
Chief Complaint:
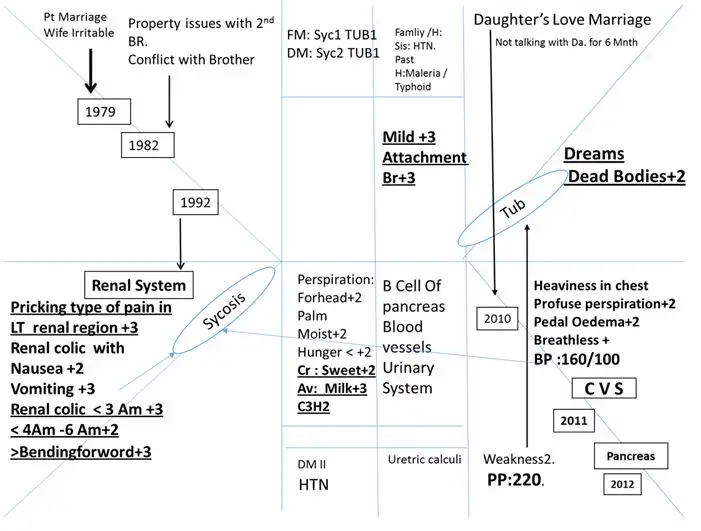
A 61-year old retired forest officer, a known case of diabetes mellitus II and hypertension presented with heaviness in chest, profuse perspiration with pedal oedema and generalised weakness since 2012. He is on T. Glibenclamide ½ OD T. Ecosprine Av 75 1 OD and T. Amlodep AT 1 OD since 2012.
Last FBS: 134 and PLBS: 220 with anti-diabetic. He is also suffering from renal calculi since 1992. He has pricking type of renal colic episodes < 3 am3, < 4am – 6am2 and pain > bending forward3. Nausea and vomiting 2 with mild urethral pain before micturition. He has experienced 11 episodes of renal colic till now.
Patient as a person:
Appearance: Moderately obese, wheatish complexion, baldness.
Skin: Cracks on soles 1-2 yrs. < winter+ HAIR: Loss since 1990
Hunger < can’t tolerate +2 CRAVING: Sweets+2 AVERSION: Milk+2
Thermally: C3H2
Past History: Malaria/ Typhoid in 1992.
Family History: Sis: HTN. Fa: Some psychiatric illness.
Addiction: Social drinker beer, tadi etc.
Physical Examination:
PR: 80 BP : 140/80 with Anti-Hypertensive Weight: 85
R/S : AEBE /Clear CVS: S1S2 N P/A : Soft
MSS: B/L Foot Pedal Oedema +2
Investigations with OHA:
FBS : 134 PLBS :220
- Creat:1
Urine R: Albumin: Absent
USG –KUB: Lt sided mild hydro-nephrosis, LT lower uretic calculi.
Other investigation not available with patient
Life Space:
61 yrs. male, wheatish complexion, obese, appeared very calm. He had no eye contact during interview (shyness while talking). He stated that his childhood was uneventful. His father was a farmer who expired when patient was 7 years old.
At that time his brothers and mother took responsibility for the family. He has two elder brothers and two sisters. All were living in joint family in one house. He married in 1979.
His wife is irritable by nature. In 1982 during property distribution his elder brother demanded complete share of agriculture property. To avoid conflict the patient accepted his demand but still his brother was not happy
His brother reasons that the patient had government service so he should not get ancestor’s properties. Since 15-20 yrs. his elder brother is not talking with him. Many times, patient tried to resolve this issue, but his brother is not ready to keep relations with him.
Once patient’s son entered the compound of his brother’s house where the son was beaten by his brother. That time also patient didn’t react and the issue was solved calmly. In 2010 his daughter got married without his consent, He did not talk with her for 6 months.
He described himself as very calm since childhood and a little anxious about health. In school he was an average student. He never took part in quarrels and always avoided them.
