I was informed about her condition on 10th September 2015. Mrs J.V.N. 82 years old, had been reported to have suddenly collapsed on 21st August 2015 morning minutes after she had waved goodbye to her grandchildren who were leaving for school. Immediately she was rushed to the nearest hospital, Campal Clinic, a reputed hospital with good emergency facilities, located at Panaji, Goa.
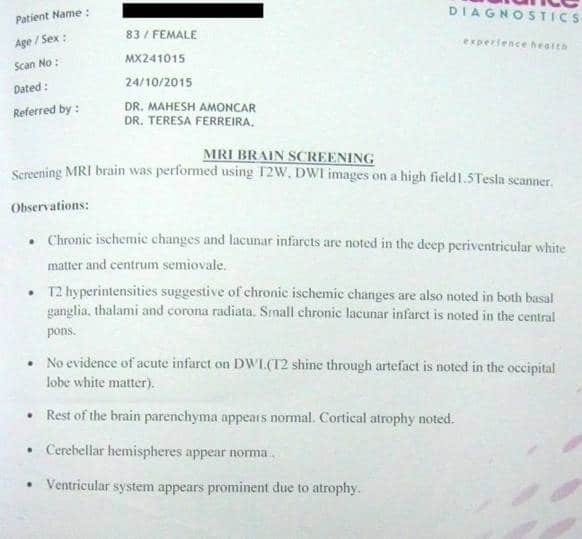
Prior to this episode she was leading a perfectly normal life, reading newspapers, attending to her household duties, socializing, etc. While being transported to the hospital she turned stiff, exhibited foaming around the mouth, and lost consciousness, suggestive of seizure. At the hospital her ECG was normal. Since she was unconscious, she was treated by Dr Teresa Ferreira, a neurologist and Dr Mahesh Amonkar, who was their family physician treating her asthma. The patient was found to be suffering from encephalitis of unknown origin and continued to remain unconscious despite all efforts of doctors of conventional medicine for the next 20 days.
On the 21st day with the kind permission of the doctors and the unconditional faith of the family members, I was asked to examine the patient at the hospital. She had been in the ICU connected to the ventilator for the last 21 days. I observed that she was lean, fair, completely emaciated, stoop shouldered with long delicate fingers. (Tubercular constitution). Her tongue was hanging towards the right side. On auscultation of the chest I found crepitations all over the right lung with reduced air entry. She appeared to be in deep sleep as if intoxicated. Her carotids were throbbing. Her head, neck and extremities were hot to the touch but she had no rise in temperature. Her pupils seemed dilated. The neurologist had put the patient on antiepileptic medications because the EEG showed continued seizure activity without any external manifestations.
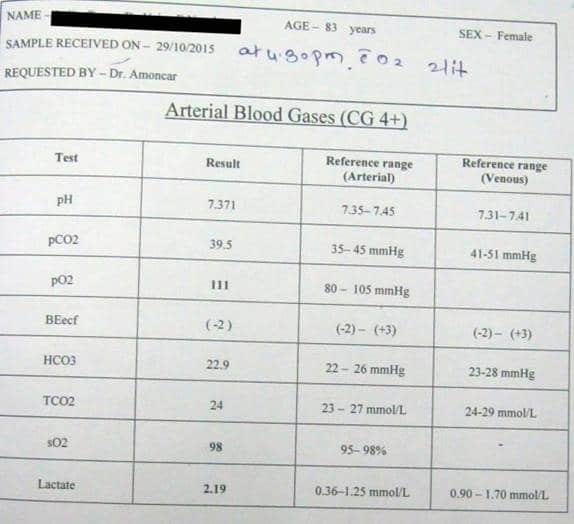
My prescription was Belladonna 200, 1 globule mixed in water and few drops were given on the tongue. The result was seen immediately by everyone, because the patient opened her eyes. Next morning she began to move her limbs. She was trying to speak but nobody could comprehend her due to the tracheostomy. She was smiling too and seemed to look alert about the surroundings. As each day passed more improvement set in and on the third day she could sit on the bed, of course with the help and support of the physiotherapist. The pCO2 which was initially 58 and marching towards respiratory failure reduced to 44 and the readings were still lower during the first 24 hours after administration of the remedy. All doctors and nurses in the hospital were thrilled to see this good development and the neurologist told the family to please continue giving homoeopathic treatment.
On the fourth day again Pco2 levels rose, so once again Belladonna 200 was repeated and there was immediate improvement. After another 4 days the condition again seemed to worsen, so Belladonna was repeated.
