This is a case of chronic kidney disease in a female patient of 32 years living in New Delhi. I was first consulted for this case on 20th November 2020 when the patient was admitted in the ICU of a hospital because of development of septicemia post-surgical excision of an abdominal hematoma that developed after the patient underwent a bariatric surgery to lose weight in August 2020.
Some Case Background
This patient was on dialysis, and I was consulted when patient developed septicemia and was going into multi organ failure. After surgical excision of the hematoma, she had been on a ventilator for 48 hours as her oxygen level dropped drastically.
The blood pressure was 60/40 mmHg and the patient developed complete suppression of urination. The patient developed jaundice because of extensive RBC destruction. The doctors at the hospital had to perform open surgery instead of laparoscopic surgery because the hematoma was compressing the spleen and when they started laparoscopic surgery there was extensive bleeding.
The patient was off ventilator after 48 hours from the surgery, and post-surgery the kidney stopped functioning and urine output was zero with complete anuria. The patient was conscious and talking after ventilator was removed and had an angry expression on her face. She was undergoing dialysis every alternate day.
Just prior to the admission to the hospital this lady had separated from her husband and was living at her parents’ place. Her husband did not even come to meet her in the hospital. The patient was about to file a divorce case just when this happened.
Even the doctors at the hospital did not want the husband to meet her as it might worsen her situation. The patient was also not willing to meet him.
Within 24 hours of the removal of the ventilator, the patient’s creatinine levels started rising and the WBC count was also extremely high. There was a constant frown on her face and her eyes were wide open. The doctors at the hospital called it dialysis related dementia.
The patient became so violent that she started spitting all over the floor and her hands had to be tied as she was trying to pull out the Iv cannula. She was put on sedatives and the next morning she developed swelling all over her body and became completely dull like a statue and was not even answering any questions asked by the family members.
She was completely unaware of her surroundings and sat motionless on the hospital bed staring constantly towards the ceiling of the room. The patient’s TLC was 32000 with complete anuria and she also developed bed sores.
There was bleeding from the rectum mixed with stool and the blood was of a dark color. Her hemoglobin levels had dropped to 3mg/dl and she had to be given a blood transfusion after which the hemoglobin levels rose to 8mg/dl.
The doctors at the hospital could not locate the site of the bleeding even after CT scan of the abdomen. The dialysis was continued on every alternate day and within 2 days the patient became completely disoriented. She kept murmuring “it is a trap” and “everyone is trying to kill me” etc.
The patient’s parameters were improving after dialysis and blood transfusion, but the orientation deteriorated dramatically, signifying wrong direction of the case. Next morning the patient’s oxygen level started falling and went as low as 72%.
Her hemoglobin fell to 4mg/dl and she was again shifted to the ICU. The body was moving slowly towards overall destruction. The patient’s body was completely swollen and started turning black. The patient also developed a cough because of pulmonary congestion and her sputum became blood tinged and the doctors were afraid that they were about to lose her.
CASE ANALYSIS
This was the situation when the relatives of the patient called me. Based on the hematic jaundice, black discoloration of the skin, bleeding from the rectum & mouth and the low hemoglobin levels I asked the attendants to apply CROTALUS HORRIDUS 30 on the palms and soles of the patient.
Crotalus horridus is the angriest of the Ophidia group and it covered the acute changes in the disposition of the patient as well.
FOLLOW UP
- The patient passed 100 ml urine in 24 hours
- The bleeding from the mouth and the rectum stopped completely
- The hemoglobin increased with a consequent increase in the oxygen saturation as well
- The jaundice settled down and the bilirubin was normal in next 3 days
The patient was discharged from the hospital after 5 days. After a week, one night the patient suddenly developed persistent tremors of the head and neck and she became completely insensitive to all her surroundings. The only thing she said was that she was afraid of dying.
Her eyes were bloodshot and there was continuous involuntary movement of the head and neck without the patient being aware of it. These neurological changes may have been a result of dialysis, medication, or blood transfusion. The patient was keeping her eyes completely closed and refused any oral feed.
