(This case was originally published in Links in 2006 and this is an updated version.)
Summary
What was Hahnemann’s belief regarding miasms and how can this knowledge be used in clinical practice? Facial analysis is a system that has been developed by Melbourne homeopath and researcher Grant Bentley. In this article Grant highlights the importance of understanding a patient’s dominant miasm through using facial analysis. He discusses how many patients can be helped without delving deeply into their mental state by using facial analysis as an objective tool. This situation is demonstrated with a case of a young autistic boy who came into the clinic with colds and a few months later was declared to be no longer autistic.
Keywords: Miasm, Facial analysis, Autism, Dulcamara
What is a miasm?
Hello from Australia, unfortunately the tyranny of distance still exists and valuable information still takes a while to be exchanged from one corner of the world to the next. This being the case I would like to share with you some exciting new developments that have been occurring here in Melbourne.
Firstly, I need to introduce myself. My name is Grant Bentley and I am the principal of a small classical homeopathic college that has been teaching homeopathy since 1989. The college has always prided itself on being a traditional institution dedicated to the fundamental teachings of Hahnemann, Boenninghausen, Kent and Roberts, all the accepted classics.
Approximately five years ago (now almost ten years), I started a project for the purpose of answering one simple question, ‘what exactly is a miasm?’ Currently the word miasm can mean a hundred different things and is applied in just as many different ways. Therefore, it is important to state that I was trying to find out what Hahnemann meant by the term as well as how he tried to use them.
The answer to the question: ‘what is a miasm’, is easy. A miasm (1) is an inherited predisposition towards a particular style of chronic illness that is triggered into effect when the right environmental conditions are bought into play. There are no surprises in this; after all it’s hardly like cracking the DaVinci code, since Hahnemann was so open about the subject in both the ‘Organon’ and ‘Chronic Diseases’.
(1) In 2006 I knew a miasm was an inherited predisposition because of the link to facial structure. In 2009, through research involving physics (energy, force, direction and shape) combined with the study of history and disease I further expanded my understanding of a miasm. I now can prove its link to our miasm/type of vital force or as I call it – a survival instinct. The survival instinct or miasm controls our emotions, our immune system, our nervous system and links directly to our facial structure. Every patient has a dominant miasm – every remedy has a dominant miasm. Every remedy chosen for a chronic problem MUST match the internal protective mechanism (survival instinct, miasm) of the patient for a deep and effective outcome.
Now we come to the question, ‘How do we make use of this knowledge in practice?” This is the sticking point. Hahnemann was certain in his knowledge that miasms are the key to understanding chronic disease, but even he showed through his clinic that he was unsure of exactly what to do with them. This I believe is the reason he gave nearly all his patients a dose of Sulphur. In his mind psora was the mother of all disease, therefore everyone must have psora, and Sulphur is the great anti-psoric, so everyone needs Sulphur. The thinking is logical but not what we would consider homeopathic because of the switch in emphasis from the idiosyncratic prescription to the routine. Even Boenninghausen wrote that there was no accurate way of determining one miasm from another.
Later in the homeopathic timeline, Hahnemann’s miasmatic theory became synonymous with hypo, hyper and dys function. Allen and Roberts are good examples of this belief and it is here that the fun begins.
True to the concept of holism, everything external effects the internal and this of course is a basic homeopathic tenet and why we do not apply ointments. However, holism also means that the reverse must be true. Therefore, everything internal must have its corresponding external counterpart. In other words, if a person has an internal sycotic or ‘hyper’ tendency, they must also have external sycotic or ‘hyper’ tendencies.
The development of how this theory was put together is explained in my book, Appearance and Circumstance (2), but for the brevity of this article, I will simply state that after much research the hypothesis that ‘miasms influence externally as much as they do internally’ has gone from suggestion to fact.
