What Are Cystic Hygromas?
Cystic hygromas are abnormal growths that usually appear on a baby’s neck or head. They consist of one or more cysts and tend to grow larger over time. This disorder most often develops while the baby is still in the womb. However, a cystic hygroma can also appear after birth. Cystic hygromas are fluid-filled sacs caused by blockages in the lymphatic system Approximately half of all fetuses with a cystic hygroma have chromosomal abnormalities. A baby is unlikely to have a chromosomal abnormality if the cystic hygroma goes away by week 20.Cystic hygromas can also increase the risk of miscarriage and may even be life-threatening.
Causes of Cystic Hygromas
Cystic hygromas can develop due to genetic disorders or environmental factors. One or more growths may be present at the time of diagnosis. Common environmental causes of cystic hygromas are:
- viral infections passed from the mother to the baby during pregnancy
- exposure to drugs or alcohol during pregnancy
Cystic hygromas are seen more often in infants with genetic diseases. They are particularly common in infants with chromosomal abnormalities.
Some genetic conditions associated with hygromas include:
Turner’s syndrome — where female children have one X chromosome instead of two
- Trisomy 13, 18, or 21 — conditions where children have an extra copy of a chromosome
- Noonan syndrome — a disorder caused by a mutation (change) in one of seven particular genes
Symptoms of Cystic Hygromas
Cystic hygromas may not be noticeable when the baby is born. They can become visible as they grow larger and the child gets older. Cystic hygromas will usually appear by the time the child is 2 years old. The main symptom is the presence of a soft, spongy lump. This lump most commonly appears on the neck. However, a cystic hygroma can also form in the armpits and groin area. Cystic hygromas range in size from smaller than a quarter to as large as a baseball. Larger growths may interfere with movement or cause other difficulties.
Diagnosing Cystic Hygromas
Amniocentesis if a cystic hygroma is suspected during an ultrasound. An amniocentesis can check for genetic abnormalities in your fetus. Other tests will be used to make a diagnosis if cystic hygromas aren’t found until after the child is born. These include:
- chest X-ray
- ultrasound
- CT scan
Treating Cystic Hygromas
Cystic hygromas aren’t treated while the baby is in the womb. A cystic hygroma is usually treatable if it’s found after birth. The first step of treatment is surgery. The entire growth must be removed to prevent it from coming back. In some cases, however, doctors may not want to remove large cystic hygromas. Since these growths usually aren’t cancerous, doctors won’t want to get rid of them if there’s a risk of damaging any healthy tissue.
Instead, other techniques may be used to shrink large cystic hygromas:
- Sclerotherapy — where medicine is injected into the cyst
- chemotherapy
- radiation therapy
- steroid medication
These methods aren’t very effective in treating small cystic hygromas, but they may be useful in shrinking large growths. Once the growth is small enough, it’s easier to remove surgically. You should never try to puncture or drain a cystic hygroma yourself. It may cause severe bleeding and lead to an infection.
Prognosis
The main potential complications of cystic hygromas are:
- recurring growths
- bleeding
- infection in the affected area
- damage to muscles, nerves, or tissues from surgery to remove the hygroma
The outlook for babies with cystic hygromas is generally good if the growths appear after birth. This is especially true if the growths can be completely removed. If they can’t be removed, cystic hygromas may return or spread to other areas.
