Keywords: Community Acquired Pneumonia (CAP), case report, homeopathic therapy
BACKGROUND
Pneumonia is the most frequent acute lower respiratory tract infection, contributing to the highest mortality rate in infectious diseases,1 largely affecting males more than females.2 The most common causative agent of pneumonia is Streptococcus pneumoniae (pneumococcus), that affects 18% of the total pneumonia cases.2 Whereas, other agents (atypical pathogens) like Hemophilus influenzae and intracellular pathogens (Legionella pneumophila, Chlamydophila pneumoniae, Mycoplasma pneumoniae and others) contribute 2-20% of pneumonia cases and are generally less severe or even self-limiting.3 However, it is estimated that over 50% of the pneumonia cases go without a microbial diagnosis and the cause is considered to be unknown.2
In an attempt to classify the condition, the American Thoracic Society classifies PN based on their location of acquiring infection as – Community-Acquired pneumonia (CAP – acquired outside a hospital – focus of our study), Hospital-Acquired pneumonia and Ventilator Associated pneumonia.4 The gold standard tool for diagnosing CAP is Chest X-ray (CXR), which maps out any one of the 3 radiological signs viz. focal nonsegmental (lobar), multifocal bronchopneumonia (lobular), and focal or diffuse (interstitial).5 High-resolution computed tomography provides a better study of these patterns, but generally opted when the cause is undetermined. Routine serological tests and sputum culture are additionally advised to evaluate severity.6
The most accepted treatment guidelines for CAP is through administering antibiotics and respiratory fluoroquinolone in presence of other co-morbidities.7 Recommendation for an inpatient management is assessed by the CURB-65 (Confusion, Uremia, elevated Respiratory rate, low Blood pressure – 65 years of age and older) score, which estimates risk of mortality in CAP cases with a score greater than two.8
Likewise PSI (Pneumonia Severity Index) score is also used for evaluating patients aged above 50 claiming better indication.8 The clinical efficacy and safety of antibiotics for CAP is still under question; one due to its potential systemic adverse effects9–11 and the other due to antimicrobial resistance to various antibiotics processed so far, calling forth novel antibiotics which in turn requires clinical trials.12,13 The use of CURB-65 is still under debate due to its moderate accuracy.14
As mentioned previously, it is documented that the majority of the CAP cases have no pathogens detected, and yet the antibiotic regimen is recommended even in these cases as per the guidelines. Hence, we present a case report of a 30-year-old male diagnosed with CAP (of indeterminate etiology), treated with individualized classical homeopathic therapy. The patient never took antibiotics and had no known comorbidities. There have been studies formerly conducted under homeopathic therapy for respiratory infections, but failed to prove its effectiveness due to its generalised approach of the cases15 .
CASE REPORT
A 30-year-old male
Initial consultation: 29 October 2019
Chief complaints:
Patient was coughing for 1 week before the first consultation. Cough was dry, no expectoration and had to strain a lot but in vain. Constant coughing, more at early morning around 6 am. Cough in two bouts+2. Violent cough on attempting to speak+3 and immediately after lying down at night+2.
Cough followed by dryness of mouth and need to drink water very often in large quantities, but this does not quench the thirst. Cough accompanied with violent sneezing; nasal discharge flies off from nose especially in the morning+2.
Appetite diminished, likes spicy fried food; occasionally constipated. Cannot tolerate both extremes of temperature but cannot tolerate heat more and needs fanning.
As patient was in severe distress because of coughing, he was not willing to give any mental symptoms.
