Cervical cancer continues to be a major public health issue, affecting many middle-aged women. Ten years ago, cervical cancer was ranked as the third most common cancer among women worldwide. Today, it remains the most common cancer in women in developing countries.
First, let’s go over the different stages of pre-cancerous cervical changes:
ASCUS – atypical squamous cells of undetermined significance.
CIN1, CIN 2, CIN 3 – Cervical intraepithelial neoplasia
Low-grade neoplasia (CIN 1 or LSIL) refers to dysplasia that involves about one-third of the thickness of the epithelium.
CIN 2 (HSIL) refers to abnormal changes in bout one-third to two-thirds of the epithelial layer.
CIN3 (HSIL) – severe dysplasia describes a condition, that affects more then two-thirds of the cervical epithelium.
Risk factors for Cervical Cancer
Cervical intraepithelial neoplasia (CIN) is typically a progression of an infection with the Human PapillomaVirus (HPV). The virus is spread through sexual skin to skin contact, which means condoms are not always effective. Most countries do not include HPV testing as part of a STI test panel, and many individuals remain asymptomatic, which allows the virus to spread very quickly. In Canada, 75% of sexually active adults will have had an HPV infection at least once in their lifetime.
There are over 100 strains of HPV, some of which (HPV 16 and HPV 18) are much more likely to infect the reproductive tract in women and cause CIN.
In most cases, HPV infections will clear out on their own, however this often depends on having a healthy immune system. In some cases, the infection lingers, and can eventually progress to cervical cancer. Other risk factors include:
- Having unprotected sex with many partners
- Smoking
- Having multiple full-term pregnancies
- Having a weakened immune system
- Long term use of oral contraceptives
- Chlamydia infection
How is Cervical Intraepithelial Neoplasia (CIN) diagnosed?
Since CIN usually does not cause any symptoms, a Pap smear is needed to find abnormal cells. If the Pap test is unclear or abnormalities are found, the next step might be a colposcopy to examine the cervix and surrounding structures under a microscope.
How is Cervical Intraepithelial Neoplasia (CIN) treated?
In the case of low-grade CIN, treatment usually is not required. In the case of moderate and severe CIN, treatment focuses on the removal of abnormal cells that might become cancerous.
Removal (resection) procedures include:
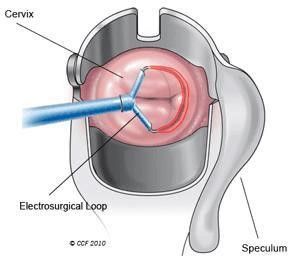
- Loop electrosurgical excision procedure (LEEP) – This technique uses a small, electrically charged wire loop to remove tissue
Side effects of LEEP include:
- Bleeding
- Pelvic infections
- Cervical stenosis
- Increased risk of miscarriage and preterm birth
- In 10 cases, LEEP does not completely cure the problem
2. Cold knife cone biopsy (conization) – This is a surgical procedure in which a cone-shaped piece of tissue containing the lesion is removed.
3. Hysterectomy – removal of the uterus
———————————————————————————————————————–
A Case of Cervical erosion, CIN1-CIN 2, HPV 18, 52
First consultation on 18 of May 2020
Female patient, Medical doctor, 33 years old came to my clinic, complaining of Cervical erosion, CIN lCIN ll, HPV 18, 52; PCOD 28-35 days periods, nodules face acne, hair loss, anxiety.
Medical anamnesis
The Patient’s PAP smear on 28/08/2019 showed ASCUS. HPV 18 and 52 were positive. Colposcopy with biopsy was done on 25/09/2020. Cervical ectropion with CIN1-CIN2(LSIL-HSIL) was described in the histopathology report.
Patient was advised to undergo LEEP procedure. She preferred to make some healthy modifications to her life and then to be rechecked. From September 2019 till May 2020, she was doing regular exercises, ice baths, magnotherapy, stopped eating sweets.
In May 2020 her PAP smear result showed CIN 1 (LSIL) which is worse than before (ASCUS). At this point, her gynaecologist strongly advised for doing the LEEP procedure. The patient does not have children yet, and she was scared of conization. She decided to come to me for homeopathic treatment.
Her childhood diseases:
- Bronchial asthma with the difficulty of breathing in a humid climate. She was on a nebulizer with salbutamol on and off
- Eczema on flexors of joints.
Repertorization of symptoms:
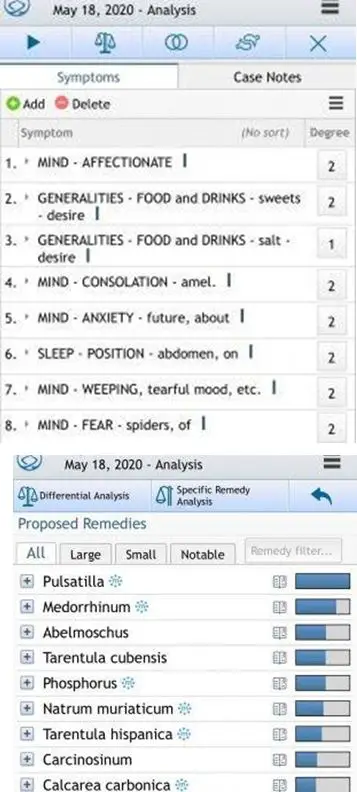
Pulsatilla 200 CH was prescribed in diluted form for 1 month.
