Abstract
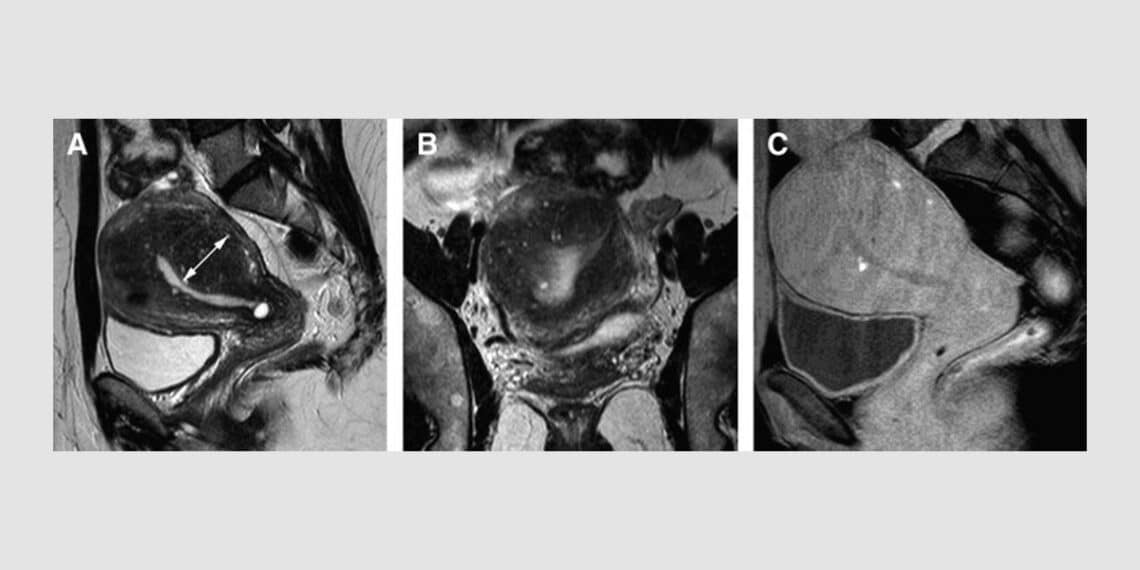
Adenomyosis is a common gynecological disease of myometrium infiltration by endometrial glands and stroma, often giving rise to dysmenorrhea, pelvic pain, menorrhagia, and infertility. Adenomyosis is increasingly identified in young women by transvaginal ultrasound and magnetic resonance but streamlined international surgical and medical treatment guidelines are lacking.
The following case report outlines adenomyosis in a 36-year-old nulliparous Australian woman who was treated with individualized classical homeopathy for one year alongside the standard medical protocols of endometrial ablation and Implanon rod insertion.
Retrospectively, an initial posological misstep encouraged the author to publish this case report in order to highlight the importance of working within the Levels of Health theorem.
Keywords
Adenomyosis. Levels of Health theory. Posology. Remedy reactions.
Introduction
Adenomyosis is characterized by the presence of endometrial glands in myometrium, typically manifesting pelvic pain, abnormal uterine bleeding and infertility. Although adenomyosis and endometriosis share a number of features, they are considered to be two different medical conditions1.
Adenomyosis often coexists with other gynaecological conditions, such as endometriosis and uterine fibroids, and has a negative impact on quality of life. Its pathogenesis remains elusive, and no one theory can explain its different phenotypes.
Current treatment is a lifelong symptom management plan. Once considered the classic condition of multiparous women over 40 years old with pain and heavy menstrual bleeding and diagnosed at hysterectomy, the present epidemiological scenario has completely changed, and adenomyosis is now increasingly identified in young women2.
Case report
36-year-old nulliparous woman presenting with a recent diagnosis of adenomyosis, and associated iron deficiency anaemia.
Initial consultation
2021-07-12. Australia.
Main complaint
‘I am literally bleeding to death’ from painless uterine haemorrhage, 50ml daily loss of ‘bright red blood which pours out of me, gushes out.’
Heavy, protracted, and inconsistent menses developed during marital discord two years’ prior. Uterine fibroids (left sided) diagnosed in Oct 2019. Irregularity of menses worsened after replacement of contraceptive pill (taken for sixteen years’) with an Intra Uterine Device (IUD) in July 2020.
Abnormal heavy uterine bleeding without dysmenorrhea, and intermittent passing of very large, painful clots, described by the patient as ‘the size of my shoe’ began in Nov 2020. During this period, she was under extreme work stress, and was prescribed Ciprofloxacin for unexplained high fever a few days prior.