(2) Since 2006 I have published a desktop guide to facial analysis – Homœopathic Facial Analysis and a philosophy book on the seven survival instincts (miasms) called Soul & Survival. See
Facial analysis
Boenninghausen would be pleased, because now there is a way to determine one miasm from another, and the answer has been literally staring us in the face. If a person has a natural predisposition toward hyper or excess function, that tendency will be reproduced in their facial structure. Therefore, by using facial analysis we can determine the miasm that is dominant in the patient.
Facial analysis means dissecting each facial feature to determine what inherited process is the strongest, hypo or small, hyper or large, or dys or inward function. Traditionally face reading meant trying to determine personality but Homœopathic Facial Analysis (HFA) is only for assessing miasmatic influence.
Hahnemann stated clearly that a remedy based on the totality of symptoms as well as the miasm was a far deeper remedy than one based on totality alone. For example, based just on totality alone it is common for two remedies such as Sulphur or Mercury to feature prominently in a repertorisation. However, although both may include the symptoms of the case, they cannot possibly be interchangeable, and the reason is because of their different essence. Not essence in the contemporary form meaning personality type, but essence in regard to quality of action within the remedy. Sulphur has an irritated quality, an instinct to push things out, to drive out onto the skin for all to see. Sulphur as a remedy demands attention. Mercury does not have this quality, it is syphilitic and as such, it is dysfunctional and inward. Mercury ulcerates and degenerates, it hides and covers over and sneaks in quietly. They may both be near the top of the repertorisation but only one could ever be seriously considered for the case when linked to facial analysis.
Not all patients have a strong pathological history and this limits us to clearly see whether the trend is inward, outward or otherwise (3). Many have few if any obvious miasmatic signposts, so how do we choose between Sulphur and Mercury. Boenninghausen wrote the words he did because he knew that pathology is a poor indicator of the miasm, and yet he knew enough to know that we needed to include the miasm in our prescription. Facial analysis is without doubt the best indicator to the miasm and, it is objective – and objectivity is sorely lacking in modern homeopathy.
(3) My research between 2006 and 2008 has led me to the understanding that there are three basic energy forces that are the drive behind all material life and how our universe operates. Outward energy (psora), inward energy (syphilis) and circular energy (sycosis).
By applying facial analysis, the distinction between Sulphur and Mercury is clear. If the patient has smaller eyes, thin lips a curved or hooked nose and two lines between their eyes, I know these are all features of psora therefore my choice is Sulphur. However if the patient has dimples, recessed eyelids and is balding then I would know that syphilis is dominant so Mercury becomes my choice.
If the patient has large protruding eyes, full lips and a low straight hairline (4), I know that I would be searching for a sycotically dominant remedy and would therefore need to move away from both Sulphur and Mercury. My choice might be Sepia, a remedy a little further down the list.
(4) All the facial features listed above are examples of features found in each of the three primary miasms (psora, sycosis and syphilis). I have confirmed more than seventy features and a patient can have an endless variation of any of these features which accounts for individual appearance. Only by deciding the dominance of the features can the final of the seven miasms (psora, sycosis, syphilis, syco-psora, syco-syphilis, tubercular, cancer) be determined.
Finally, there is one last adjustment to the system. We live in a very politically correct time and it is now improper to talk in harsh or unpleasant terms. Compton Burnett’s book on Delicate, Backward, Puny and Stunted children for example if written today would most likely be titled: ‘refined, not yet competent, vertically challenged young people’. With this in mind, psora, sycosis and syphilis have become yellow, red and blue respectively (5).
(5) – There are seven miasms – each has been given a colour to stop the natural tendency of linking miasms to specific diseases.
– Psora – yellow
– Sycosis – red
– Syphilis – blue
– Syco–psora – orange
– Syco-syphilis – purple
– Tubercular – green
– Cancer – brown
Benefits
Not all patients like to talk about themselves or their feelings. However, using this system, that problem is overcome, as psychoanalysis plays a far lesser role than it does in other contemporary methods. Facial analysis screens remedies – those that do not belong to the same miasmatic group as the patient are automatically discarded. This does not mean that delving into a patient’s state of mind is a waste of time, but at the same time it must be acknowledged that only a certain type of patient is willing to do so. In my clinic, only about thirty percent of patients would suit this criteria. Men often feel far too uncomfortable with this line of questioning and children don’t know how to answer. Even many women are too defensive to be pushed.
