Luisa Ferla, Aishwarya Madhusudhan, Seema Mahesh
1Azienda sanitaria locale TO4 di Ciriè, Chivasso e Ivrea,
Department of Ivrea, Chivasso, Italy
Email: [email protected]
2 Government Homeopathic Medical College and Hospital,
Bangalore, India
3Taylor’s University School of Medicine
Malaysia
4Centre for Classical Homeopathy
Bangalore, India
email: [email protected], [email protected]
Keywords: Neurological diseases, case series, Homeopathy, Trigeminal neuralgia
Background
Neuroanatomy
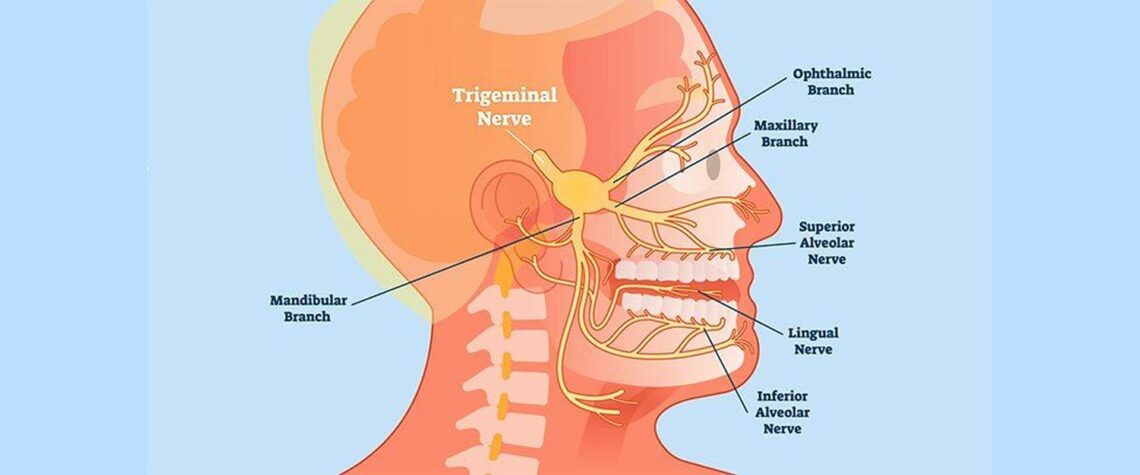
The trigeminal nerve (fifth cranial nerve) is the largest and most complex among the cranial nerves; providing primarily, sensory and motor functions of the face, specifically conducting sensations like touch, temperature and pain.
The nerve further divides to emanate three branches viz. ophthalmic, maxillary and mandibular, which meets at the trigeminal ganglia located in trigeminal fossa (Meckel cave) in the cranial cavity.
The ophthalmic and maxillary divisions provide sensory innervations to the eye, portions of nasal cavity, sinuses and maxillary teeth respectively. Whereas the mandibular branch provides both sensory and motor functions, innervating mandibular teeth, buccal mucosa, anterior two-third of tongue with sensory functions and muscles of mastication with motor function.1,2
The neuropathic pain involving the sensory divisions of the trigeminal nerve characterizes the condition trigeminal neuralgia (TN). TN is classified by International Classification of Headache Disorders, third edition (ICHD-3, 2018)3, as classic TN (cause attributing to vascular compression), secondary TN (attributing to tumor compression or other underlying disease like multiple sclerosis) and idiopathic TN (cause unknown).
Etiology
As mentioned, most cases of TN are ascribed to trigeminal nerve root compression including meningioma, epidermoid cyst, acoustic neuroma and rarely aneurysms. In the later years, the development of neurovascular theory evidenced, arterial and or venous compression of the nerve are not far from causing TN1, and is accepted as the most common cause of TN.
This mechanism is also termed ‘neurovascular conflict’4 which steers demyelination of the nerve, thus conducting anomalous impulses. Likewise a minority of the cases with TN are considered to have multiple sclerosis as a risk factor.5 While the exact pathogenesis of TN still remains contentious.
