Abstract: A patient who developed Takotsubo cardiomyopathy was treated successfully with Aconitum napellus and conventional treatment. She later developed autoimmune hepatitis which resolved with Lycopodium clavatum and a one week water fast. The possible connection between these conditions and chronic mercury poisoning from her amalgam fillings is discussed.
Keywords: Takotsubo Cardiomyopathy, Autotimmune Hepatitis, Homeopathy, Aconitum napellus, Lycopodium clavatum, case report
The following case report is formatted according to CARE guidelines. 1
Introduction
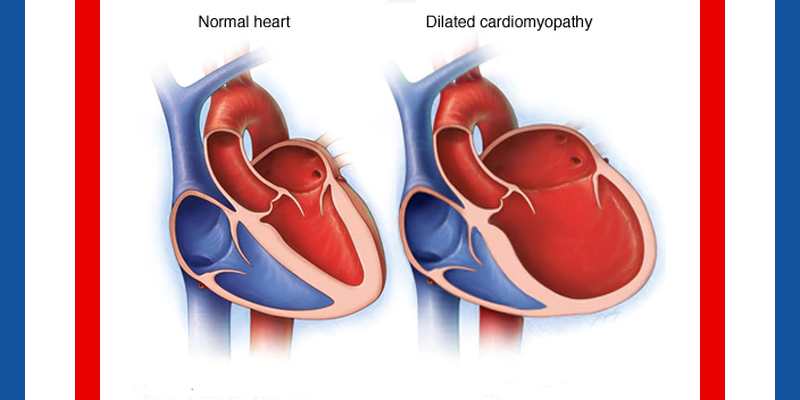
Takotsubo cardiomyopathy, also known as broken heart syndrome, is an acute syndrome first described in Japan in 1990 which occurs mainly in women and can mimic a heart attack. 2 Most people rapidly recover with no long term heart damage, but it rarely can result in death. Symptoms include chest pain and shortness of breath after a severe physical or emotional stress (Homeopathy for Stress). EKG changes and cardiac enzyme elevations can mimic a heart attack. However, cardiac catheterization reveals no evidence of coronary artery obstruction. Instead a ventriculogram reveals a characteristic ballooning of the left ventricle so that it looks like an octopus pot, which is the literal translation of tako tsubo. The cause is unknown, but it is suspected that surges of stress hormones (e.g. adrenaline) “stun” the heart, and prevent the left ventricle from contracting effectively. It is usually treated with standard heart failure medicines such as beta blockers and ACE inhibitors.2 It is suspected that older women are more susceptible due to reduced levels of estrogen after menopause. After performing a cursory Google search, no published cases of Takotsubo cardiomyopathy treated with homeopathy were found. So this would be the first such case. Additionally, this patient developed autoimmune hepatitis (AIH), which is an autoimmune disease of the liver which is diagnosed by the presence of elevated liver enzymes and various autoimmune markers. This condition is usually treated with corticosteroids and/or immunosuppressants. 3
| Timeline | |
| Dates | Medical history, Diagnoses and Treatment |
| 6/25/01 | First appointment for Psoriasis-treated with Causticum |
| Feb. 2003 | Psoriasis mostly healed |
| 5/16/08 | SOB and chest pain, Takotsubo diagnosed, Aconitum started |
| 8/14/08 | Normal Echocardiogram, Takotsubo symptoms resolved |
| 3/27/09 | Normal Echocardiogram |
| March 2009 | Symptoms of AIH develop |
| 4/13/09 | Lycopodium 10M started |
| Jan. 2010 | 7 day water fast |
| 11/23/10 | Liver enzymes normal from this point on |
| 2012 | Amalgam removal and 6 wks later kidney stone attack |
| 5/16/13 | Last amalgam was removed |
Patient Information-Past History
M.M. is a 76 year old female social worker born in 1940 who was first seen by me at the age of 60 on 6/25/01 for palmoplantar psoriasis and onycholysis. She did well over the next 3 years on Causticum beginning with the 200 D (Dunham) potency and gradually increasing to the 10M, 50M, CM, DM and MM potencies. The psoriasis initially aggravated, and then quickly resolved over a few months. It healed first on the upper part of her body and trunk and lastly on the lower body and ankles. The onycholysis also gradually resolved. Her sensitivity to injustice and her general mood and energy improved with the remedy. From 2004-2008 she received other remedies for various issues, including Staphysagria up to CM, Lycopodium up to 10M and Ignatia up to 1M.
