Preliminary History: Male child, 8 yrs, middle class
Acute History:
An 8yr old male, only child of educated parents, was brought to the Homeopathic Hospital OPD carried in by his father. This family had never taken homeopathy before. The chief complaint was of frank and large hematemesis. He had had a history of similar episodes in the past, every year about the same time. Sclerotherapy had not helped prevent these bleeding episodes. They recurred periodically every year.
The acute picture was as below:
Frank profuse bright red bloody vomiting 3- 4 times a day
Passing dark tarry stools 3-4 days prior to vomiting
No history of abdominal pain
No history of having consumed any substance
H/O He had a history of 3 similar episodes in the past. The sequelae, inspite of conventional management was circulatory collapse with dyspnoea and he had to be revived with blood transfusion and life support systems (ventilators and ICU management). Each episode lasted for three to four days, before he recovered enough to be taken out of ICU.
Past history
Obstructive jaundice at the age of 1 yr
Milestones delayed. He was a chilly child and craved sweets.
k/c/o Childhood Cirrhosis with varices and episodes of hematemesis
Examination:
Category II Triage
General condition satisfactory, clammy skin
Heart rate 130/min
Respiratory rate 43/min
Per abdomen : Liver and spleen palpable.
Investigations:
• TC : 10,000
• Hb : 4 gm%
• Platelet : 1.4 Lakhs
• B.T : 4.14/sec.
• C.T : 3.10/sec.
Diagnosis:
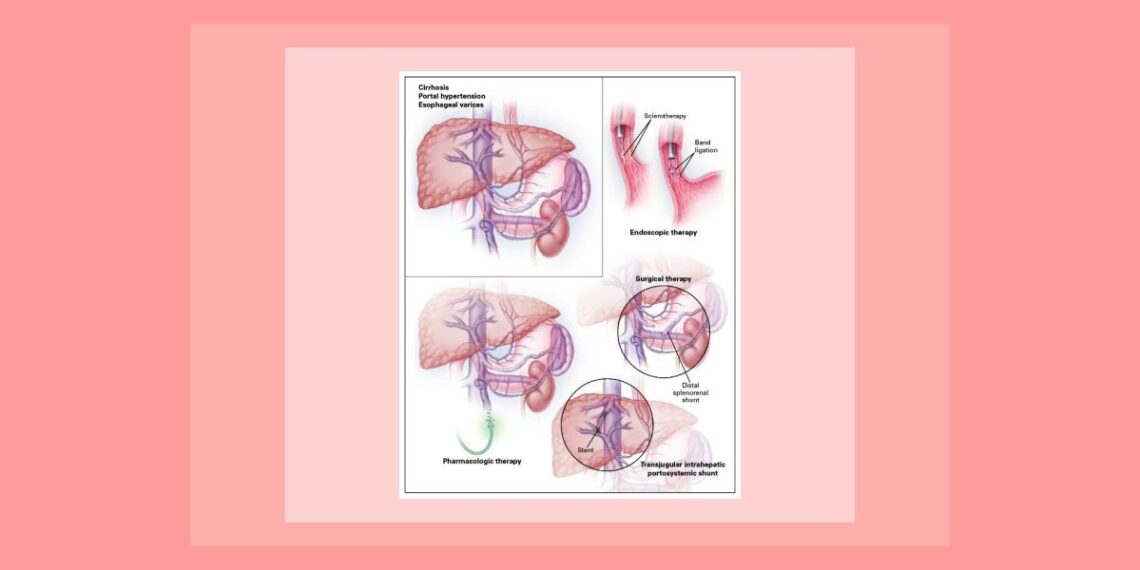
Gr. II – III Oesophageal varices with portal hypertension due to cirrhosis of liver and splenomegaly presenting with hematemesis and impending hypovolemic shock.
Totality:
The focus for constructing the totality in this emergency is based on the history obtained of sequelae to these same set of symptoms in the past. There are no characteristics to indicate a simillimum except the annual recurrence of symptoms. The patho-physiology behind the episode that leads to circulatory collapse and shock would hence be important components of the remedy to be chosen. The constitutional symptoms help for further differentiation of a group of remedies covering the pathological presentation. Hence the totality consists of:
1) Annual aggravation
2) Location, liver, blood
3) Pathology and degeneration, destruction, hemorrhage, shock
4) Craving sweets
5) Chilly patient
Susceptibility assessment
Pace of disease : moderate
Pathology : degenerative liver- irreversible with complication of varices
Characteristics : few, only pathological symptoms
Sensitivity : low
Dominant miasm : tubercular (bleeding, degeneration, shock) with syphilitic background.
Correspondence : based on pathological generals, venom group
Plan of Emergency Management:
Given this assessment, we see that the vitality is very low and susceptibility is very low. He needs to be revived at any time if he slips into circulatory collapse; he still remains in a compensated phase though he could decompensate anytime. The choice of potency hence is low, single dose and very cautious repetition to avoid fatal aggravation that may present either with increased hematemesis or decompensated circulatory collapse. The remedy should also cover the tubercular /syphilitic miasmatic pathophysiology.
Crot. horridus 30C, cautious repetition
Assessment after each dose
Ancillary Measures:
All precautions to prevent circulatory collapse:
Head low position
Intact IV line
Oxygen
IV infusions to maintain plasma volume
Follow up:
He had only one episode of vomiting after the dose of Crot. H 30C. He had no vomiting the following days. His heart rate reduced and peripheral circulation stabilized thus preventing his further deterioration into hypovolemic shock. He had no complaints thereafter. He was followed up for more than one year after this to watch for repeat episodes of hematemesis. He had no further episodes, which meant that the annual aggravation had also been prevented.
Discussion DC26:
Establishing Clinico-pathological correlations:
Pathology progression, degeneration of liver (cirrhosis), destruction of muscular layer of circulatory (venous) system due to backpressure at varices resulting in hemorrhage and shock.
Knowledge of this should be correlated with the same in terms of remedy pathogenesis. Snake remedies have a similar pathological evolution and hence are indicated in this pathology.
Copperwaithe states: “GENERAL ANALYSIS.
Like other serpent poisons, Crot. acts primarily upon the cerebro-spinal nerve centers, producing secondarily decomposition of the blood, a destruction of blood fibrine, hemorrhages, ecchymosis, etc”
Importance of the Time dimension / evolution in the case:
The case itself has presented in a stage of irreversible pathology. Treatment is basically symptomatic and palliative. The focus is to prevent further bleeding from the varices and prevent incipient shock.
Quick clinical assessment and monitoring of vital parameters:
In the emergency presentation the focus is on observing and controlling the onset and development of shock. Appropriate vigilance and monitoring of the heart rate, blood pressure and hematemesis (loss of blood volume) with knowledge of ancillary measures required are important parts of management.
——————————————————–
Dr. Navin Pawaskar, MD (Hom)
Director, Clinical services,
ML Dhawle Trust and Organizations