To me the consultation is all about the patient. If they want to go deep, then I go deep. If they want to stay topical then that is where I stay. Experience with this model proves that facial analysis combined with a few good generals’ means that miracles can occur.
The following is just one example. He is a young autistic boy who cannot talk, brought in by his grandmother who refuses to say anything negative about him. He has no physical pathology save for a few minor symptoms. In short, if I did not have facial analysis to fall back on, the following result would most likely not have occurred.
Case – Autism and continuous colds
 A three year old male child comes to clinic in March 2005 with continuous colds and discharges from the ear and nose. He runs from one cold into another continuously with perhaps a break of two to three days in between. He is fully vaccinated and has had measles. He has been diagnosed as autistic by a specialist that was organised by the family G.P. He cannot or will not talk and only points and grunts and makes noises; he has never said a word. He does not participate in any games and even though he is inquisitive he has a very poor concentration span that inhibits him from learning anything in detail. No fantasy play is ever undertaken and a diagnosis of hyperactivity has also been given by the same behavioural specialist. The only thing he likes to do continuously is to place things like toy cars in a line. He places all things in lines. There is a thick heavy green yellow congestion from his nose and his ears become very hot when he has a cold, this is always accompanied by a copious mucous congestion in his chest. The seasons of spring and autumn are his worst times.
A three year old male child comes to clinic in March 2005 with continuous colds and discharges from the ear and nose. He runs from one cold into another continuously with perhaps a break of two to three days in between. He is fully vaccinated and has had measles. He has been diagnosed as autistic by a specialist that was organised by the family G.P. He cannot or will not talk and only points and grunts and makes noises; he has never said a word. He does not participate in any games and even though he is inquisitive he has a very poor concentration span that inhibits him from learning anything in detail. No fantasy play is ever undertaken and a diagnosis of hyperactivity has also been given by the same behavioural specialist. The only thing he likes to do continuously is to place things like toy cars in a line. He places all things in lines. There is a thick heavy green yellow congestion from his nose and his ears become very hot when he has a cold, this is always accompanied by a copious mucous congestion in his chest. The seasons of spring and autumn are his worst times.
In the clinic he refused to make eye contact. There were some squeals and grunts to go along with his pointing if he wanted a particular toy but that was all. The screaming and grunting was extraordinarily loud and his restlessness was obvious; his agitation at being in the consultation room was also obvious. When it came time to take his photos he continually refused, despite heavy coaxing from his grandmother. When she tried to put him in a particular position needed for a photo he would scream, arch his back and hit. This behaviour was repeated for each photo. In the end, the photos became almost useless so I had to rely on obvious physical facial features that I could see with my eyes.
The child’s mother is also autistic, but I am unsure as to whether this has been diagnosed by an authority or whether it is just supposition by the family based on her behaviour. Either way, he lives with his father because the mother does not feel competent in raising him, a duty the father shares with the boy’s paternal grandparents. Both the grandparents and the boy’s father seem deeply caring and concerned for his well-being.
His appetite is good, his favourite food is apples but not to the point of a craving.
At this stage without the method of facial diagnosis I would feel lost in where to go next. Because he is only three years old, autistic and suffering from colds he cannot contribute, and it was difficult getting any more information other than ‘he is a lovely child’ from his grandmother. With limited information, facial analysis becomes paramount in deciding the remedy.