The doctors had done a percutaneous endoscopic gastrostomy (P.E.G.) for parenteral feeding. What is remarkably interesting to note is that in the initial stages in which the patient was prescribed Crotalus horridus there was no fear of death and on the contrary, the body was tending towards frank destruction with sudden decline of all the parameters essential for maintenance of life.
The development of a fear of death indicates a shift of the gear from syphilis towards sycosis and can be considered a welcome sign. The tremors that the patient was suffering from may be a result of physiological imbalance because of overmedication, dialysis, and blood transfusion. So, an acute state remedy for the physiological disturbance was to be hunted for.
CASE ANALYSIS
Based on the causation of loss of vital fluids (dialysis) and the dullness and indifference to the surroundings I prescribed, ACID PHOSPHORICUM 1M, unit dose.
The next day the patient passed 1300 ml urine and the tremors stopped within 12 hours. The eyes regained their normal color and were no longer bloodshot. The listlessness after loss of vital fluids along with the neurological symptoms post dialysis are covered by Acid Phos.
After Acid Phos, the patient had loose stools and gained some appetite. The patient started walking within the house in the next few days. Her creatinine level was still 4.3mg/dl (which was 5mg/dl initially). The patient also developed slight cough which was a result of the psychological fear of death (death fright conflict – Lungs; fluid accumulation – sycosis; fear of death – sycosis). The patient also had tremendous fear of dialysis.
After a few days when the patient was a little settled, she started developing symptoms like extreme irritation from the slightest noise, vomiting 2 to 3 times a day, loose stools, productive cough worse from lying down and increased irritability at trifles.
However, the patient felt much better than before as she was now able to walk and even resumed her office work from home. She was able to cook food as well and started oral feed. The single dose of Acid Phos 1M had given a remarkable result but the improvement had now come to a halt.
A month later, the patient’s condition again deteriorated. The blood pressure went as low as 70/50mmHg, there was severe chest pain, the urine output was as low as 100 ml per day and the TLC started rising again. Her cardiac enzymes were high, and the doctors advised ICU admission.
There was a suspected infection in the chest or the abdomen. The situation again started declining and homoeopathy was again put to the test in another life-threatening condition. All this while homoeopathy was being opted for when all doors had been closed and the patient landed in near a death situation.
The patient’s sister said that she had been having dreams of being deserted by her parents and of having fights with her husband, which she repeatedly complained of before being admitted to the hospital. The patient sat with open eyes and was completely motionless. She was staring at a fixed spot.
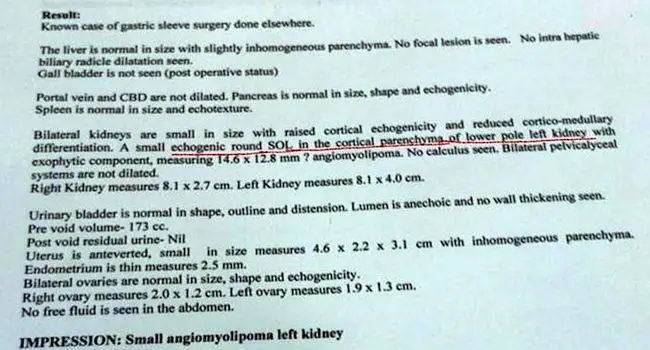
The doctors did an ultrasound of the abdomen in which a new growth was found in the left kidney and doctors diagnosed it as angiomyolipoma (a benign growth comprising of blood vessels, muscles, and fat tissue). The patient’s relatives became frantic when they were told that the patient had developed a tumour in the left kidney which required surgical excision as per the expertise of the treating physicians.
Now, these are the testing times for any homeopathic physician. As per our understanding of the doctrine of chronic miasms, the development of a benign tumour in the left kidney in a case of chronic renal disease is a good sign as this was nature’s way of increasing the renal parenchymal tissue to increase the GFR and promote better filtration of waste material like urea and creatinine.
