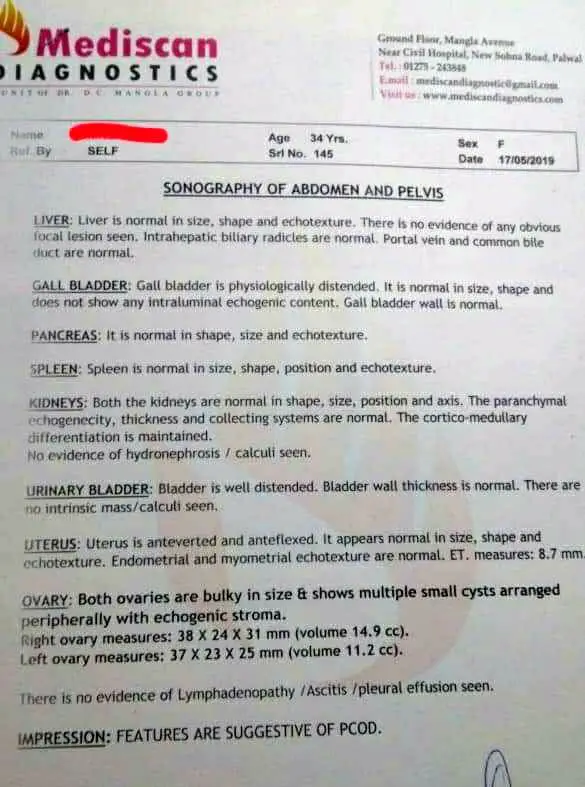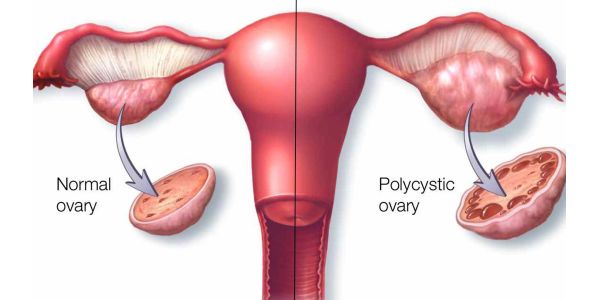
This is a case of polycystic ovarian syndrome in a female of 34 years. The patient was seen for the first time in February 2019. She presented with irregular menstruation with very scanty menstrual flow (at times reduced to a drop of blood only). She also complained of pain in the lower abdomen and back during menstruation.
PHYSICAL GENERALS
Thermal – Averse to extremes
Thirst – Good amount of water, 5-6 liters
Appetite – reduced lately
Desires – Earlier, spicy and sour
Aversion to – sour and sweets because of teeth sensitivity.
Tongue – bluish discoloration, imprints of teeth, catches under teeth.
Stool- occasionally costive, with very little urge to pass stool.
Urine- reduced as compared to her fluid intake. Earlier had a desire to urinate after having fluids of any kind, especially tea.
Sleep- Disturbed of late
Dreams- trains, snakes, climbing, slipping
PATIENT AS A PERSON
- Build – mesomorphic
- Irritable mood.
- Indolent, with no desire to do any exercise. Keeps lying in bed for most ofthe day.
- Has always been very competitive.
- Averse to coitus because of some differences with spouse. No physical intimacy since last few years (suppressed libido).
OTHER CONCOMITANT SYMPTOMS
- Sensitivity of vertex
- Teeth sensitivity to sour and sweets.
- Irritating cough.
- Rashes on inner thighs with severe itching which disturbs daily activities (developed during the course of treatment). Itching, worse from sweating. Her husband also has similar rashes on inner thighs.
- Irritating cough
ON OBSERVATION
The moment the patient entered the clinic she had a curious expression on her face. After I enquired about the case, she wanted to be doubly sure that I had understood her disease and that I would be able to prescribe for it. I perceived this as a suspicious nature and verified it by asking if she doubts her friends and husband, to which she agreed.
PRESCRIPTION
The patient was prescribed Lachesis (in ascending LM potencies up to 0/15).
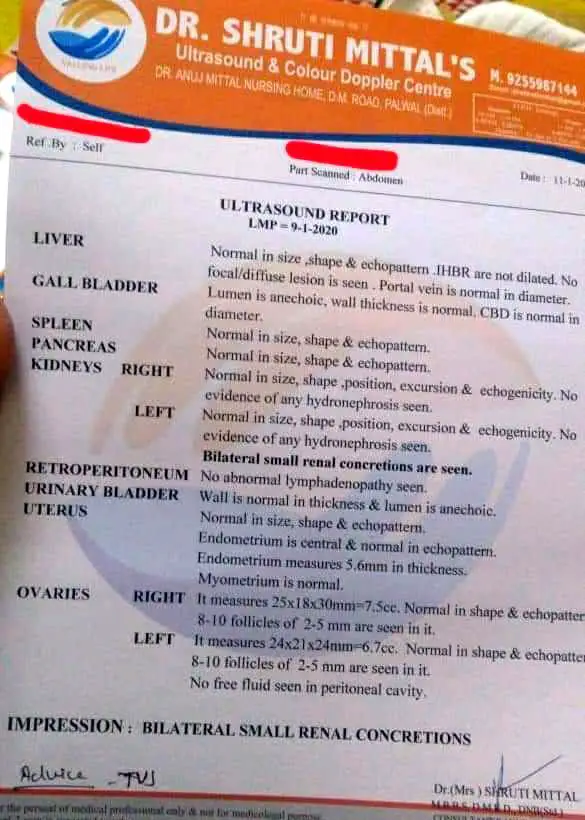
The ultrasound scan done on 11th January 2020 showed restored ovarian morphology. The scan showed small renal concretions which was movement of the disease from the more important (fifth- endocrines) to less important disease plane (second – endoderm).It is also the conversion of a static sycotic pathology (polycystic ovarian syndrome) to a dynamic sycotic pathology (renal concretion), showing the process of gradual release of the sycotic build up (sycosis = accumulation).
The patient developed fever, coryza and rashes on her inner thigh during the treatment but unfortunately resorted to allopathic treatment which kept on suppressing the disease and it took longer for the pathology as well as the patient to heal.
(see ultrasound reports below)