Incidence
The incidence of TN, considering different statistics, affects 4 to 13 cases/100,000 per year. Females are affected more than the males, with the ratio of 2:1. The incidence increases with age > 50, few cases are reported under the age 40 and rarely in children.2
Clinical course and Diagnosis
TN is distinguished by sudden paroxysmal unilateral facial pain with an episode of exacerbation and remission. This pain is distributed along the area innervated by one of the three divisions of the nerve and is generally evoked by trivial stimulation of pain zones called “trigger points”.1
This routinely observed pain pattern accounts for clinical diagnosis of TN. Eventually this intermittent paroxysmal pain or typical TN (TN1), progresses to a more constant pain or atypical TN (TN2), requiring further neuroimaging interpretation for a precise diagnosis. Whether the progression of TN1 to TN2 is a continuous process or belongs to different entities is still unclear.2
Therapy
The first line treatment for TN lies in prescribing anti-epileptic drugs (oxcarbazepine and carbamazepine co-administered with gabapentin etc.), neuroleptics, muscle relaxants6 and recent advancement – the use of botulinum toxin A injections;7 although effective, significant cognitive side effects have been recorded.8,9
According to the guidelines set forth by the European Academy of Neurology10, at least 2 drugs should be administered and evaluated before invasive techniques (microvascular decompression (MVD), Deep brain and motor cortex neuro-modulatory stimulation, Percutaneous approaches like radiofrequency ablation, glycerol injection, balloon compression, radiosurgery) are instituted,11 and studies suggest more than 50% of TN patients eventually had some kind of surgical procedure with postoperative complications (chemical meningitis, ipsilateral hearing loss, facial palsy, cerebellar injuries etc.), especially in the elderly.12,13
The homeopathic choice
Homeopathic therapy provides an integrated outlook for the pathology, wherein, the patient is treated as a whole considering his past and present illnesses, of not only the physical level, but also the mental-emotional level. There are homeopathic studies conducted under neurological pathologies which have further proved its efficacy in conditions such as TN.14,15
Methods
The objective of the study was to prospectively analyze the outcome of therapeutics under individualized classical homeopathy in adults with TN, who did not respond to conventional treatment under anti-epileptics and or invasive techniques for TN.
Eligibility criteria: Patients diagnosed of TN, who were non responders to pharmacological and/or surgical treatment. The recruitment was consecutive, and the study was conducted between November 2009 and November 2017.
Results
The five-cases included in the study were all female with TN, aged between 44 to 77 years old (Avg age: 64 years). The cases were clinically diagnosed; among which, one case had neuroimaging interpretation result positive. All the five patients in the study are treated with individualized classical homeopathic therapy16, along with the on-going conventional treatment for TN and other co-morbidities, as mentioned in the case series.
Further, to avoid bias arising out of the natural course of the condition involving periods of remission, the cases incorporated clear reporting of the follow-up under homeopathic treatment, for an average of one to five years. Additionally, dietary or supplementary restrictions were not made, although the cases involved did not resort to these interventions.
Case 1
History
A 68-year-old female developed TN (right maxillary branch) for the last 2 years, with steady worsening of symptoms. Patient was on Pregabalin 50 + 75 mg/day. Brain NMR and panoramic dental Rx not meaningful. No other significant anamnestic history except moderate hypertension, well controlled by ongoing therapy.