Chief Complaint: Chest Pain and SOB
On 5/16/08 she calls to say that she’s had her wallet stolen out of her office. She feels shock (2), upset (2) and fear (2). When she called the credit card company, someone had already tried to use her credit card. Since this event, she is feeling a constant, dull ache/pressure substernally in the upper chest which does not radiate and is a 7 out of 10. It feels tight around her neck. To a lesser degree she has dyspnea and can’t take a deep breath. She has a small headache on the forehead and top of the head which feels like a tight hat is on. Although she teaches meditation, her meditation practice is not calming her down and her blood pressure feels high.
Homeopathic Assessment
A repertorization was not done at the time due to the acuteness of the problem and the clarity of the picture. However, in retrospect, a repertorization would look like the following figure.

(From MacRepertory4)
The acute onset, and the etiology which combines shock, fright and anger as well as the chest pain and dyspnea and headache clearly point to Aconitum napellus.
Homeopathic Intervention
The patient was told to take the Aconitum 200C 2 pellets by mouth as needed. Because the symptoms could be consistent with an acute myocardial infarction, we urged her to proceed immediately to the emergency room. She initially refused to go to the ER even though she worked there on a regular basis as a social worker. However, on urging she agreed to go to the ER for a blood pressure check. After taking the Aconitum 200C she immediately felt very hungry.
Testing, Follow-up and Outcomes
In the ER the chest pain increased to an 8 out of 10 but there was no nausea or sweating. After 2 doses of Aconitum 200C and 325 mg of aspirin, 5 mg of IV metoprolol and an IV drip and 0.4 mg sublingually of nitroglycerin her chest pain decreased to a 0 out of 10. Her blood pressure was up to 180/101. An EKG revealed sinus tachycardia up to 135, non-specific ST-T changes and a positive troponin-I at 0.689 and 13 hours later increased to 3.524 (normal is 0.010-0.039 and rising numbers indicate myocardial injury). She has a family history of coronary artery disease in her mom in her 40s. Physical exam was unremarkable except for a positive S4 on cardiac auscultation. CBC and BUN and creatinine were normal as was the CPK. With metoprolol, nitrates and aspirin her blood pressure and pulse and pain were controlled. The assessment in the ER was probable unstable angina and she was taken for cardiac catheterization. Surprisingly, the cardiac cath showed clear coronary arteries except for a mild, non-obstructive 20% left main ostial lesion. The ventriculogram showed a left ventricular ejection fraction of 25%, global hypokinesis with anterior, anterior apical and inferior apical akinesis. Also, it showed the pattern of apical ballooning seen in Takotsubo cardiomyopathy.
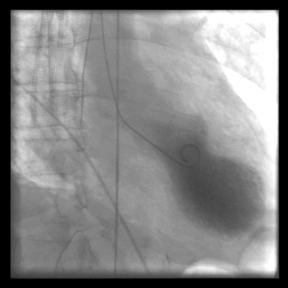
Ventriculogram with apical ballooning characteristic of Takotsubo cardiomyopathy. (By Tara C Gangadhar, Elisabeth Von
der Lohe, Stephen G Sawada and Paul R Helft
[CC BY 2.0 (http://creativecommons.org/
licenses/by/2.0)], via Wikimedia Commons)

Octopus pots on the beach. (By Nicholas.gosse (Own work) [CC BY-SA 4.0 , via Wikimedia Commons)
She was placed on enalapril 5 mg BID and carvedilol 3.125 mg BID. She took Arnica 10M after the catheterization and it helped stop the groin oozing of blood. She continued the Aconitum and took Ignatia once, the night after the catheterization and cried after taking it.
She was discharged from the hospital on 5/18/08. She was only able to take the carvidelol twice as it made her dizzy and short of breath. She started with Arnica 10M and then decreased it to 200C which she took once on 5/19 for soreness of the groin at the cath site, which was healing well. When she exerted she became short of breath, then anxious (2), then she took the Aconitum 200C in water and felt better with it (2). She was in an expansive mood, and was talking a lot and feared something would happen again. She was weeping (2) alternating with euphoria. She was having trouble wearing bras, and could only tolerate baggy clothes. She was feeling warmer and felt worse on getting up in the am on 5/19. She had just retired from her Zen group leadership role.