Moreover, it confirmed our understanding of the shift of the miasmatic gear from syphilis to sycosis. Whenever, sycosis comes up in such cases, one thing that we can rest assured is that the threat to life has reduced as sycosis means lingering of disease and it will never go towards fast destruction which is characteristic of Psorosyphilis.
In the earlier scans, the kidney parenchymal only showed atrophic changes characteristic of syphilis and now we have a benign growth in the kidney parenchyma signifying the shift towards sycosis which is indicative of right direction of treatment.
Luckily, as the blood pressure of the patient was extremely low, the surgery was deferred by three days. The doctors were insisting on immediate surgery as they thought the tumour might be impinging somewhere and decreasing the urine output.
The patient looked as if she had become a statue. We had very little time with us and based on the current situation I considered the rubrics:
- MIND, STUPEFACTION, SITS MOTIONLESS LIKE A STATUE
- DREAMS, QUARRELS
- KIDNEYS, SUPPRESSION OF URINE
The patient was prescribed a unit dose of STRAMONIUM 200. Within three hours the blood pressure returned to normal, and the patient passed 1500 ml of urine in the next 24 hours. She was kept under observation for the next three days during which she passed 1800-2000 ml urine per day which meant that surgery could now be deferred, and the patient was eventually discharged from the hospital.
After Stramonium, the frequency of dialysis was reduced from once in two days to once a week. The nephrologist also acknowledged the fact that the kidneys responded well to whatever homoeopathic medicine was given to her.
What I understood was that she was improving and again relapsing into some emergency. As per aphorism 221 and 222 of The Organon of Medicine we were not prescribing the anti-psoric after treating the acute emergency state.
In a deep-seated sycosyphilitic pathology we were prescribing on the psorosyphilitic aspect of the case and hence the improvement was only short lasting. I realized what was lacking in the case and started looking for the anti-psoric (constitutional) remedy for the patient.
The patient had been a very obedient girl. She had been a very timid girl since her childhood and did not have many friends. She avoided public interactions as she was hesitant to speak up in front of many people. She was creative, and loved to bake cakes and make chocolates at home.
Her sister said that she was the most hardworking person in their family and had always been a very diligent person. The patient was forced to marry against her wishes by her parents. Her husband was not at all hard working and within a few months of marriage he left his job and the strain of bearing the expenses of the family came on to her shoulders.
Since childhood, she was like the man of the house. She did all the household jobs that her brother should have done and was always known as the most tomboyish girl of her class. As she had separated from her husband and was living at her parent’s place, she had a strong sense of guilt because she felt that she had become a burden on her father and brother as they had to bear the expenses of her as well as her daughter.
She resumed work immediately after she improved a little from her grave condition so that she could contribute financially to the family, and she used to attend the office despite having high fever and chest pain. She had a very tough time post-marriage and there were regular fights with her husband.
Things got out of hand when the husband did not return home on her birthday and instead went to a party with his friends. Since that day she decided to separate from him and moved to her parent’s house. There had been episodes when the husband returned home in a drunken state.
She had tried hard to adjust and save her marriage but all in vain. Her first liposuction surgery was also opted for because she wanted to look more attractive so that her husband would start taking care of her. The kidney function also started deteriorating during this period (ongoing existence conflict).
The patient’s biggest dilemma was that her daughter should not become like her husband and to avoid this she used to be overly harsh on her. Whenever her daughter refused to study or when she made some mistake in public, the patient used to say out loud that it is because her father was like this that the girl misbehaved.
There were instances where the patient also slapped her daughter publicly whenever she did some childish behavior. The extent of the patient’s hatred for her husband was palpable. I asked the patient about her thought process prior to the development of the disease to which she replied that she felt as if her family always preferred her two siblings over her.
This may have been the reason that they got her married to such a man without even checking whether that man was worthy enough to be married to their daughter. In order to be loved and appreciated the patient became very hardworking since her childhood.
