Case: 6-year-old boy with multiple tics
On March 7 of this year, a young mother presented her 6-year-old son to me. He was still in preschool, but should have started school last year, but was put on hold. During the enrollment test, the school doctor and principal recommended that he be referred to a special education support center, which the parents refused to do.
It was noticed that he had multiple tics and ADHD was diagnosed, which was confirmed by the child and adolescent psychiatrist who was called in afterwards. He pronounced a tentative diagnosis of “incipient Tourette’s syndrome.” He prescribed Ritalin, which the parents did not want to give at first and therefore came to see me.
The mother said that she and her husband had never noticed this, that he was a smart child with whom one could talk very well, and that he only had to overcome this hurdle now and manage to start school normally this summer. It is noticeable that the mother has fused eyebrows and stutters.
Otherwise he is never sick. The last three years he was completely free of infections, had only once a slight cough. As for the tics, the mother says, “He bounces a lot, clears his throat all the time and sniffles, sometimes eye rolls, sometimes shoulder rolls.” “And this one,” the boy says, coming very close to my face, twitching his eyes and grimacing.
He talks very coherently, smartly and a lot, is very attentive and not at all shy, but very restless and very quick in his reactions. Conspicuous: frequent toe walking.
The mother further reports:
“The tics are involuntary. When he does something, then hardly, in the evening when he gets tired, they are strongest, the more exhausted he is. In the morning not at all. Sometimes he points at something or makes shoulder rolls or eye movements.
Every week it’s different, wave-like. I haven’t found a pattern yet, it’s just sometimes more, sometimes less. Right now mostly at home, in the evening, on the sofa. One movement he gives preference to for maybe a week, he then does it pretty monotonously, like a loop. If you distract him, he’s out again.”
“There was a phase when he flattened his nose with his finger, really badly – that was for a week, then it was gone again. He does a lot of toe walking and clearing his throat, then there was a phase where he pointed a lot – at the sky, at birds or mostly at nothing at all. That happened pretty quickly. He coughs a lot.”
“It all started when he was 3 or 4 years old. We never noticed it, we never noticed that he couldn’t say R, he always said U. Then went to speech therapy, then it got better.”
He does “discharges” – looks at a book and goes “pfffft,” like a gun. He has no interest in other kids. They don’t bother him, but he doesn’t play with them either. At preschool, there are requirements to play with other children; he does that for a few minutes, then stops.
Pregnancy and birth were unremarkable. He has received all the usual vaccinations. As a toddler, various mild infections, twice given antibiotics. When asked about other noticeable tics in the family and after I asked the mother about her stuttering, she says, “My husband also has tics like that and is restless – always wiggling and fidgeting with his foot. He also pulls out his eyelashes without realizing it. It’s also like sometimes he doesn’t have any at all.”
In terms of food cravings, the only thing that stands out is that he doesn’t have much of a craving for sweets, but eats a lot of fruit and drinks so much that he has already been screened for diabetes. He himself interjects, “Since I broke, I drink less.”.
The boy is constantly on the move in my practice – his urge to move even extends to the garden. His movements, however, are purposeful and he listens attentively to what is spoken, interjects a remark more frequently, by which one can see how quick and well developed his mind is and how high his actual attention is.
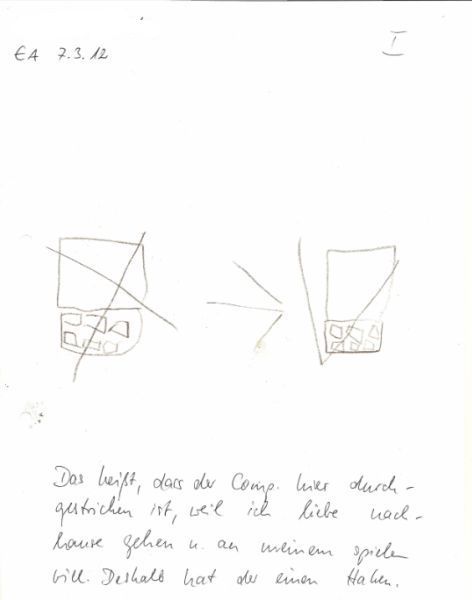
Nevertheless, he seems to get bored quickly in the anamnesis situation – which he communicates in a very indirect and non-confrontational way: He draws alternatives!