She underwent exploratory uterine procedure, removal of the IUD and biopsy after IUD had dislodged, resulting in diagnosis of adenomyosis, and was scheduled for uterine ablation in one weeks’ time, with planned insertion of the Implanon rod. Tranexamic acid and Estrogen had been prescribed but she was not currently taking either. Iron infusion had no effect, and she was taking supplemental iron Maltofer twice daily.
Table 1: Past Medical History
| Diagnosis | Intervention |
| Severe upper respiratory tract (URTI) infections (with no reported fever), yearly as a child with a thudding in the head – still feels this now in arms/hands when lying on the couch occasionally. | Multiple antibiotics. |
| Infectious mononucleosis aged 17 – in bed for a week – rest to recover; to begin university. | |
| Recurrent urinary tract infections (R-UTI) aged 18 – late 20’s (no fevers) – accompanied by antibiotic induced vaginal thrush. | Multiple antibiotics. |
| Human Papilloma Virus (2008). | Large loop excision of the transformation zone (LLETZ) (2008). |
Table 2: Family Medical History.
| Siblings | Endometriosis (Sister). |
| Maternal Line | Goitre, benign thyroid tumours (Mother).
Dementia. |
| Paternal Line | Polycythaemia (Father-deceased).
Type 2 diabetes, myocardial infarction, dementia. |
Analysis
Progression of the original disturbance from the respiratory system to the urinary system to the reproductive system is indicative of significant chronic health burden. The continuum of a unified theory of diseases3 postulates that continued and incorrect treatment of acute inflammatory diseases i.e., with multiple antibiotic prescriptions leads, via suppression, to sub-acute inflammatory process aka chronic, degenerative disease. Here this theory is confirmed – immune system dysfunction / chronic disease progresses in a non-healthful direction.
Looking at the hierarchical structure within the three levels of the human being energy complex, we note with concern that both maternal and paternal lines have dementia – the deepest pathology. Burdened predisposition, peripheral disturbance i.e., physical pathology which has steadily descended layers, and dissatisfaction (marital) – an identified contributing factor to the current condition – involving the emotional sphere4 gives weight to descending and deteriorating health.
Table 3: Repertorization of presenting symptoms
| Mental / Emotional | Physical | Generalities |
| MIND – ANIMALS – love for (3) | GENITALIA – FEMALE – METRORRHAGIA – bright red (4) | GENERALITIES – FOOD & DRINKS – fish – desire (1) |
| MIND – PLEASING – desire to please others (2) | GENITALIA – FEMALE – METRORRHAGIA – gushing (4) | |
| MIND – FANCIES – vivid (1) | GENITALIA – FEMALE – METRORRHAGIA – continuous (4) | |
| GENITALIA – FEMALE – METRORRHAGIA – painless (4) | ||
| GENITALIA – FEMALE – METRORRHAGIA – profuse (4) | ||
| GENERALITIES – ANAEMIA – haemorrhage, after (4) | ||
| GENITALIA – FEMALE – METRORRHAGIA – emotions, excitement etc., (3) | ||
| GENITALIA – FEMALE – METRORRHAGIA – bright red, clots, with (3) | ||
| GENERALITIES – SIDE – left (3) | ||
| GENITALIA – FEMALE – METRORRHAGIA – concussions (3) | ||
| GENITALIA – FEMALE – METRORRHAGIA – coition (2) | ||
| GENITALIA – FEMALE – METRORRHAGIA – exertion, after (2) |
Table 3 The numbers 1-4 denote intensity of symptom – (4) extreme; (3) strong; (2) moderate; (1) mild
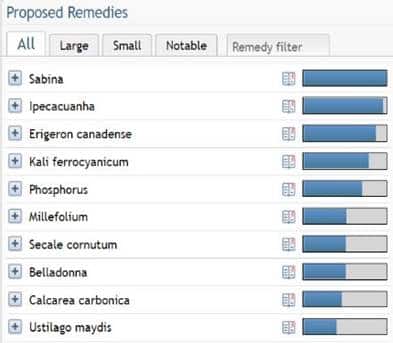
Figure 1: Results based on repertorization of symptoms (Table 1). Vithoulkas Compass (2022)
Remedy differentiation
SABINA – Metrorrhagia with active, gushing flow of bright red blood, or mixed with clots. The great guiding symptom is ‘pain in the back radiating to the pubis’, excruciating pelvic pains, severe dysmenorrhea, or more generalized back and pelvic pain5 is not seen in this case.
IPECACUHUANA – Uterine haemorrhage that starts suddenly with bright red uncoagulated blood, coming in gushes, often with nausea, vomiting & faintness5 is not seen in this case.