Table 1. Case 1. Details of treatment
| DATE | SYMPTOMS | PRESCRIPTION |
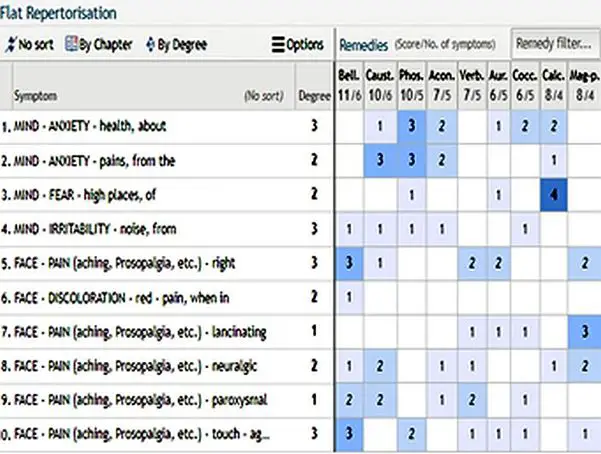
| 03/2015 | · Neuralgic face pain, paroxysmal and lancinating on right side of face, with red discoloration of the affected area, and pain aggravated by touch.
· Psychologically anxious about health due to the pains, irritability from noises and fear of heights. |
Belladonna 200CH, 3 drops /day (till 3 drops x 3/day if pain increases). |
| 06/2015 | · Improvement of neuralgic symptoms.
· Pain in trigger points reduced. · Pregabalin dosage reduced to 25 mg x 2/day |
Continues to take Bell 200CH for 2 months. |
| 10/2015 | · No more neuralgic pain
· Stopped Pregabalin 3 months ago |
Placebo |
| 10/2016 | · Reappearance of neurological symptoms | Bell 1M 3 drops x 3 for one month, followed by quick remission of symptoms. |
Case 1. Repertorization
Outcome
Patient is doing well (01/2017); she has stopped taking the remedy anymore. Hypertension is better. Generally better and psychologically better, anxiety reduced.
Case 2
History
A 74-year-old female suffering from TN since 2015, after the death of her husband (2014) and sister, following a depressive state and anxiety for her daughter’s health. The pain was there since a year, around right eye area, triggered by even slight touch.
The neurological examination reveals: de-ambulation still possible without support, with mild hypertonus in lower left limb, mild left pyramidal deficiency, pain triggered at the point of the I branch of right trigeminus. Other medical history includes hypertension outbreaks (right pons ischemia – 2010), hysterectomy for uterine cancer at age of 45, currently on ticlopidine, statin and antihypertensive therapy, MNR of spine revealing multiple disc protrusions and EMG lower limbs negative, with walking difficulties.
Table 2. Case 2. Details of treatment
| DATE | SYMPTOMS | PRESCRIPTION |
| 02/2016 | · Ailments from loss of loved ones
· No repertorization has been done, the remedy was prescribed on the basis of emotional symptoms, given that the neuralgic pain started shortly after the death of the spouse. |
Ignatia Amara 200CH, 3 drops |
| 07/2016 | · Total remission of neuralgic symptoms after one month of therapy.
· Emotionally better |
Placebo |
Outcome
Patient was doing completely well for about two months, followed by reappearance of the symptoms, which resolved after repetition of the remedy. Currently discreet wellness, except asthenia. No more pain at trigger points. Psychologically patient is doing well.
Case 3
History
A 44-year-old female developed TN since 6months, with short-lasting pain in the right maxillary region. She was on pregabalin 75 mg x 2/day, with discrete results, but symptoms had again accentuated after attempting to reduce the dosage. The patient is a reserved and responsible person. She is an English teacher and had been suffering emotionally from tensions at work. Personal history of endometriosis (waiting for surgery), occasionally heartburn, flu-vaccination yearly for the last 3 years.
Table 3. Case 3. Details of treatment
| DATE | SYMPTOMS | PRESCRIPTION |
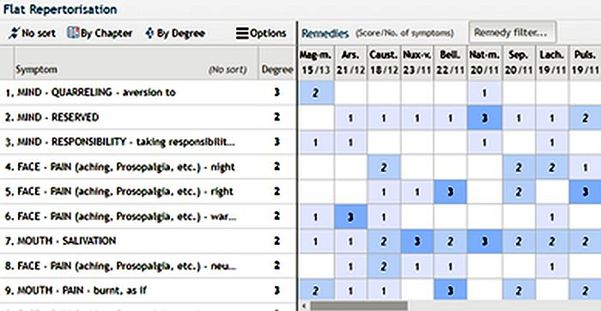
| 11/2009 | · Face pain, right side, triggered by chewing and touching, <during the night and >warmth
· Profuse salivation of mouth during pain, with pain as if burnt in the mouth. · Psychologically intolerant to quarrelling, reserved and takes responsibility too seriously. |
Magnesia Muriatica 200C, drops 3 x 3/day, associated with the ongoing treatment (pregabalin 75 mg x 2) |
| 05/2010 | · She refers to 90% improvement, just feels mild annoyance in the right maxillary region, totally bearable and short-lasting.