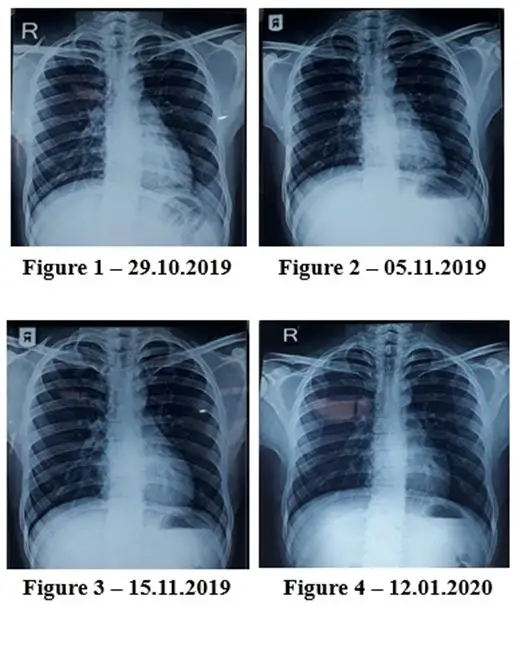
Investigations (CXR – PA view): Consolidation noted in left lower zone (See Figure 1.)
Repertorization 1: 31.10.2019
Prescription: LACHESIS MUTA 1M single dose
FOLLOW UPS:
| DATE | FOLLOW UP | INVESTIGATION (CXR-PA VIEW) | PRESCRIPTION |
| 31.10.2019 | Patient said he is slightly better. After 15 days of disturbed sleep, he slept peacefully.
Cough slightly persists. Sneezing stopped after the first dose, but it again increased in the morning. He said he used menthol-based ointment (antidotal substance). |
– |
Lachesis 1M single dose repeated once |
| 05.11.2019 | “Patient says it has been a miracle.” Coughing almost nil. Sneezing in the morning stopped.
He can sleep better. Expectoration has started now. Appetite improved. He can eat now though he does not feel hungry. |
Reduced extent and density of left lower zone opacity. Prominent broncho-vascular markings seen at both lungs. Improvement in consolidation of left lower zone with decreasing haziness (See Figure 2.) | Nil |
| 15.11.2019 | Cough is better, but eruption on axilla appeared for a month and resolved without medication. | No evidence of haziness or consolidation in the left lung.
(See Figure 3.) and (See Figure 4. – 12.01.2020) |
Nil |
DISCUSSION
The sequel of lower respiratory tract infections such as PN is determined by the vigour of the inflammation initiated. In recent studies, the concept of integrated pathogenesis in cases like PN are emerging with wide acceptance that pulmonary cells and extrapulmonary cells or tissues in unison drive out the infection and protect the lung tissues, while the same can turn counterproductive if the on-going inflammation is dysregulated, leading to chronic inflammatory states.1
Further, pulmonary dysbiosis through massive prescriptions of antibiotics can yield similar disaster.11 The homeopathic system of medicine, with its integrated perspective on pathology, preserves the immune system from degenerating, thereby providing a general state of well-being for the patient and the same is being demonstrated in the case report presented here.
The patient suffered from acute episodes of violent cough with no history of fever along with the infection and the CXR revealed consolidation prominently in the left lung. The prescription was based on acute pathological and general symptoms presented by the patient at that time and the choice of high potency was due to the clear acute picture.
The remedy not only brought about a considerable betterment of violent cough and sneezing, but also helped to improve his sleep and appetite. The lung resolved, evidenced by the normal CXR at the end of the treatment. During the first interview the patient expressed that, though he had such violent bouts of cough, he could not bring out expectoration.
After Lachesis he started to expectorate, which is a good sign in the right direction. The undeniable appearance of eruptions on the axilla as the patient was nearing cure signifies that the remedy not only achieved lung clearance but also elevated the immune system, in consonance with the theory of Levels of Health;17 which states that the defense mechanism in better health levels impels the pathology to a much lower order (here from lung organ to skin) and pushes the organism to higher health states. We can claim cure with not just the evidence of shift of pathology from lungs to skin, but also with the evidence that the skin eruptions on axilla completely cleared at the end of the treatment period.