She married that man to keep her parent’s word. Even after the marriage she felt that her husband never cared for her. He could neither provide her with love and support nor take care of her and her daughter financially. Her husband did not even give any expenses for the daughter’s education.
The patient had been having a persistent cough with chest pain for two months when she came to see me in the clinic. I enquired about any anxiety or fear that she had in her mind to which she remarked that after she was hospitalized the second time, she had developed a persistent fear of death and felt that she did not have many days left.
She was most troubled by the fact that when she would die, there would be nobody to look after her daughter. As she was already an added burden on her family, she wanted to invest money to secure her daughter’s future in case something untoward happened to her. She did not want her daughter to feel that her mother never cared for her. This was a ramification of her own feeling of being neglected by her parents and husband.
CASE ANALYSIS
Based on the mannish behaviour of the patient since childhood and the predominant animus in her, the first rubric considered was, MIND, DELUSION, IDENTITY, ERRORS OF PERSONAL IDENTITY.
The second rubric considered was based on her introverted and timid nature whenever she went to a public gathering (genetic traits) – MIND, TIMIDITY, PUBLIC, ABOUT APPEARING IN
The third rubric taken was the pathological process going on in the body – KIDNEYS, SUPPRESSION OF URINE
Remedies that covered the three rubrics were: –
- Plumbum – 6/3
- Lachesis – 5/3
- Phosphorus – 4/3
- Petroleum – 3/3
Looking at the repertorial analysis a very peculiar rubric came to my mind and that was MIND, DEATH, PRESENTIMENT OF, SETTLING HIS AFFAIRS, MUST BE in which the only medicine mentioned is Petroleum. I enquired about petroleum and got the confirmatory symptoms of headache and nausea from carriage riding.
On further interrogation it was found that the loose stools that the patient had also were always aggravated in the daytime. The patient was chilly, thirsty and introverted which fitted the description of Carbons. Petroleum is the only diligent carbon.
Also, Petroleum rafinatum is mentioned under Delusion, neglected, he or she is neglected, which was a constant perception of this patient since her childhood.
PRESCRIPTION
The patient was given a unit dose of PETROLEUM 200.
FOLLOW UP
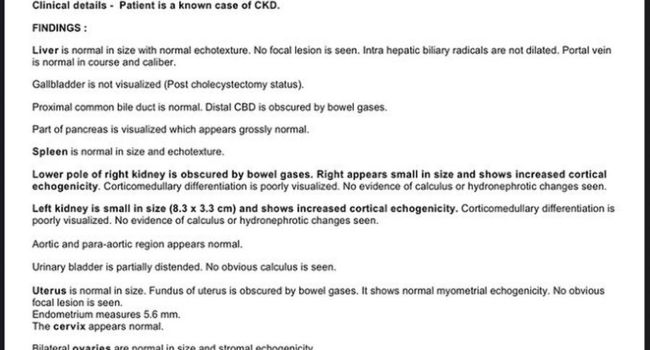
- The tumour in the renal parenchyma (angiomyolipoma) was not seen on latest scans
- The patient’s glomerular filtration rate has improved to 31% (which was 9.91% when we started treatment)
- The patient’s creatinine levels were 5mg/dl when we started her treatment and now, they have come to 2.1mg/dl
- Urine output is maintained at 1700-2000ml/day
- Patient has been going to her office daily for the last 8 months and can do her daily chores
This case shows how homoeopathy can restore organ failures as well as be effective in handling acute life-threatening medical conditions when practised on principles.




Very well presented case, thanks for sharing some insights in Emergency cases with Homoeopathic approach
Absolutely masterclass.
marvelous case & superb analasys. Hats up to you sir, we can learn much in this case based on principles of homeopathy but not just prescribing as per rubrics of case. you have analysed the journey of miasms very well and person in disease which is a very good lesson to all. Thank you for sharing. we are more convinced & confidence levels increased that homeopathy can bring back life from death bed.
This was such a difficult case and you put in lot of effort to understand and treat the case. A very good learning for us. Thanks!!!