Rx: Lachesis 200C in water and repeat as needed for dyspnea and mood fluctuations. Arnica 200C can be repeated prn for groin soreness and Aconitum 200C prn for anxiety. She has just started the enalapril at half the recommended dose, i.e. 2.5 mg BID because she is sensitive to medication.
6/4/08
She still has episodes of anxiety when talking of her illness or retelling the story of her illness, and is worse with anticipation. She had two stronger episodes of anxiety after a call from her bank, and the Aconitum helped right away with the anxiety and the shortness of breath. Now she is only short of breath after 2 flights of stairs. When she got out of the hospital, half a flight of stairs caused dyspnea. At first she needed to sleep on 2-3 pillows but now is down to only one. She realized that she had had an episode like this 3 weeks before her ER visit with another stressful situation. With these episodes, she was paralyzed with fear. The Lachesis has helped with the loquacity, but has had no effect on the sensitivity to clothing around the chest (i.e. it is still difficult to wear a bra).
She continued to do better with the cardiomyopathy and the anxiety. She had a repeat echocardiogram on 8/14/08 and 3/27/09 which both revealed normal left ventricular systolic function and size and a normal ejection fraction of 60%. She weaned off the ACE inhibitor in August of 2008. Since that time she has continued to do well with her heart symptoms and anxiety, but if stressed and anxious with chest tightness and dyspnea she immediately takes the Aconitum and these symptoms resolve without further problems.
Development of AIH
In March 2009 she developed a pinkish color in her urine and a general feeling of malaise and depression. A urinalysis was positive for 4.0 mg/dl of urobilinogen (normal is 0.2-1.9) and so a CBC, CMP and Lipid panel were done. This revealed elevated liver enzymes with an AST of 313 IU/l (normal 10-40) and an ALT of 337 (normal 10-60). She was referred to a gastroenterologist for further testing and became quite anxious again, but the anxiety responded quickly to the Aconitum 200C. At the GI specialist, hepatitis A, B, and C testing were all negative, but her ANA was positive with a titer of 1:160 with a diffuse pattern, a smooth muscle (Actin) antibody was positive at 86 Units (normal 0-19), and a double-stranded DNA antibody was positive at 42 IU/ml was a borderline high result. On 3/19/09 the AST was slightly better at 250 and the ALT was 289. On 3/31/09 with these tests in hand, the GI specialist diagnosed autoimmune hepatitis (AIH) and recommended a liver biopsy and 5mg of prednisone daily. The patient refused both treatments.
Homeopathic Treatment of AIH
We placed her first on Natrum sulphuricum 200C 1-2 times daily in water with occasional doses by mouth and she felt slightly better. She was placed on a strict Vegan diet, which was not difficult for her as she had already been mostly vegetarian. On 4/13/09, we took a more detailed history and her symptoms repertorized as follows:
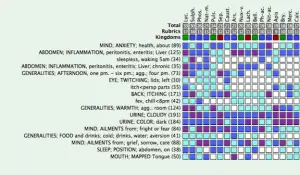
(From MacRepertory4)
Because of the hepatitis, her chilliness (which at times alternated with heat) and desire to be warm in bed but to have the room cold, her aversion to cold drinks, worse at 4pm, and fever or chills at 8pm, twitching of the left lids, mapped tongue and worse in a warm room the choice of Lycopodium was clear. She was started on Lycopodium 10 M 2 pellets by mouth prn for energy, soreness of the liver or mood.