PHOSPHOROUS – Haemorrhagic tendency, debility & collapse states, left sided symptoms, fibrocystic growths, uterine fibroids, Metrorrhagia with bright, red blood – almost never clotted, prices are paid for poor boundaries5. As if there are no barriers which on the physical manifests in haemorrhage from any injury or stress.
Painless haemorrhage. While physical symptoms predominate there are few mental / emotional symptoms. Puts concerns of others above themselves, vulnerable to all types of influence, emotions go freely to others, little ability to contain and protect oneself from emotional vulnerability, – can be seen here as ‘trying to please everyone else – over giving my time & energy. ‘Causation of strong emotions, anger.’ Daydreaming – fantasizing. Typical craving for fish, and characteristic thirst for ice cold drinks6.
USTILIGO – Uterine haemorrhage, fibroids with haemorrhage, metrorrhagia5.
Posology
Levels of Health theory makes posology logical and comprehendible. Factors determining the Level of Health of an individual are: Hereditary disposition; Individual actions concerning the management of health; Vaccination, and unnecessary drugs, taken by the individual, and their ancestors7.
This complex presenting complaint combined with a convoluted personal medical history, additional weight of severe pathologies in both her parents, and coupled with the fact that her last known fever was recent but unexplained and not associated with two head colds, indicates a Level of Health classification 7 where systemic, chronic disease will manifest in full strength symptomatology after stress7.
Prescription PHOSPHOROUS
Potency 1M
Regimen One dose daily for two days.
Table 4: Reaction to the remedy – first follow-up – four week’ after the remedy
| Overall Patient’s Impression | Reaction to the prescription | Analysis of the reaction |
| ‘No bleeding for two days after taking my Phosphorous and was going to cancel the uterine ablation scheduled for that week.’
‘Have been feeling better, not as feeble, and have also been less emotional these past few weeks – work seems easier now. |
Endometrial ablation performed. The surgeon advised 30% have reduced bleeding post endometrial ablation. Implanon rod inserted. Uterine bleeding is increasing. | No aggravation post remedy was reported. It is impossible to analyse the reaction here due to the endometrial ablation general anaesthesia, and painkillers on day three, after two days of cessation in bleeding. |
Prescription: The only option here was to repeat Phosphorous 1M to ascertain if it was the correct remedy, or not.
Table 5: Reaction to the remedy – second follow-up – two months after the remedy
| Overall Patient’s Impression | Reaction to the prescription | Analysis of the reaction |
| ‘Bleeding stopped for the two days I took the Phosphorous, I was feeling better, but it has been getting increasingly heavier since.’ ‘I’m putting boundaries up, now I’m not very concerned any more about who wants what from me, or that huge fear of letting people down.’ | Temporary amelioration without initial aggravation, then full relapse after one month. (Observation 11 – Vithoulkas, 2017) | No initial aggravation is not a good sign, the duration of amelioration clearly shows something is wrong
resulting in the person feeling better for a little while, the best course of action is to retake the case and study the symptoms in depth to discover a better suited remedy7. |
Symptoms that have been ameliorated
MIND – PLEASING – desire to please others (Table 1) ‘I’m putting boundaries up, now I’m not very concerned any more about who wants what from me, or that huge fear of letting people down.’
Prescription: After much study of differential remedies, I was loathe to change the only well indicated remedy, Phosphorous, too quickly. So, I investigated Level of Health 7 for which an initial potency of 200c is advised7. This is homeopathy 101, feeling very sheepish to admit this here! Phosphorous 200c one dose daily for two days only to begin.
Table 6: Reaction to the remedy – third follow-up – four months after the remedy
| Overall Patient’s Impression | Reaction to the prescription | Analysis of the reaction |
| ‘Day 2 extreme reduction in bleeding to lightest I’ve had.’
‘Really bad gush with emotions, my nephew has a tumour, he’s 6, & having surgery.’ ‘My boundaries get stronger – I have de-friended two couples who were draining me, always’ |
Uterine bleeding steadily increases. Observation 11 (table 5) is the closest but not completely reflective here. Vithoulkas states that this reaction occurring again & again could be a compromised person who battling development of a serious chronic condition (p126)7. Another perspective is that it may be placebo effect at work (p126)7. | Strengthening ‘boundaries’ is a good sign that Phosphorous, who tends to put others’ concerns above their own, is exerting influence, as is the bad gush with strong emotions lending weight to the known Phosphorous trait as if there are no barriers which on the physical manifests in haemorrhage from any injury or stress6. |
Prescription: Phosphorous 200c one dose daily for two days only to begin, with instructions to repeat the dose when bleeding returns as relapse indicates demand for repetition and a tenacious belief that Phosphorous was the similimum.