CASE PROCESSING:
Classification and Evaluation for Approach Selection
| Heading | Symptoms |
| A. Physical General Modality : | <Hunger<+2
<Winter+ |
| B. Particular Modalities : | < 3 Am +3
< Night + > bending forwarded +3 |
| C. Physical generals | Cr : Sweet+2 Av: Milk+3
C3H2 |
| D. Characteristic Sensation | Pricking pain +3 |
| E. Characteristic Location | LT renal region +3 |
| F. Mental emotional Attribute Type | Mild 3
Attachment 3 |
| G. Subconscious | Dreams Dead People 2 |
Boenninghausen Approach: Totality
- < 3 Am +3
- Hunger < can’t tolerate +2
- > bending forwarded +3
- Pricking pain +3
- Cr : Sweet+2 Av: Milk+3
- Mild+3
- Attachment +3
- Dreams Dead bodies+2
- Chilly +2
Reason for Boenninghausen approach:
- Complete symptom available
- Characteristic modalities available
- Characteristic sensation available.
- No qualified mental expression.
Essential Evolutionary Totality:
Repertorization
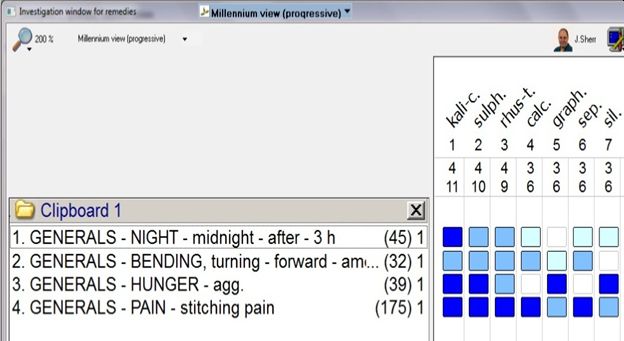
Potential Differential Field:
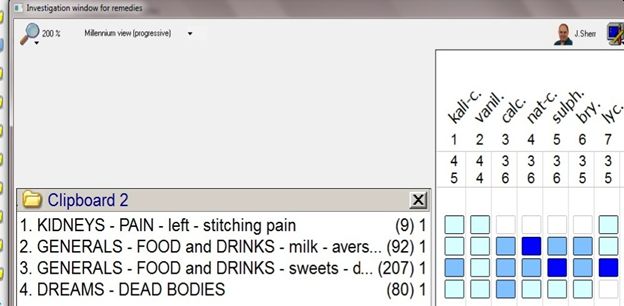
Final impression: Kali carb
The core of this individual is understood in terms of the attachment to his brother and timidity. Physical data is more essential to differentiate the remedy in this case. Calcarea Carb and Silica come very close in terms of core and physical expression of this case which is reflected in above repertorization. There is very peculiar location and sensation that is: stitching in Lt Kidney and specific time modality of 3 AM aggravation with chilly patient. This indicates kali carb will be more suitable for this case.
Follow up Criteria:
- Dreams
- Anxiety Health
- Weakness
- Chest heaviness
- Breathlessness
- Renal colic episode
- Urethra pain B Maturation
- Pedal oedema
- BP
- FBS /PLBS / WT
Follow ups
| Date | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | New S/S | Prescription |
| 29/1/13 | S | S | > | 0 | 0 | 0 | S | S | 120/86 | WT: 85KG | Kali Carb 200 1P | |
| 12/2/13 | S | S | S | 0 | 0 | 0 | S | S | 100/70 | Kali Carb 200 1P | ||
| 19/2/13 | S | S | S | 0 | 0 | 0 | > | S | 110/70 | Kali Carb 200 1P | ||
| 26/2/13 | S | S | >++ | 0 | 0 | 0 | > | >+ | 100/70 | F : 83
PP :78 |
Kali Carb 200 1P | |
| 5/3/13 | 0 | > | >++ | 0 | 0 | 0 | > | ++ | 120/90 | Kali Carb 200 1P | ||
| 19/3/13 | 0 | > | >++ | 0 | 0 | 0 | > | ++ | 110/70 | WT:84.5Kg | Kali Carb 200 3P | |
| 2/4/13 | 0 | > | >++ | 0 | 0 | 0 | >++ | >++ | 130/80 | 26/3/13
F:105 PP:136 |
Stopped T.Glibenclamide T. Amlodep AT
By allopathic Physician on 6/3/13. |
Kali Carb 200 3P |
| 16/4/13 | 0 | > | >++ | 0 | 0 | 0 | 0 | >++ | 110/90 | WT: 84.5Kg | Kali Carb 200 3P | |
| 30/4/13 | 0 | 0 | >++ | 0 | 0 | 0 | 0 | 0 | 100/80 | Kali Carb 200 3P | ||
| 6/1/14 | Occ | 0 | >+ | 0 | 0 | 0 | 0 | > | 130/70 | F :98
PP:114 WT: 82 |
Kali Carb 200 3P | |
| 9/4/14 | occ | 0 | >+ | 0 | 0 | 0 | Occ | + | 110/70 | F:91
PP: 165 WT: 82Kg |
BP range 150-140/100-90
Started Amlodep ½ OD |
Thuja 200 1p +
Kali Carb 200 3P |
| 10/9/14 | occ | 0 | >+ | 0 | 0 | 0 | 0 | 0 | 110/70 | WT: 82Kg | BP range
110-130/80-90 |
Thuja 200 1p +
Kali Carb 200 3P |
| 20/1/15 | ++ | 0 | >+ | 0 | 0 | 0 | 0 | 0 | 110/70 | HGT: 145
@ Breakfast WT: 82Kg |
Antihypertensive
Stopped by self |
Thuja 200 1p +
Kali Carb 200 3P |
| 17/4/15 | ++ | 0 | >++ | 0 | 0 | 0 | 0 | 0 | 110/70 | Alcohol drinking started 2 | Kali Carb 200 3P | |
| 6/5/15 | > | 0 | >++ | 0 | 0 | 0 | 0 | 0 | 110/70 | F: 87
PP: 175 |
Episodes of vertigo on bending neck
Motion <2 No exercise. |
Conium 200
+ Kali Carb 200 3P |
Discussion:
From the above follow up record we can understand the qualitative improvement in subjective as well objective symptoms after Kali Carb 200 single dose. There is a significant improvement in generalised weakness followed by reduced subjective distress like chest heaviness, renal colic episodes and improvement in the blood sugar levels as well.
Gradually, as per the demand of susceptibility, the dose of Kali carb 200 has been shifted from one dose to three doses every week. By witnessing the above response to homoeopathic medicine, the allopathic physician stopped his anti-diabetic and anti-hypertensive medicines on 2/4/2013.
After the one year period of homoeopathic treatment the patient was feeling better with no episode of renal colic and no subjective distress. Due to some exciting cause like consuming alcohol and missing some homoeopathic doses, his range of blood pressure started fluctuating on the higher side, so the allopathic physician again started him on Tab Amlodep OD. When those symptoms stopped the patient discontinued the Amlodep and followed homoeopathic treatment.
Summary: The above case is an attempt to demonstrate the concept and technique of the Boenninghusen approach from symptomatology study. Availability of data in the case in terms of complete symptoms, general modalities, peculiar sensation and peculiar location with inadequate qualified mental symptoms demands the Boenninghusen approach in the case.
We know that, Boenninghauaen was a close follower of Hahnemann and he focused on essence of a problem in terms of image of the patient with drug picture. Hahnemann expected the homoeopathy physician to establish similarity, not at the level of sign and symptoms but at the level of Portrait of Disease which is elaborated in aphorism 5 and 6 of organon of medicine. Hence repertorization is an indispensable tool to understand the evolution of Hahnemann’s totality of the natural and drug disease as well as establishing the similarity between the two.


A few comments –
1. Hahnemann didn’t advise on disease portrait. It is always on symptom similarity especially the peculiar ones. We can see mathematical accuracy in applying this. Of all master’s disciples, Boenninghauaen applied this religiously in his practice.
2. It is surprising to see the repetition of a drug like Kali Carb every 15 days and later 3 times a week. Neither Hahnemann nor Boenninghausen gave medicines like that. At least, the master’s new mode of preparation (millesimal) could have been used which will allow such repetition.
3. Understanding the disease is advised to be gathered through the symptoms – not through the pathological terms (like pedal oedema) in order to capture the peculiarity.
4. When there is no improvement after a year, the second best remedy could have been used (using concordances).
5. In stead of publishing the results of repertorisation, the relevant symptoms of Kali could have been published (as Boenninghauaen used to do in his lesser writings).
In chronic diseases I have found it best to give a dose (e. g., a spoonful) of a solution medicine a least every two days, more usually every day.
Chronic Diseases – Samuel Hahnemann.
All perceptible signs represent the disease in its whole extent, that is, together they form the true and only conceivable portrait of the disease. These matters the true physician regards as actual symptoms of the disease, and they aid him to discover the nature of the disease, and to form an accurate portrait of it, so as to enable him to cure it with a similar medicinal morbific agent. Organon of Medicine – Samuel Hahnemann 6th edition.
Great reasult