Follow-up for AIH and Subsequent issues
Despite lots of stressors in her life, the Lycopodium 10M helped her sleep and immediately helped her irritability. She had to take it about once a week. After 1 month her symptoms plateaued with her liver being more sore and she had headaches with less effect from the 10M so she increased to Lycopodium 50M prn on 5/16/09. She had a terrible aggravation with the 50M: she felt the worst left TMJ attack in 5-7 years (the dentist found no problems with her bite). She had a massage and then was better and she then felt a tremendous sense of well being (2) and mental clarity. This lasted until 5/24/09 when her son came down with appendicitis in the midst of a bad divorce. She repeated the Lycopodium 50M on 5/26 and had less aggravation and then felt pretty good. Her labs on 5/29/09 were much improved with and AST of 46 (normal 10-40) and a normal ALT of 40 (normal 10-60)! The GI specialist thought the decreased AST and ALT were good, but felt that since AIH can have an up and down course, that a liver biopsy was still indicated. We sent her to a hepatologist at the University of Chicago Hospital for a second opinion. He found normal AST 31, ALT of 29 and GGTP of 13 U/L (normal 11-63) and a Fibrospect score of .25 (normal < .21). Because of these results, he felt it was a transient AIH due to the medications she had previously been on, and felt a liver biopsy was not indicated. On 1/9/2010 her AST was again up to 189 and her ALT was 235 and she was not feeling well. After this she went on a 7 day water fast and her liver enzymes gradually came back to normal by 11/23/10 and have remained there ever since. She continues to take the Lyc 10M or 1M as needed. She had another normal echocardiogram in June of 2010. On 10/25/12 her Fibrospect score was down to 0.17 which indicated no fibrosis.
She still had 3 large amalgam fillings which could have been contributing to her health issues, so she gradually had these removed by her dentist. Two of these amalgams were removed in 2012 and within 6 weeks she had a kidney stone attack. The last amalgam was removed on 5/16/13. She was continuing to take the Aconitum 200C up to two times a week for anxiety and the Lycopodium 50M for liver ache or full body itching. Her anxiety has gotten less over time, despite an increase in her stress. She was able to move into a more secure housing situation on 9/6/13. She has occasionally needed other remedies for problems like a meniscal tear in her knee due to a fall, vertigo and epistaxis. Overall her health continues to be good.
Patient’s report
On 6/23/15 the patient wrote:
I was reflecting on the fact that my health has been pretty stable recently. I didn’t have a cold all winter. All of my various systems appear to be functioning as they should. I’ve been taking Lycopodium CM since April about twice a week because of liver ache, sleeplessness or an upset stomach. I think that removing the amalgam was a really good thing and I believe that the floor of my health is better.
I’ve also taken Aconitum 10M quite a lot. Mostly when I get anxious and overwhelmed at the hospital (she works in the psychiatric unit as a social worker). I’ve increased my schedule there and can get sort of stressed out at times at the end of my shift. I still have a lot of stress in my family and will take it then as well.
I think a combination of therapy and the arrival of the baby (her son adopted a baby) have lowered my overall anxiety and raised my general cheerfulness.
At this point we are continuing to treat her with homeopathy and see her on an as needed basis. Since her amalgam removal her overall physical and mental/emotional health have continued to be more stable.
Discussion
This patient developed two relatively rare, potentially life threatening conditions which were clearly helped by homeopathic remedies. Takotsubo cardiomyopathy if not initially fatal usually resolves completely in 1-2 months. This patient showed this pattern of quick recovery and in fact her echocardiogram was normal 3 months after onset of the illness. She could only take the prescribed beta blocker twice due to side effects, but stayed on the ACE inhibitor for 3 months until the echocardiogram was normal. Aconitum napellus helped her with many bouts of feeling anxious and frightened which would lead to chest pain and shortness of breath if not quickly controlled. Thus the Aconitum helped her to get through this acute episode while receiving only a minimal amount of allopathic medicine. This was definitely a good thing, as 10 months later she developed autoimmune hepatitis, possibly as a side effect from the allopathic medicines she had received. By keeping the number and doses of allopathic medicines minimal, hopefully this helped to influence the eventual positive outcome with the autoimmune hepatitis. With the AIH, the patient refused prednisone and chose only to monitor the condition with labs. The Lycopodium clearly helped with the liver pain, headaches and energy. However, it was only after she went on a 7 day water fast and then maintained a vegan diet that her liver enzymes continued to improve and then finally normalized after 20 months.