Fig.: Drawings of the patient followed by analysis:
Analysis
I must confess, I do not repertorize in every case. Here we could do extensive repertorizations, dissecting the individual tics – and would probably get into the woods, as so often happens with mechanical repertorizations and lack of case understanding. I only looked in this section:
Mind – gestures, gestures; makes – tics; nervous.
agar.mtf11 arg-n.bro1,ptk1 ars.ptk1 bism-met.zzz carc.jl2,mrr1,mtf33 caust.mrr1 croc.mrr1 cupr.mrr1 enterob-v.zzz hyos.bro1,ptk1 ign.mrr1 laur.bro1,ptk1 lyc. bro1,ptk1 nux-v.mrr1 ran-b.ptk1 rhus-t.mrr1 sep.bro1,ptk1 staph.mrr1 stram.mrr1 syph.jl2 tanac.mtf11 tarent.bro1,ptk1 Verat.mrr1 zinc.bro1,mrr1,ptk1
Bird’s eye view
We are dealing with what I consider a highly gifted 6-year-old who is largely emotionally healthy and unremarkable, but neurologically and affectively disturbed. He is friendly, affectionate, cuddles with his mother, expresses himself well, has an extremely quick grasp of things – and in some ways discharges of his nervous system that express themselves in the tics I mentioned and also definitely his restlessness.
I am glad and grateful to have studied with George Vithoulkas for so many years, after all, when I saw this combination of symptoms, what immediately came to mind was George’s description of Veratrum album:
Idea of overstimulation. They notice things, perceive things. Twist in their mind coming out of their feelings into the physical body. They want to do something special: We walk one foot put in front of the other, they try a new step. Thoughts: back and forth, back and forth. Eyes: right and left, before turning the head.
Excessive restlessness – children in practice are never still. Quick minds. They are very brave. Attack authority figures. Others admire them for it. But underneath there is always an element of self-expression. They always twist.
After his descriptions, Vithoulkas told the story of a 5-year-old boy who was visiting him and playing with other boys: they were screaming loudly and constantly running up and down the stairs. The 5-year-old was the smallest. At one point, Vithoulkas yells, “That’s enough!”. Everyone is immediately quiet, only the 5-year-old props his hands on his hips, builds himself up and says, “Who are you? You want to forbid us to play?!”
In our case here, this self-confidence, independence and not recognizing authority can definitely be compared with drawing the actual situation and the alternative he chose. The precociousness is also known for Veratrum.
The few other noticeable general symptoms are the extremely strong thirst for cold water and the strong desire for fruit, which is unusual in a child of this age. Both of these are confirmed by the remedy.
I always involve the patients very much in my analysis of their case and also explain to them what I would expect in terms of reactions. In this case here, I explain to the mother that what needs to be treated in her son is on the neurological-emotional level (tics).
For a patient’s own case understanding and understanding of their own case, it is important to create a treatment hierarchy. What is the thing to be treated and why? Where is the patient most deeply ill? What should change urgently and as soon as possible in the case progression? What can or should get worse and why? Simply: where is the journey going?
In this case, it would be desirable if the tics improve first (nervous system) and in the further course (which certainly takes longer) the behavioral problems (ADHD symptoms, social disorder: no interest in other children).
If you explain this to the patients in exactly the same way, they have a “route planner” in their hands and can subsequently observe more precisely what changes at which level.
Since I conduct the patient conversations in such a differentiated way, I hardly ever have a follow-up appointment where the patients open the conversation with the sentence: “Nothing happened at all.”
Prescription and course
Prescription –Verat. C 200 fractionated
With Tjado, I have learned that in cases where I do not expect strong initial reactions, I should have the remedy that I am quite sure of taken fractionated and “findings-oriented”. So I told the mother to dissolve the remedy and give 3-4 doses daily for a maximum of 3 days, provided there are no new reactions or exacerbations. If this is the case, stop taking it immediately.
The mother emailed me two days later that the young patient had developed a flushed head and sweats immediately after the second dose. She then discontinued the drug.
Follow-up from 3/28/12
Forms to be filled out:
B How is your general well-being or your attitude to life? How do you get through everyday life and work (for children: school)?
C What is your state of mind or mood?
D How is your sleep?
%) Since when do you sleep better? For days, weeks.
E Have any new complaints arisen? If yes, please note which ones and since when:
1.
2.
3.
F Did any old, previous, past complaints return? If yes, which ones?
G Did the symptoms worsen after taking the medication?
If so, what was it?
When did it occur? According to
For women: How did their menstrual period behave?
Normal ü Following:
Did your sweating or perspiration change? If yes, in what way? eo.
Were there any changes in the skin? If yes, what were they?
K Did any special secretions, including previously known ones, occur? If so, which ones?
L Did your craving for or aversion to certain foods change?
