
- Kim SW, Dodd S, Berk L et al. Impact of cannabis use on long-term remission in bipolar I and schizoaffective disorder. Psychiatry investigation 2015;12(3):349-55.
- Judd LL, Akiskal HS, Schettler PJ, et al. The long-term natural history of the weekly symptomatic status of bipolar I disorder. Arch Gen Psychiatry. 2002;59:530–37.
- Judd LL, Akiskal HS, Schettler PJ, et al. A prospective investigation of the natural history of the long-term weekly symptomatic status of bipolar II disorder. Arch Gen Psychiatry. 2003;60:261–69.
- Sachs GS, Nierenberg AA, Calabrese JR, et al. Effectiveness of adjunctive antidepressant treatment for bipolar depression. N Engl J Med. 2007;356:1711–22.
- McElroy SL, Weisler RH, Chang W, et al. A double-blind, placebo-controlled study of quetiapine and paroxetine as monotherapy in adults with bipolar depression (EMBOLDEN II) J Clin Psychiatry. 2010;71:163–74.
- Sidor MM, MacQueen GM. An update on antidepressant use in bipolar depression. Curr Psychiatry Rep. 2012;14:696–704.
- Al-harbi. Treatment-resistant depression: therapeutic trends, challenges, and future directions. PPA. Published online May 2012:369. doi:10.2147/PPA.S29716
- Cartwright C, Gibson K, Read J, Cowan O, Dehar T. Long-term antidepressant use: patient perspectives of benefits and adverse effects. Patient Prefer Adherence. 2016; 10:1401-1407. doi:10.2147/PPA.S110632
- Paige E, Korda R, Kemp-Casey A, Rodgers B, Dobbins T, Banks E. A record linkage study of antidepressant medication use and weight change in Australian adults. Aust N Z J Psychiatry. 2015;49(11):1029-39. doi:10.1177/0004867415607365
- Swartz HA, Swanson J. Psychotherapy for Bipolar Disorder in Adults: A Review of the Evidence. Focus (Am Psychiatr Publ). 2014 Summer;12(3):251-266. doi: 10.1176/appi.focus.12.3.251. PMID: 26279641; PMCID: PMC4536930.
- Kellner C.H., Ahle G.M., Geduldig E.T. Electroconvulsive therapy for bipolar disorder: evidence supporting what clinicians have long known. J. Clin. Psychiatry. 2015;76(9):e1151–e1152.
- UK ECT Review Group Efficacy and safety of electroconvulsive therapy in depressive disorders: a systematic review and meta-analysis. 2003.
- Kim E, Maclean R, Ammerman D, et al. Time to psychiatric hospitalization in patients with bipolar disorder treated with a mood stabilizer and adjunctive atypical antipsychotics: a retrospective claims database analysis. Clin Ther. 2009; 31: 836–848
- Kim E, You M, Pikalov A, et al. One-year risk of psychiatric hospitalization and associated treatment costs in bipolar disorder treated with atypical antipsychotics: a retrospective claims database analysis. BMC Psychiatry. 2011; 11: 6.
- https://hpathy.com/clinical-cases/a-case-of-bipolar-disorder/
- https://hpathy.com/clinical-cases/case-bi-polar-disorder-lac-puma/
- https://hpathy.com/clinical-cases/bipolar-schizoaffective-disorder-in-a-boy-of-18/
- https://ndnr.com/neurology/homeopathic-management-of-pediatric-bipolar-disorder-2/
- Vithoulkas George, The era of Marijuana the use and its consequences, lecture, published 2015 https://www.youtube.com/watch?v=L6c5eR6vMC4&ab_channel=GeorgeVithoulkas
- Vithoulkas George, Levels of Health, revised edition, International Academy of Classical Homeopathy, 2017, Greece
- Hahnemann Samuel, Organon of Medicine, translated by Kunzli M.D., Naude and Pendleton, Orion Books Ltd, England, 2003
- Vithoulkas George, The Science of Homeopathy, B.Jain Publishers Pvt. Ltd., 1980, India
- Mohinder Singh Jus, The Journey of a Disease, B.Jain Publishers Pvt. Ltd., 2010, India
- Vithoulkas George, Essence of Materia Medica, 2nd edition. B. Jain Publishers, India, 1990
- Vithoulkas George, Materia Medica Viva, Volume 9, 3rd edition, International Academy of Classical Homeopathy, Greece, 2012



Great work Elka! The MONARCH inclusion adds extra weight to the outcome. Thanks for sharing.