0n 26th September the patient seemed not to respond Belladonna 200, so anti-miasmatic Merc Sol 200 tds for 1 day was given. After 3 days belladonna was repeated and it worked. The doctors observed that they could wean this patient off the ventilator although earlier they had announced to the patient’s family that once a person is on a ventilator for 15 days he becomes dependent on it for life. Her oxygen saturation improved to 95-96 even without oxygen.
On 6th October her heart rate rose from 66 to 84 and respiratory rate was 31 per minute so the pulmonary specialist put her on a steroid. The first 48 hours was seen to be encouraging but thereafter complications followed.
On 11th October I was called again because her eye seemed to be squinted. She was gazing fixedly in one direction towards the left. There was a redness and blush on her face. Blood pressure rose to 200/100mmHg so she was put continuously on IV’s. Her consciousness was getting worse, as the Glasgow coma scale showed about 7 points. She was having involuntary movement of the left upper extremities moving the opposite side of the neck; her mouth was open all the time. Saliva was drooling from the right angle of the mouth. Neck was rigid. Right pupil was smaller than the left. A dose of Helleborus Niger 10 M was administered mixed in water. Result was immediate improvement of her consciousness within the first hour of administration. Eye contact improved and she responded by nodding her head. Blood pressure normalised to 110/80mmHg.There was progressive improvement noted in the rigidity of the neck and extremities. Patient was completely off the ventilator.
It was noted that chest secretions had increased and become whitish. This patient was shifted to another hospital in Panaji (Trinity Hospital) in a separate room with well-ventilated window because she was getting unnecessary problems due to unhygienic conditions in the ICU of the previous hospital ( which resulted in recurrent chest infections.) Dr Vikram Dalvi took over the case in consultation with the same neurologist at Trinity hospital.
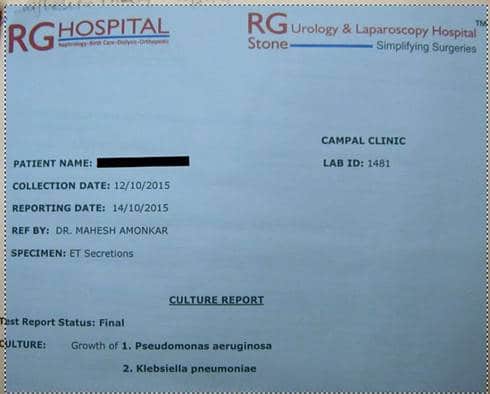
On 15th October in the new hospital the tracheal secretions were found to be positive for pseudomonas.
On 22nd October patient had excessive secretions in the mouth and repeatedly sputum examinations showed Staph Aureaus and Klebsiella. X ray showed infection in right lung. Stool showed occult blood. Developed fever 100 F, blood pressure 106/48 mmHg, ABG 41.4, heart rate 97, respiratory rate 29. S. Creatinine 1.3.
I prescribed Phosphorus 200 1 dose mixed in water. The result was rapid. Fever reduced, secretions became thin and lime coloured, she passed very offensive green watery soft stool four times.
On 26thOctober C.T Scan of chest showed a small, old pneumonic patch. She passed stool 10 times last night. No fever, Respiratory rate 32, awake and appeared worried.
On 27th October The doctors at the hospital could not do anything to help this patient because they had already given all the possible antibiotics previously and the patient was no longer sensitive to these. Heart rate 84 per minute and respiratory rate 37 per minute. Patient was experiencing suffocation due to excessive secretions. Crackles in both the lungs.
I prescribed Baccilinum 200, 1 dose per day for 3 days. Result was rapid. Her demeanour was good the next morning; suction needed to be done just once last night. Gaze normal. Slept well. Fully awake and mouthing words. Not much whitish secretions. No loose motions. Progressive improvement day wise.
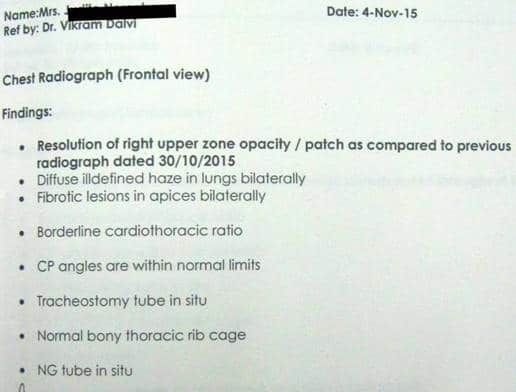
On 4th November Xray showed resolution of right upper zone opacity as compared to 30-10-15. Oral secretion reduced to minimal.
Next visit was On 30th November at Trinity hospital. The Glasgow coma scale scored 10 points. S. Creatinine reduced to 1.04 as compared to 1.17 on 18th November. It was observed that patient was drowsy throughout the day. Eyes were staring on the left side all the time. Left eyes remained half open while sleeping. Sleeps with mouth open. Upper limbs were very rigid and in flexed mode. Right palm could be opened but not the left palm. Knees could be flexed. Neck was very rigid. Tracheal secretions were thick white. On auscultation right lung had ronchi and left lung had occasional crepitations.