A CASE of CYSTIC HYGROMA
19/6/2015
Patient came for consultation. 1st prescription was based on the below said symptoms:
Right sided Cystic Swelling + Increased Head sweat+ Milk Aversion + constipated + Infant
- Thuja 200=1 dose=1/2-0-1/2
- Silicia 200= 30doses=1-0-0
29/6/2015
1st follow up. Swelling increased in size. Patient mother not happy. They wanted to consult a Paediatric surgeon and get a second opinion. I agreed. I Gave
- Kali Mur 6x=2 drachm tab=1-0-1
14/7/2015
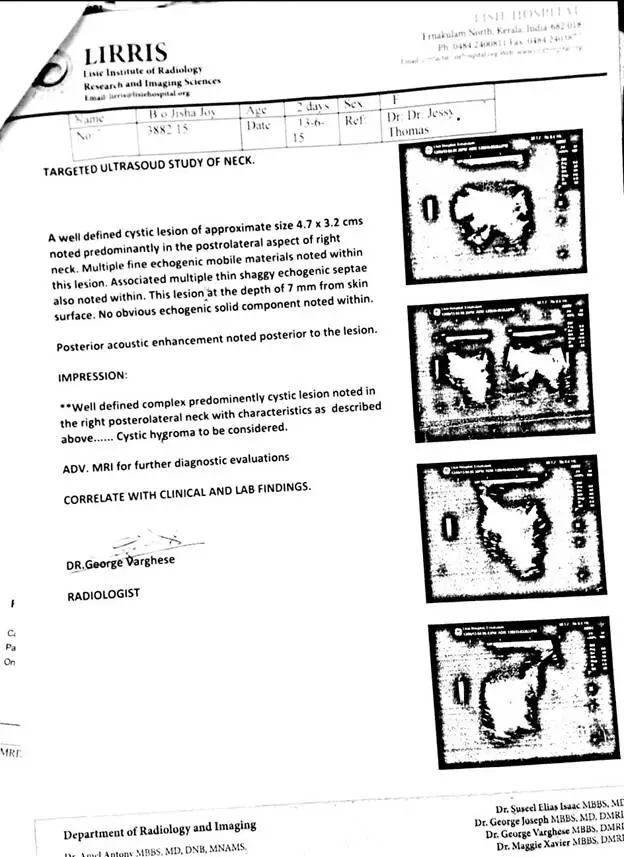
Patient went to a paediatric surgeon who gave her an Injectin of Bleomycin and aspirated 45cc of straw fluid. Also gave Taxim Syrup+Paracetamol syrup+Zincovit drops and advised follow up after 1 month.
The swelling shrunk and patient was discharged.
By evening of the same day the swelling started increasing in size.
15/7/2015
Patient was brought back to me and parents explained what was done with reports (attached).Meanwhile parents had discontinued what I had prescribed. Patient had pain in the region of the swelling after the injection was given. I gave:
- Hypericum 1M=1 dose=1/2-0-/12
20/7/2015
Pain gone completely after Hypericum on the same day it was given.
They wanted me to look into the case again. Prescribed as below (no change made).
- Silicia 200= 30doses=1-0-0
- Kali Mur 6x=2 drachm tab=1-1-1-1
- Sambucus 6c=2 drachm drops=1 drop 3 hourly for nose block=for 2 days
31/7/2015
Patient developed red itching blotches on face and legs. Acute prescription given. Swelling size started reducing.
- Sulphur 0/3=1 dose
- Thuja 30=2 drachm drops=1 drop 3 hourly
- Caleborol powder=External=after bath
12/8/2015
Skin extremely dry and patient was getting irritated. Swelling further reduced in size.
- Rhus tox oil+ Arnica oil=External=before bath
20/8/2015
White patches started appearing in skin. Swelling reduced by more than 80%. Itching reduced but slightly persisted. I gave:
- Silicia 200=30 doses=1-0-0
- Calc Phos 6x=2 drachm tab=1-1-1
10/9/2015
Swelling not seen anymore. White patches were fading. Slight itching still persists but no troubling the patient. Skin dryness still. Did not stop medicine. Gave:
- Silicia 200=30 doses=1-0-0
- Calc Phos 6x=2 drachm tab=1-1-1
- Rhus tox oil+ Arnica oil=External=before bath
- Caleborol powder=External=after bath
2/10/2015
Swelling not seen. A few white patches only seen. Skin dryness and itching still seen.
- Rhus tox oil+ Arnica oil=External=before bath
29/10/2015
No swelling. Parents came to buy Calebrol powder, since it was finished.
19/11/2015
Swelling not seen at all and no mark of swelling as well. White patches still present but much reduced. Itching still present slightly.
Stopped Silicia
- Kali mur 6x=2 drachm tab=1-0-1
- Calc Phos 6x=2 drachm tab=1-0-1
- Rhus tox oil+ Arnica oil=External=before bath
The patient has been coming to me for acute complaints since 19/11/2015 and has not had any recurrence of hygroma for the last 15 months.
Images:

Total Duration of Treatment: 5 months
From 19-6-2015 to 19-11-2015




Sir.. My baby is having cystic hygroma since birth on right arm.. We are giving homeopathic medication for last 1 year.. Still no change is there.. Can u help us??