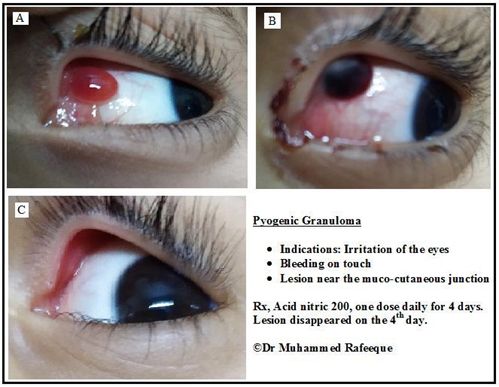
Master E, aged 5, was brought to me complaining of irritation and bleeding from the left eye due to a pyogenic granuloma inside the left upper lid. It was moving freely with the movement of the eye ball, which was producing pain the last five days.
There was mild fever and inflammation of the conjunctiva. They already visited an eye hospital, where doctors had suggested surgical removal the next day. As the family was not willing to do that, they consulted me.
On examination, pyogenic granuloma was found, with bleeding on touch. Irritation in the eyes, bleeding on touch, lesion near mucocutaneous junction lead to my prescription of Nitric ac. 200, one dose daily for 4 days. The next day the granuloma became dark red, and bleeding was still present. On the 4th day, the lesion disappeared.
Pyogenic Granuloma
Pyogenic granuloma (PG) refers to a benign vascular proliferation of immature capillaries that is neither purulent nor granulomatous and is also called lobular capillary hemangioma. PG presents as a lobulated raised lesion within the conjunctiva.
Associated conditions
Although there are several predisposing factors, pyogenic granuloma is most commonly seen at a traumatic wound site or near a suture line after surgery for chalazion, pterygium, strabismus, retinopexy[1], enucleation, or other ocular insults[2]. Rare cases have been reported of PG formation secondary to ocular acne rosacea [3][4] and soft contact lens wear.[5]
Pathology
PG is thought to represent an abnormal wound healing reaction. Microscopically, PG consists of aggregations of immature blood vessels and fibroblastic stroma, much like granulation tissue, with accompanying lymphomcytes, plasma cells, and scattered neutrophils. Early lesions have numerous capillaries and venules with prominent endothelial cells arrayed radially toward the epithelial surface. The mature PG exhibits a fibromyxoid stroma separating the lesion into lobules. The epithelial surface exhibits inward growth at the base of the lesion. A regressing PG has extensive fibrosis.
The American Academy of Ophthalmology’s Pathology Atlas contains a virtual microscopy image of Pyogenic Granuloma .
Diagnosis
Symptoms
Some discomfort or irritation may be felt depending on location of the PG. The lesion will bleed with very little trauma.
Physical examination
Rapid growth usually lasts a few weeks. This condition usually follows an ocular insult and presents as a slowly enlarging fleshy vascular mass. It ranges from a sessile, broad-based lesion to an abruptly elevated growth. PGs are often pedunculated, with an underlying stalk of feeder blood vessels and connective tissue[2]. The surface may be rough and friable with a tendency to bleed easily. Elevation of the margin with a cotton-tipped applicator often reveals the peduncle.
A chart review was conducted at Wills Eye Institute for patients with “vascular lesions of the conjunctiva”. Pyogenic granuloma was the second most common diagnosis after lymphangioma and lymphangiectasis [2]. Other common diagnosis that would be on the differential for PG are capillary hemangioma, acquired sessile hemangioma, Kaposi’s sarcoma, racemose hemangioma, varix, cavernous hemangioma, and glomangioma[2]. Clinical diagnosis, however, is usually straightforward. Rarely is it necessary to biopsy a pyogenic granuloma.
Management
Most PGs will resolve once the primary inciting cause such as a chalazion is treated. Lubrication with artificial tears and occasionally topical steroid eye drops can help with symptom relief. If the PG does not regress within weeks or is causing symptoms, simple excision can be curative. Shaving, followed by cautery and cryotherapy, is the most common practice, but recurrence is not rare[2]. Low-dose plaque brachytherapy can be used if the PG has multiple recurrences[2].
https://eyewiki.aao.org/Pyogenic_Granuloma
References
Damasceno EF, Pereira C, Damasceno NAP, Horowitz SAP, Amaral Filho, Octavio Moura Brasil. Pyogenic granuloma after retinal detachment surgery with scleral buckle: case report. Arquivos Brasileiros de Oftalmologia. 2009;72:543-544.
Shields CL, Shields JA, Mashayekhi A, et al. Vascular Tumors of the Conjunctiva in 140 Cases. Ophthalmology. 2011;118:1747-1753.
Rahman, Mamun Q., et al. “Fibrosing Blepharo-Conjunctivitis Following Pyogenic Granuloma in Ocular Acne Rosacea.” Ocular Immunology and Inflammation, vol. 18, no. 5, 2010., pp. 346-348doi:10.3109/09273948.2010.501945.
Rahman MQ, Lim Y, Roberts F, Ramaesh K. Fibrosing blepharo-conjunctivitis following pyogenic granuloma in ocular acne rosacea. Ocular immunology and inflammation. 2010;18:346.
Horton JC, Mathers WD, Zimmerman LE. Pyogenic Granuloma of the Palpebral Conjunctiva Associated with Contact Lens Wear. Cornea. 1990;9:359-361.