· Stopped pregabalin one month ago, after progressive reduction. · Has been operated for endometriosis. |
3 x 2 drops/day of Mag-m LM1 |
| 11/2010 | · Neuralgic symptoms have totally disappeared, not on any medications since 3months.
· Complains of heartburn and burping and has been taking lansoprazole prescribed by the treating physician. |
Repetition of remedy (Mag-m 3 x 2 LM1) for a few days. |
Case 3. Repertorization
Outcome
After one year (05/2011), there was reappearance of neuralgic symptoms which resolved after repetition of the remedy; meanwhile the gastritis was better. Last follow-up was 5 years later (01/2014), where patient had only sporadic flare-ups of symptoms which always resolved with repetition of the remedy.
Case 4
History
A 77-year-old female developed TN (right mandibular branch) starting at the age of 20. Subjected to intervention of Gasser ganglion neurolysis many years ago, without benefit. Treated for years with carbamazepine (not effective), subsequently suspended due to leukopenia, and then treated with pregabalin + amitriptyline, stopped recently for intolerance and poor effectiveness of the drugs. Not on any other medications. Now pain spreading to the maxillary and ophthalmic branch occasionally. Psychologically she is very anxious.
Table 4. Case 4. Details of treatment
| DATE | SYMPTOMS | PRESCRIPTION |
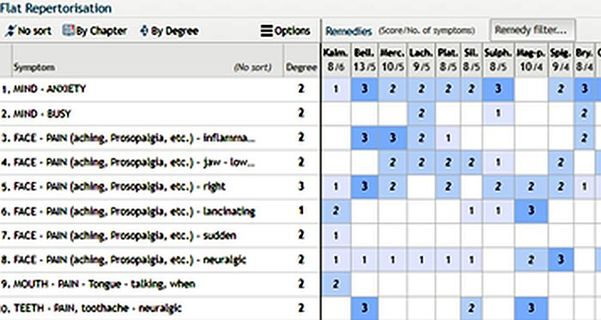
| 09/2016 | · Face pain, right side, sudden and neuralgic extending to lower jaw, teeth and tongue.
· Anxiety about heath |
Kalmia 30C 3 x 3 (drops) |
| 11/2016 | · Slight improvement in symptoms, she can speak a little better, psychologically better. | Kalmia 30C 3 x 3 (drops) |
| 07/2017 | · Still complains of burning tongue and gum pain, neuralgic pain of face is better. | Kalmia 30C 3 x 3 (drops) |
Case 4. Repertorization
Outcome
Follow-up after 11 months (10/2017), there is further slight improvement with ongoing therapy, Kalm 30C 3 x 3 (drops). She claims that homeopathic therapy has been the only one in all these years to have alleviated her pain.
Case 5
History
A 57-year-old female developed TN. During the last six months she has constant burning neuralgic pain involving the left side of face, occasionally in periorbital region with downwards extension, sometimes in maxillary region and the ear. Dental/ORL/OCL insignificant findings, atypical facial pain? or atypical TN? She is a primary school teacher, very responsible and careful in her work, often stressed. Very attached to the family and worries excessively about all of them. Complains of some difficulty in concentrating and slight memory weakness. Good health level from the general point of view, she seldom takes medicines, she generally takes homeopathic treatment. Menopause at age 53 with some complaints, relieved by homeopathic remedy Causticum.