Table 7: Reaction to the remedy – fourth follow-up – seven months after the remedy
| Overall Patient’s Impression | Reaction to the prescription | Analysis of the reaction |
| ‘Significantly less bleeding, barely any. Had sex with husband, helped us so much. Really happy with how I am going. Also started exercising with no issues. No longer anaemic’
Three repeats of Phosphorous 200c from the last follow up. |
It is impossible to state whether Phosphorous has had any real effect due to an endometrial ablation and implanon. A complicated case. I worked many, many hours to manage this case as best I could.
|
It could be the placebo effect, but due to the perceived amelioration of MIND – PLEASING – desire to please others (her boundaries), this is unlikely as the placebo effect ameliorates all areas with the remedy action simply fading away (pg126)7. |
Prescription: Phosphorous 200c instructions to repeat one dose when bleeding returns.
Table 8: Reaction to the remedy – one year later
| Overall Patient’s Impression | Reaction to the prescription | Analysis of the reaction |
| ‘Homeopathy helps – it stops periodic excess bleeding within 12hours.’
‘My life and work are significantly less stressful now – I have fantastic work/life balance.’ |
Menses remain irregular with light spotting, three times it has increased, and a dose of Phosphorous 200c taken.
|
It cannot be stated that Phosphorous has made any difference at all to this case. Although there was a glimmer of reduced haemorrhage initially, this now is just as likely due to the endometrial ablation and Implanon rod and here we have a case of suppression via surgery and synthetic hormones. |
Discussion
An organism overloaded with various hereditary predispositions created not only by the primary miasms of psora, sycosis, and syphilitic but also by poorly treated infectious diseases7, 8, will descend down through the Levels of Health.
Advancements in homeopathic theory4, 7, 8 state Hahnemann’s miasms are but a glimpse into understanding genetic predisposition, and its descent through the Levels of Health which enables the miasms to start exerting effect, which is usually further convoluted by medical interventions. According to Vithoulkas (p.108)4,
“Since allopathic drugs are never selected according to the Law of Similars, they inevitably superimpose upon the organism a new drug disease which then must be counteracted by the organism.”
I have submitted this case not as an example of a good outcome or prescribing but rather to highlight the importance of adherence to a sound theoretical basis for every prescription we make. If I had followed my own advice here and initially matched the potency to the level of health – who knows, the ablation and rod may have not been taken, with a much clearer case before you now.
Conclusion
My advice? Know homeopathic theory and apply it to every, single case before you. Master homeopaths of superlative mind have figured this all out for us humble prescribers. We just need to be aware of, mimic, and always apply, their methods.
References
- Lacheta, 2019. Uterine adenomyosis: pathogenesis, diagnostics, symptomatology and treatment. Ceska Gynekol. Spring;84(3):240-246. English. Available from https://pubmed.ncbi.nlm.nih.gov/31324117/
- Vannuccini & Petraglia, 2019. Recent advances in understanding and managing adenomyosis. Mar 13;8:F1000 Faculty Rev-283. Available from https://pubmed.ncbi.nlm.nih.gov/30918629/
- Vithoulkas G, Carlino S. 2010. The “continuum” of a unified theory of diseases. Medical Science Monitor [online]. Feb;16(2):SR7-15. Available from https://pubmed.ncbi.nlm.nih.gov/20110932/
- Vithoulkas, G. 2014. The Science of Homeopathy; Seventh edition. Alonissos: International Academy of Classical Homeopathy.
- Morrison, R. 1993. Desktop Guide to Keynotes and Confirmatory Symptoms. Grass Valley. Hahnemann Clinic Publishing.
- Vithoulkas, G. 2012. Essence of Materia Medica, Second edition. 14th B. Jain Publishers. New Delhi, India.
- Vithoulkas, G. 2017. Levels of Health, The second volume of the Science of Homeopathy, revised edition. Alonissos: International Academy of Classical Homeopathy.
- Vithoulkas & Chabanov, 2022. The Evolution of Miasm Theory and Its Relevance to Homeopathic Prescribing. Oct 28. Available from https://pubmed.ncbi.nlm.nih.gov/36307103/
- Vithoulkas Compass, 2022. Vithoulkas Compass Homeopathy Software [computer program]. Greece.
- Vithoulkas & Chabanov, 2022. The Evolution of Miasm Theory and Its Relevance to Homeopathic Prescribing. Homeopathy. Oct 28. Available from https://www.thieme-connect.com/products/ejournals/html/10.1055/s-0042-1751257#info