His major facial features include a straight hairline, a full bridge, large round eyes, spaced teeth and full lips. These features mean sycosis is the dominant miasm. In this method I prefer to use colours to signify genetic miasmatic inheritance rather than pathology for reasons that are too lengthy for this article. Suffice to say that sycosis means he is from the red colour group
FACIAL ANALYSIS OF THE CASE
To analyse a face it is important to take five (6) good quality photographs. Three are front on, showing a non-smile, a smile (with teeth) and a hairline plus a profile from both sides. Due to his autism, general restlessness and his young age the photos obtained do not show adequately his dominant features. The following sketches are an artist’s impression of the boy, highlighting the shape and structure of his features. Knowing how to interpret facial features gives an accurate determination of the dominant miasm and will lead to successful remedy choices.
(6) I now suggest seven photographs and often as many as ten or more are required for children who cannot sit still
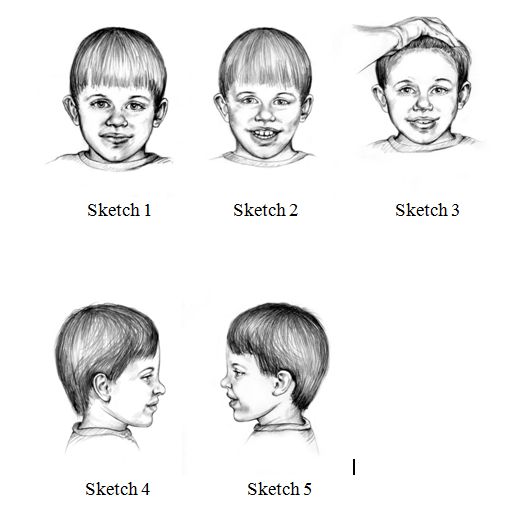
- Sketch 1 – large eyes, full lips, ball shaped nose, ears that stick out, cleft in the chin
- Sketch 2 – spaced teeth, gums show
- Sketch 3 – straight hairline
- Sketch 4 – straight forehead, straight (full) bridge of nose
- Sketch 5 – straight forehead, straight (full) bridge of nose (confirmed on both profiles)
A chart is drawn to highlight the miasmatic dominance
| YELLOW (psora) 2* | RED (sycosis) 10* | BLUE (syphilis) 1* |
| Eyes shapeChin position | Eyes – sizeLips – sizeNose – shapeEars – position
Chin – cleft Teeth – spaced Gums – show Hairline – shape Forehead – shape Bridge of nose – shape |
Hairline – height |
* These features have been reworded and some added for this 2013 publication. In reviewing the sketches, 2 psoric and 1 syphilitic feature have been identified – this identification does not change the final analysis but is an example of the development of the HFA system and the accuracy required to identify every facial feature.
This boy has only (*mainly) sycotic features. This is extremely rare to find in one patient. Almost all people have a mix of the three primary miasms (psora, sycosis and syphilis) as part of their genetic makeup with dominance showing in one primary miasm or mixed miasm. An evaluation of all the facial features will show which miasm is dominant.
My repertorisation included
- Generals; Change of weather aggravates
- Nose; Discharge; colour; greenish
- Lungs; Inflammation; bronchial
- Generals; Cold; tendency to take
I did not include any mental rubrics because I did not feel I sufficiently understood what was going on in this child’s mind, as well as the fact that all the mentals were characteristic of autism and therefore too ‘common’.
The major red (sycotic) remedies in my repertorisation included Dulcamara, Rhus Toxicodendron and Sepia. Because of the greenish yellow discharge combined with the observation that spring and autumn were his worst seasons, Dulcamara 30C daily was chosen.
Follow up
After three months
Coughs and colds have vanished and he is now talking in sentences of up to seven or eight words per sentence. This occurred three weeks into taking the remedy. A few weeks later he started talking in long well formed sentences and has not stopped talking since. Occasionally he has a very mild discharge from his nose but it has never turned into a cold. He has a problem with mild constipation which has not altered. When he does have this mild nasal discharge it is drier than previously and it has no specific colour.