I prescribed Hyoscyamus Niger 200, 1 single dose. Result within 24 hours: her limbs became soft and very light to lift. Her demeanour looked good. Sensorium good: responding, taking initiative to say something, looking around normally. Her physiotherapist reported that she has seen improvement now as compared to the last 10 days. As days went by, her limbs appeared better and her comprehension and connection with environment improved. Speech became meaningful, clearer and even comprehensible. Mouth closed and fine movements better.
On 6th December the EEG was repeated. It showed no abnormal activity, so the neurologist reduced her dosage of antiepileptic medicines.
Since patient was improving on 15th December tracheal tube was removed, after which her secretions became minimal. Sensorium was okay and Sp02 was 93.
On 19th December the tracheal wound was closed.
On 21st December patient was discharged home. She was home to celebrate Christmas with her loving family.
Next visit on 6th January 2016 at home in Panjim. Patient asked for tea and soup, responded to grandchildren. She used to sleep more and cough a lot. Takes hand to throat while coughing, tries to turn and lie on the left side. Glasgow coma scale had scored 13 points. Neck stiffness less than previously. On auscultation expiratory ronchi on the left lung. Expectoration is thick white in the morning then thin in the day. I prescribed Bryonia Alba 200, 1 single dose in water. The patient said “Thank you” to me. Result: Secretions increased considerably and had to be suctioned every few minutes. She asked to be taken to veranda on her new wheelchair and asked for dal. Her hunger increased.
On 21stJanuary 2016 patient suffered another generalised tonic clonic seizure lasting for 1 minute, pulse was fluctuating, developed hard breathing. Patient was put on 4 lit oxygen, 8 times suction. Heart rate 88 beats per minute. Doctors found urinary infection which they started treating. On the same day her daughter in law delivered a baby girl in the same hospital and patient’s face expressed happiness.
On 1st February I observed that Glasgow coma scale was scoring 9 points. On auscultation air entry had reduced in left lung. Expiratory wheeze was heard. Patient seems comfortable in sitting upright. She had complained of heat a few days ago and no thirst. Pulse was 95b/min. respiratory rate 30b/min, spo2 98 on 2 lit oxygen. My last prescription was Pulsatilla 200 single dose in water. Result: the first 2 days X ray showed improvement but on the third day the lungs began worsening and even the right lung was going for collapse. So the family was informed that the patient was dying and advised to give only conventional medicine because patient stopped responding to homoeopathy for the first and last time in her life.
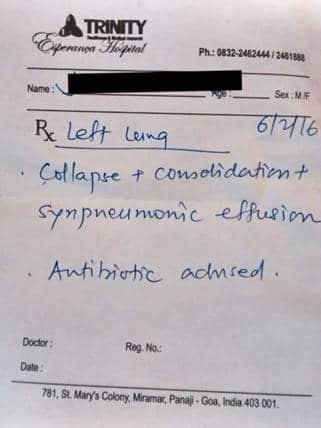
On 6th February 2016 X-ray revealed left lung collapse with consolidation with synpneumonic effusion. And doctors advised antibiotics.
Patient passed away on 11th February at 7.15am in the hospital.
What could homoeopathy offer this case?
She was recalled to life by homoeopathic medicine and she could learn of the birth of her new granddaughter. She could once again enjoy all the pampering from all her 5 children and grandchildren and second life brought glory for the homoeopathic science in Goa.
In the above case we observe with every following action of the remedy, the miasms begin to move one by one. Here we saw that it shifted from deeper organ to less deeper organ (from brain to lungs), from lungs to urinary organs, from lungs to excretory organs. We have to keep a track of them. Sometimes they discharge, come out in the form of diarrhoea and expectoration. Ultimate relief is with psora; if she makes a psoric aggravation, especially when you are treating a syphilitic case, that’s many jumps from syphilis to psora. Shifting is an action of the medicine from more important to less important organs. Watch it carefully. These reactions have to be well kept in mind while analysing the reaction to a homoeopathic remedy. Here the syphilitic miasm was extremely difficult to tame. It was so destructive and rapidly growing that it left us very little time and chance to fight it.







DEAR DR,
THE CASE WAS VERY DIFFICULT. IT WAS DIFFICULT TO REPERTORY IT. THE VITAL FORCE WAS WEAK AND FURTHER WEAKENED BY STEROID AND ANTIBIOTICS GIVEN IN HOSPITAL. ANY HOW YOU MADE EFFORTS
THANKS