Follow-Up Questionnaire
Name: John S. Datum:
Dear patient,
To evaluate the result of the last remedy I request you to answer the following questions before each consultation and to make a cross for your answers. Please use simple words and avoid specialist terms. If your complaints (symptoms) are better now, please fill in how many percent you feel it is better (i.e.: headache 70% better). If there is not enough space, please take an additional sheet. Thank you for your efforts!
Complaint resp. symptom is: Better = B / Unchanged = U / Worse = W
Please name the ailment(s)for which you decided to seek treatment:
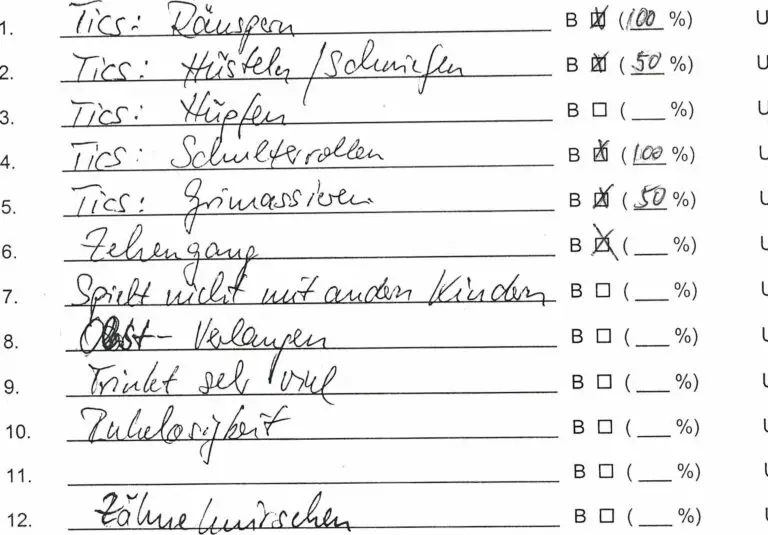
Right at the beginning she says that almost all tics would have disappeared right after the remedy. As expected, the intensity of ADHD symptoms and contact disorder remained pretty much the same.
Furthermore, she reports:
“He sleeps a lot better and is great in the morning. Overall, he seems a little calmer. He doesn’t grind his teeth anymore! That’s weird.” (Hadn’t told me at case intake).
“Since he started sweating as an initial reaction and had that red head, he hasn’t had that at night! He used to have that all the time.” (Hadn’t told me.)
I explain to her that it would be desirable if her son, associated with further improvement of his neurological symptoms, could develop an infection and/or fever and that she should not give him anything then.
Follow-up on 5/23/12
“For the first time in three weeks he has had a real cold, quite a cold, he also had a cough, which is now gone. Especially in the morning, it’s really coming down.”
He also had some temperature in the evening and was tired and still sleeps a lot. In the morning, a green-tough secretion comes out of the nose, during the day it becomes clear-bright.
The mother says on her own: “I think the globules are still working. He seems much calmer than before. He has also become more affectionate, he often comes here to hug, he never used to do that. Also comes to bed more often at night, he never did that.”
When asked:
Tics:
“Are gone, only very rarely when he is tired at night.”
– Clearing throat: “Completely gone.”
– Coughing/sniffling: “He has a cold now! But doesn’t sniff conspicuously.”
– Shoulder roll: “Not at all.”
– Grimacing: “No.”
ADHD/contact disorder:
– Fidgetiness: “Got better, fine during the day, just back in the evening for the last half hour.”
– Bouncing: “Still does. When he is happy e.g. But gets less over the day and in general.”
– Toe walking: “He still does. Nothing has changed there.”
– Other children/social contact: “He now has a friend for the first time, also makes an effort to have contact with other children, seems to be a bit better, but he needs a lot of time for himself.”
– Teeth grinding: “When he’s in the phase between waking and sleeping, he still has it sometimes, but it’s not bad anymore.”
Every two weeks, he’s in a child psychology office playgroup. There, he says, it was extremely noticeable that he was suddenly free of tics, and when asked by the psychology team, the mother indicated that he was now receiving homeopathic treatment.
The boy says to me when we say goodbye: “At one point in a ghost story I’m scared. Can you do something there too?”
Current supplement
After finishing the article (end of June), I asked the mother’s permission to publish it. She emailed me back:
“Hi Mrs. Hill,
I wanted to write to you today anyway: for three days now, T. has been playing much more openly with other children, so much so that two teachers from his preschool have already approached me enthusiastically! Obviously a barrier has been loosened – isn’t that wonderful?
I would totally love it if you mentioned T.’s case ….
Could I then maybe have/purchase a copy of the magazine?
Enjoy your article and have a great day!”