For both of these conditions, even after the echocardiogram and liver enzymes had returned to normal, she continued to have the precursor symptoms of anxiety, chest pain and liver aches which continued to respond to Aconitum and Lycopodium respectively. In paragraph 3 of the Organon, Hahnemann after discussing how to match the medicine to the disease and select the proper posology states, “lastly, if in each case he knows the obstacles to cure and how to remove them, so that recovery is permanent, then he knows how to treat thoroughly and efficaciously, and is a true physician.” 5 My clue to what her obstacle to cure could be came while researching another paper for this journal. 6 While reading the background book Diagnosis: Mercury, I came across a passage where Dr. Hightower stated that she found cases of autoimmune hepatitis were strongly associated with chronic mercury poisoning in her experience. In the initial history and physical on my patient, I had noted that she had several large mercury amalgam fillings in her teeth which could be a source of such chronic mercury poisoning. A toxic and essential element hair test done on 12/25/12 confirmed this. Although the test showed only small amounts of mercury, the essential elements showed a pattern indicative of deranged mineral transport which confirmed chronic mercury poisoning. My experience treating many other patients with chronic mercury poisoning from mercury amalgams has shown that a pattern of deranged mineral transport in the essential elements and low levels of mercury is actually the norm in these patients as they are not able to excrete the mercury in their hair. In this patient, after having the last of her amalgams removed, she had a crisis of passing kidney stones, but then enjoyed a period of more stability with her health which continues until today.
I have been treating this patient for 15 years, and over that time have used many different remedies on this patient in many different potencies. The interesting history given here is only a small slice of a much larger history as the patient’s paper chart is currently 4.5 inches thick (I measured it.). Some might object to this saying that less remedies should be used. In fact, that has been my experience with some patients that only one or a few remedies are needed over a course of many years. However, it is also my experience that in patients with the barrier to cure of chronic mercury poisoning that such a complicated course using many different remedies in different potencies is in fact not unusual but rather the norm. Hahnemann recognized this as well, as in paragraph 171 he states, “In nonvenereal chronic diseases . . . one often needs to use several antipsoric remedies in succession to bring about a cure.” In these cases of chronic mercury poisoning, it is as if the underlying psora keeps pushing out these various acute conditions each requiring different remedies (i.e. they are dissimilar diseases) until the underlying mercury poisoning is dealt with. As it is said, we learn the most from those cases we struggle with the most. This most gracious patient with her various serious acutes and underlying chronic mercury intoxication has truly been an amazing teacher for me!
Informed Consent
The patient provided consent to publish this case report via email.
- Gagnier J. The CARE guidelines: consensus based clinical case reporting guideline development. BMJ Case Reports 2013.
- Takotsubo cardiomyopathy (broken-heart syndrome). (Accessed 9/3/16, 2016, at http://www.health.harvard.edu/heart-health/takotsubo-cardiomyopathy-broken-heart-syndrome.)
- Autoimmune Hepatitis. National Institute of Diabetes and Digestive and Kidney Diseases, 2014. (Accessed 9/3/16, 2016, at https://www.niddk.nih.gov/health-information/health-topics/liver-disease/autoimmune-hepatitis/Pages/facts.aspx.)
- MacRepertory. 8.5.2.9 ed: Synergy:MMPP version of Complete 4.5 Repertory.
- Hahnemann S. Organon of Medicine. First ed. Los Angeles: J. P. Tarcher; 1982.
- Fior T, Dunn D. A Modern Day Mad Hatter. AJHM 2014.



very interesting case.
I agree , many of my chronic cases have required a variety of deepacting remedies along with a few acutes.
ultimately …the fact that the patient is in a much better state of health at the other end of chronic treatment suggests that one remedy for life cannot be a norm.
given the fact the a majority are also on other allopathic chronic medication.. contributes to.this scenario.
Why did you tell us the remedy you prescribed at the beginning? For me this completely spoiled it as I like to try and work out the remedy myself!
topmost international level advice.myself non professional but one dr sp mondal of ishapore west bengal india used causticum 200 frequently after acute over.i saw his prescription for a executive sulphur 10m for very very severe constipation ,this person told me has much relief.books stress more on morning diarrhea for sulphur,homeopathy is typical science.
Pls read my recently published book “Homeopathy In practice”, subtitle “Clinical Insight into Homeopathy and Remedies” by Iqbal Husain. So far 3 Volumes have been published. Currently, I m reviewing the manuscripts of Volumes 5 & 6.
Professional Homeopaths will find these Volumes very helpful in quickly finding the needed remedies for variety of disease conditions. Will save lot of time and minimize the need for repertorization.
These volumes can be ordered from Amazon, Barn & Novels and other outlets.
I would highly appreciate your comments after you have read them.
Thnx.
Iqbal Husain
(630-899-9103)
Please send a specimen copy