Table 5. Case 5. Details of treatment
| DATE | SYMPTOMS | PRESCRIPTION |
| 10/2013 | · Face pain left side, < cold exposure, > lying on affected side
· Ailments from disappointment and anticipation, dictatorial, weakness of memory. Sleeplessness from excessive thoughts, sleep unrefreshing. |
Spigelia [sb1) |
| 02/2014 | · Neuralgic symptoms improved; she continues to complain memory impairment. Other psychological symptoms better. |
Case 5. Repertorization
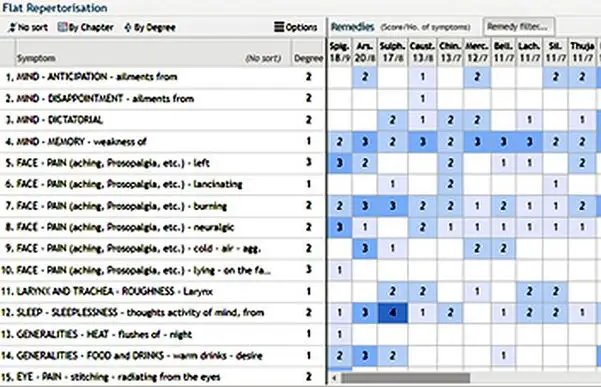
Case 5. Outcome
After one year of treatment, patient is doing well. Recent follow-up (October 2017), facial pain never relapsed, memory weakness and difficult concentration is better (she has retired, but still helps her colleagues at school; she has a very active life).
Discussion
TN is a debilitating condition with unpredictable refractory periods, with linking episodes of intense facial pain, calling forth high dosage drugs for pain relief. The aftermath of such an approach in handling the condition, results in patients suffering from disabling adverse side-effects.
This is evidenced in one of the cases presented here, where the patient on anti-epileptic drugs for many years, was switched between further drugs of the same sort, either due to lack of efficacy and or intolerance, causing low WBC count in this particular case (case 4. History).
The homeopathic system of medicine provides an integrated approach for disease conditions, where the focus of treatment is not alone the primary pathology, but also the general well- being of the patient.
Even in seemingly rare conditions such as TN, the disease presentation is diverse in each patient, and through homeopathic remedies these varied indications are easily addressed. Furthermore, the psychological implications in cases like TN play a major role as the patients anticipate the upcoming attacks, leading to depression and anxiety17, a challenge to conventional management.
In these cases, the patient suffering from neuralgic pain of right maxillary branch subsequently suffered from anxiety due to strong pains, with an added psychological factor like irritability which was often triggered by external noises (case 1).
This case was prescribed Belladonna, a homeopathic remedy with indications such as sudden and intense pain accompanied with intense emotions like irritability, rage, fear and anxiety.18 Following the prescription, the neuralgic pain as well as the anxiety and irritability simultaneously got better.
Thus, the patient’s over-all status was addressed considering the totality of symptoms. Similarly in the case where Ignatia amara was prescribed, the patient developed TN shortly after the death of her husband which followed depression and anxiety (case 2). Here the remedy was administered mainly considering the grief and romantic disconnection as the causative factor resulting in neuralgic facial pain. Ignatia is a remedy indicating ailments arising out of grief concerning loss of loved ones.
The remedy also has its action upon neuralgic pains especially around the face and eyes.18 Likewise, other cases are treated considering the totality of symptoms and thus stands by the individualized classical homeopathic rules of prescription.16
As previously stated, the sequence of TN attacks is difficult to elicit and the patients are often put on aggressive conventional management without any time frame. These cases under homeopathic treatment eventually remained free of any medications, and the reappearance of facial pains were less intense and much easier to manage with lesser intervals compared to their first visit. A controlled study is further required to prove homeopathic significance in neuropathic conditions like TN.
Conclusions
The case series presented here illustrates substantial improvement of the neuralgic facial pains of TN through individualized classical homeopathic treatment, and at the end of the treatment the patients remained medication free. Thus, homeopathic therapy may constitute a valid alternative in the treatment of neuralgic conditions and merits further investigation.