CONCLUSION
This case report is an example of cure achieved in infectious conditions like CAP through individualized classical homeopathic therapy, without the aid of antibiotics or hospitalization. Additional case studies are required to strongly establish the efficacy of classical homeopathy in such instances.
REFERENCE
- Ferreira-Coimbra J, Sarda C, Rello J. Burden of Community-Acquired Pneumonia and Unmet Clinical Needs. Adv Ther. 2020;37(4):1302. doi:10.1007/S12325-020-01248-7
- C C, I M-L, C G-V, A SJ, A T. Microbial Etiology of Pneumonia: Epidemiology, Diagnosis and Resistance Patterns. Int J Mol Sci. 2016;17(12). doi:10.3390/IJMS17122120
- FW A, JT S, JA R. Role of Atypical Pathogens in the Etiology of Community-Acquired Pneumonia. Semin Respir Crit Care Med. 2016;37(6):819-828. doi:10.1055/S-0036-1592121
- G M. The definition and classification of pneumonia. Pneumonia (Nathan Qld). 2016;8(1). doi:10.1186/S41479-016-0012-Z
- Cilloniz C, Martin-Loeches I, Garcia-Vidal C, Jose AS, Torres A. Microbial Etiology of Pneumonia: Epidemiology, Diagnosis and Resistance Patterns. Int J Mol Sci. 2016;17(12). doi:10.3390/IJMS17122120
- Regunath H, Oba Y. Community-Acquired Pneumonia. StatPearls. Published online August 11, 2021. Accessed August 23, 2021. https://www.ncbi.nlm.nih.gov/books/NBK430749/
- RG W. Guidelines to Manage Community-Acquired Pneumonia. Clin Chest Med. 2018;39(4):723-731. doi:10.1016/J.CCM.2018.07.006
- AR M, CS K. Community-acquired pneumonia: Strategies for triage and treatment. Cleve Clin J Med. 2020;87(3):145-151. doi:10.3949/CCJM.87A.19067
- HJ T, JH W, CC L. Lefamulin vs moxifloxacin for community-acquired bacterial pneumonia. Medicine (Baltimore). 2020;99(29):e21223. doi:10.1097/MD.0000000000021223
- SM S, T F, J S, LA B. Antibiotics for acute bronchitis. Cochrane database Syst Rev. 2017;6(6). doi:10.1002/14651858.CD000245.PUB4
- D Y, Y X, X S, Y Q. The impact of lung microbiota dysbiosis on inflammation. Immunology. 2020;159(2):156-166. doi:10.1111/IMM.13139
- S S, PG C. Controversies in diagnosis and management of community-acquired pneumonia. Med J Aust. 2017;206(7):316-319. doi:10.5694/MJA16.01463
- K E, H W, A B, A A, HZ A. Clinical cure with ceftriaxone versus ceftaroline or ceftobiprole in the treatment of staphylococcal pneumonia: a systematic review and meta-analysis. Int J Antimicrob Agents. 2019;54(2):149-153. doi:10.1016/J.IJANTIMICAG.2019.05.023
- A I, A M, V K, et al. Performance of the CURB-65 Score in Predicting Critical Care Interventions in Patients Admitted With Community-Acquired Pneumonia. Ann Emerg Med. 2019;74(1):60-68. doi:10.1016/J.ANNEMERGMED.2018.06.017
- K H, ML van D, BJ B, TM M, D K. Homeopathic medicinal products for preventing and treating acute respiratory tract infections in children. Cochrane database Syst Rev. 2018;9(9). doi:10.1002/14651858.CD005974.PUB5
- Z W, Q P, C H, M W. Crosstalk Between Lung and Extrapulmonary Organs in Infection and Inflammation. Adv Exp Med Biol. 2021;1303:333-350. doi:10.1007/978-3-030-63046-1_18
- Vithoulkas G. Levels of Health.; 2017.


Outstanding. Thanks for sharing.
Amazing 👍👏
Nice presentation of case.