Both his father and grandmother state that he is talking a lot around the house even though he is quieter in unfamiliar surroundings such as the clinic. His concentration span has improved dramatically. His father claimed that in the past he could never read any type of book to him, no matter how short, where as now he will sit through an entire children’s book listening while his father reads to him. His father states that he is now ripping through books. He has grown in the last three months and his doctor – the original behavioural specialist – has stated openly that she is questioning her original diagnosis of autism. In the clinic his behaviour is good and he smiles and says both hello and goodbye to me. His father is almost in tears with gratitude as he had given up any hope of having a normal relationship with his son.
Dulcamara 30C daily – continue
After four months
He is still continuing to improve mentally and is now singing to himself and instigating conversations. He is very happy and does not place things in lines. He also enjoys fantasy play. He still has not had one cold.
After seven months
Has not suffered with colds but has an occasional runny nose. His talking continues to improve although his speech is still slightly delayed for his age so he has commenced speech pathology. Tests conducted by his behavioural specialist place him just above the cut-off point for autism and he is no longer considered eligible for “special help” by Human Services. He is asking questions and making eye contact. At kindergarten he has lots of friends and is playing football. There is no hitting (there was in the past) or signs of frustration and he talks to his friends nicely and understandably. He has become toilet trained and continues to develop his fantasy play.
If he doesn’t take Dulcamara 30C daily he gets annoyed, everything becomes hard and he becomes run down very quickly. Continue Dulcamara 30C daily. (see footnote on potency)
After one year
Still doing well – going to a normal school and has stopped the remedy. The father is annoyed that he couldn’t get a financial refund from the special school after his son was re-diagnosed “not autistic”.
After three years (phone follow up)
He is a normal boy and loves to play team sports (football). He has not needed any more of the remedy.
Comment on posology
Because of his continuous improvement, the prescription of 30C daily was still justified. His father was under instructions that should any of the cold signs and symptoms return or his demeanour or development regress, they must make contact with me immediately.
Footnote on potency.
I am sure there are many questions regarding the continuance of the 30th centesimal potency rather than moving up to a 200th or 1M. My reasoning is based on the simple fact that the 30th continues to work. The fact that this boy continues to improve means his vital force still needs and accepts the remedy in this potency; if this were not the case, improvement would cease and he would slip back. Each prescription is given with the sound knowledge that should old symptoms return, the Dulcamara is to be discontinued and a new consultation conducted. This is based on Hahnemann’s guidelines for LM potency use, which is applicable in this case as it relates to any long term prescription. Many times in the past I have ruined a case by trying to turn ‘excellent’ results into ‘even better’. It is a natural human impulse to go for more, but I strongly advise against it. When a medicine is working well – do not be in a hurry to change it. It is true that he slips back when the remedy is not given for a day or so, but this should not be interpreted as an incorrect prescription, rather, it is merely a display of how entrenched his affliction is and of how important it is to see a case through the eyes of management and balance rather than cure. To the suggestion that perhaps it is the wrong remedy – which seems to be the standard retort to any prescription that does not fix a problem first go, I reply; the wrong remedy does not achieve the wonders this remedy has achieved. Again I reiterate, do not change what is working and always work within the patient’s time frame, not your own. Do not try and hurry the process along, or push it harder, the symptoms are the guide. In this case, slow and gradual improvement is how this boys system works and I must follow that lead. To do any different would show ignorance on my part.
Further information about Grant Bentley’s research and his books can be found on the Victorian College of Classical Homœopathy website http://www.vcch.org/miasm.html and the Soul & Survival website http://www.soulandsurvival.com/
Contact details
PO Box 804
Mt Eliza
Victoria
Australia 3930
Email [email protected]
+613 9873 0567


Hi Grant,
Can you point us to the source of the statement attributed to Boenningheusen that there is no accurate way of determining one miasm over other?
Also, you mention that your ideas resonate with Hahnemann’s. However, Hahnemann considered Miasms from the etiological point of view?
Please shed some light on these seeming inaccuracies.
Surabhi
Regrading the selection of rubrics, why did you choose Lungs; Inflammation; bronchial over Chest, catarrh?