Second consultation on 22/06/2020
The patient still has anxiety, sleep disturbance, palpitations, and internal trembling. She has a dry rash on her fingers, eczema (old symptom) and body rash. The acne has gotten worse, nodular. Patient asked if she is ok to seek laser removal for her acne. I advised against this, as this would be suppression of skin manifestation.
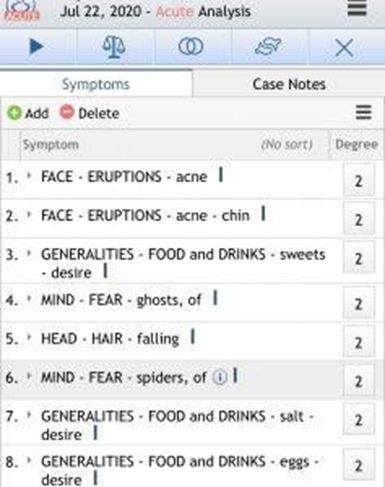
Repertorization of symptoms:
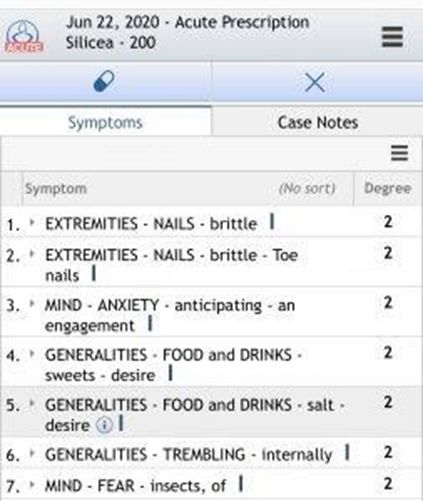
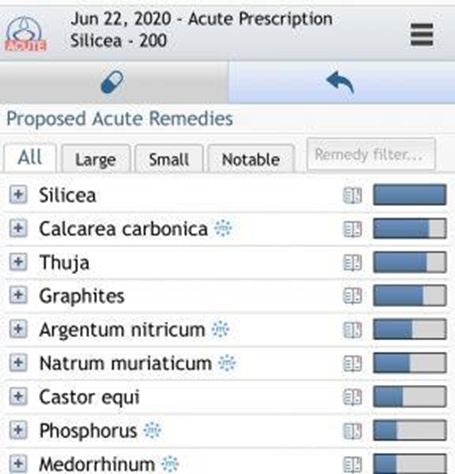
Silica 200 CH was given in diluted form with increased dynamization for 1 month.
Third consultation 22 July 2020
Patient got a skin rash-folliculitis on her abdomen. I advised against using any creams and the rash disappeared after 3 days on its own. Her acne got better as well, less nodular but pigmented. Nails better. Hair falls less. Body rash is gone. Her doctor also said her PCOD has gotten much better. She did a scan in her hospital and Dr said her PCOD was much better, especially on her right side.
Gynaecological examination revealed that her cervical erosion had become smaller.
Repertorization of her symptoms:
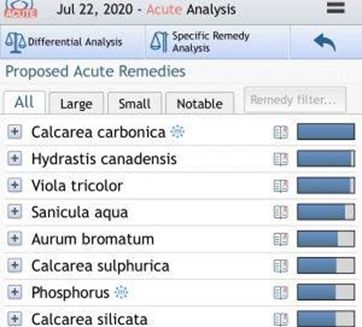
Calcarea Carb 200 CH was given in diluted form for 1 month.
Fourth consultation on 03/09/2020
Patient reported that her sleep, and mood has gotten better. She had boils on her back with pus coming out of them. Gynaecological examination revealed no cervical erosion anymore. Her Cervix looked healthy. She was no longer anxious about her health, her hair-fall stopped, acne got much better, and periods became more regular. She still had some eczema on her hands.
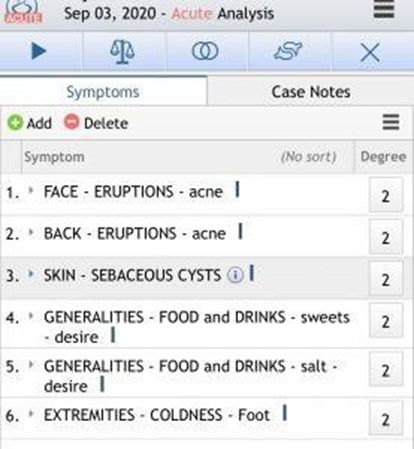

Calcarea Carbonica 200CH was given again in diluted form, but with stronger dynamization for 1 month.
In October 2020 she checked her PAP smear. It was normal. Eczema was gone. Acne is much better.
HPV was checked in November 2020, the result is negative. (See lab work below)
Conclusion
After 4 months of homeopathic treatment, her cervical erosion disappeared, the cervix is normal in appearance. Her LB PAP smear is normal. Her HPV test is negative. She doesn’t have any anxiety. Her self-confidence has improved. Her hair loss stopped. Her PCOD improved and periods are more regular now. Her acne improved a lot.
This case showed a very successful cure of deep precancerous cervical changes CIN1-CIN2 (LSIL-HSIL), associated with high oncological risk HPV 18, with the use of homeopathic treatment in 4 months.



A skillfully worked case with a very happy conclusion. It demonstrates the power of homeopathy in the hands of an experienced, knowledgeable practitioner.
Would the use of cryosurgery be considered “suppression”?