References
- Yadav YR, Nishtha Y, Sonjjay P, Vijay P, Shailendra R, Yatin K. Trigeminal Neuralgia. Asian J Neurosurg. 2017;12(4):585. doi:10.4103/AJNS.AJNS_67_14
- Kikkeri NS, Nagalli S. Trigeminal Neuralgia. StatPearls. Published online April 7, 2021. Accessed July 10, 2021. https://www.ncbi.nlm.nih.gov/books/NBK554486/
- The International Classification of Headache Disorders – ICHD-3. Accessed July 1, 2021. https://ichd-3.org/
- Maarbjerg S, Wolfram F, Gozalov A, Olesen J, Bendtsen L. Association between neurovascular contact and clinical characteristics in classical trigeminal neuralgia: A prospective clinical study using 3.0 Tesla MRI. Cephalalgia. 2015;35(12). doi:10.1177/0333102414566819
- A T, L P, V C, et al. A dual concurrent mechanism explains trigeminal neuralgia in patients with multiple sclerosis. Neurology. 2016;86(22):2094-2099. doi:10.1212/WNL.0000000000002720
- E G, JG C, GW Z. Trigeminal neuralgia: An overview from pathophysiology to pharmacological treatments. Mol Pain. 2020;16. doi:10.1177/1744806920901890
- A R, G J. The Use of Botulinum Toxin A in the Management of Trigeminal Neuralgia: a Systematic Literature Review. J oral Maxillofac Res. 2020;11(2). doi:10.5037/JOMR.2020.11202
- G DS, G DS, C L, et al. Real-world effectiveness and tolerability of carbamazepine and oxcarbazepine in 354 patients with trigeminal neuralgia. Eur J Pain. 2021;25(5):1064-1071. doi:10.1002/EJP.1727
- V T-P, G L, J R, AG O, JM Z, R C. Adverse effects of anti-epileptics in trigeminal neuralgiform pain. Acta Neurol Scand. 2018;137(6):566-574. doi:10.1111/ANE.12901
- L B, JM Z, J A, et al. European Academy of Neurology guideline on trigeminal neuralgia. Eur J Neurol. 2019;26(6):831-849. doi:10.1111/ENE.13950
- MR J, I U, KP E, et al. A Comprehensive Review of Trigeminal Neuralgia. Curr Pain Headache Rep. 2019;23(10). doi:10.1007/S11916-019-0810-0
- P A, B L, G L, J W, AT B. One Hundred Eleven Percutaneous Balloon Compressions for Trigeminal Neuralgia in a Cohort of 66 Patients with Multiple Sclerosis. Oper Neurosurg (Hagerstown, Md). 2019;17(5):452-459. doi:10.1093/ONS/OPY402
- R Y, C W, C Q, et al. Study on the Therapeutic Effects of Trigeminal Neuralgia With Microvascular Decompression and Stereotactic Gamma Knife Surgery in the Elderly. J Craniofac Surg. 2019;30(1):E77-E80. doi:10.1097/SCS.0000000000004999
- YN M, F M, A M, A S, K M. Individualized homeopathic treatment of trigeminal neuralgia: an observational study. Homeopathy. 2007;96(2):82-86. doi:10.1016/J.HOMP.2007.02.006
- TE W. Homeopathy in multiple sclerosis. Complement Ther Nurs Midwifery. 2003;9(1):5-9. doi:10.1016/S1353-6117(02)00105-1
- Vithoulkas G and Tiller W. The Science of Homeopathy.; 2009.
- JM Z, J W, M M-W, N P, SH P. Evaluating the impact of trigeminal neuralgia. Pain. 2017;158(6):1166-1174. doi:10.1097/J.PAIN.0000000000000853
- J.T.Kent. Lectures on Homeopathic Materia Medica. B.Jain Publishers (P) LTD; 2002.


