
Abstract:
This is a case of 12 year old girl who suffered from agonizing back pain with inability to walk without support. MRI of the cervical spine showed pathological changes. She had a history of ground level fall (GLF) from slipping. The orthopedic surgeon advised surgery to overcome the condition. This patient recovered well after homeopathic treatment without surgical intervention. This case shows the effectiveness of homeopathic medicines in providing symptomatic relief and improving the pathological findings, and doing so gently and harmlessly.
INTRODUCTION
Falls are the number one cause of injury1. A ground level fall (GLF), or a fall from a lower height than a GLF, is considered minor trauma and patients sustain less traumatic injury2. The most likely cause of a spinal compression fracture in those without osteoporosis is severe trauma, such as from an automobile accident or a fall from a great height3. Upper cervical spine injuries are frequent due to the increasing number of road accidents and falls. These lesions are often serious but neurologic complications are rare 4. Fracture dislocations of the thoracic and lumbar spine comprise less than 3% of all spinal injuries5. They may develop painlessly or cause agonizing localized pain that radiates around the ribs and abdomen. Multiple fractures lead to an increased thoracic kyphosis (‘widow’s stoop) 6. A key aspect that makes vertebral fractures so critical is that their presence greatly increases the risk of additional fractures7. Compression fractures of the thoracolumbar spine have a flexion compression mechanism of injury. This mechanism usually involves the first column (anterior longitudinal ligament and anterior half of the vertebral body). Pain is the main symptom; neurologic deficits tend to be quite infrequent, because such a fracture does not involve retropulsion of bone fragments into the vertebral canal8, 9. There is a bimodal age distribution among patients with spinal cord injuries: the first peak occurs in patients between 15 and 24 years, and the second in patients over 55 years of age10, 11.
Injuries to the spine include the bone (vertebrae), soft tissue and the spinal cord itself. All of these components are integrated and function together as a unit in health (and fail to do so in disease). Many times it is difficult to delineate exactly which tissue the injury affects. Luckily in homeopathy, we work from the patient’s symptoms, not the diagnosis, and thus can help many patients with various back injuries12.
CASE PRESENTATION
Miss Asima, age 12 years, was diagnosed with caries of the spine and paraspinal abscess by MRI Cervical Spine. On July 07, 2013, she was consulted for the homeopathic treatment of her back pain and associated complaints. She presented the following chief complaints at the time of examination.
Presenting Complaints
- Severe agonizing pain and stiffness of cervical, thoracic and lumbar region.
- Back pain aggravated by walking and long sitting.
- Patient had pain and trembling of right leg on standing and walking.
- Severe weakness of legs (especially right leg) and cannot walk without support.
- Patient felt feverish and Restless in bed in the night.
- Absence of menstrual flow for last 3 months.
- Excessive thirst for cold water.
- Over-salivation during sleep.
- Excessive sweating of palms, soles and body.
- Pain lumbar region with stiffness < waking on morning < long walking.
- Insensibility, arms, waking on morning, with stiffness and no pain.
- Poor appetite in morning.
- Des salted, spicy, fatty, cold drinks, ice cream,
- Desire open air.
History of presenting illness
Patient was alright 7 months ago when she had a ground fall by slipping. After a few days she developed symptoms of severe back pain and weakness of legs with restlessness. Her parents sought a medical opinion and the case was referred to a hospital where routine laboratory tests and radiological investigation i.e. M.R.I. of cervical spine were performed. The MRI report showing caries of spine and paraspinal abscess and she was advised for surgery by a consultant.
Past Personal History
- H/o Ground level fall during running.
PHYSICAL GENERALS
Appetite : Diminished
Thirst : Excessive for cold water
Desires : Salted, spicy foods, cold drinks
Bowel Habits : Normal
Urination : Normal
Perspiration : Excessive
Sleep : Restless
Thermal reaction : Hot patient
Observations
- Walking in stooping position.
- Trembling of right leg on walking
- Cannot sit for long time period without back support.
- Skin pale with dark hue.
- Tongue flabby and coated white.
RADIOLOGICAL INVESTIGATION
- M.R.I. CERVICAL SPINE
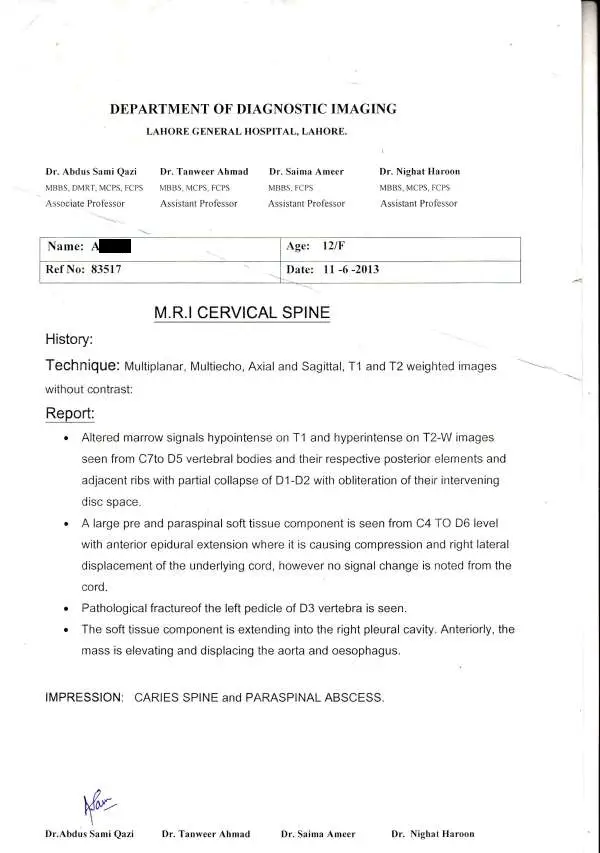
M.R.I. REPORT AT ENTRY
- Altered marrow signals hypointense on T1 and hyperintense on T2-W images seen from C7 to D5 vertebral bodies and their respective posterior elements and adjacent ribs with partial collapse of D1-D2 with obliteration of their intervening disc space.
- A large pre and paraspinal soft tissue component is seen from C4 TO D6 level with anterior epidural extension where it is causing compression and right lateral displacement of the underlying cord; however no signal change is noted from the cord.
- Pathological fracture of the left pedicle of D3 vertebra is seen.
- The soft tissue component is extending into the right pleural cavity. Anteriorly, the mass is elevating and displacing the aorta and oesophagus.
IMPRESSION: CARIES of SPINE and PARASPINAL ABSCESS.
RESULTS & DISCUSSION
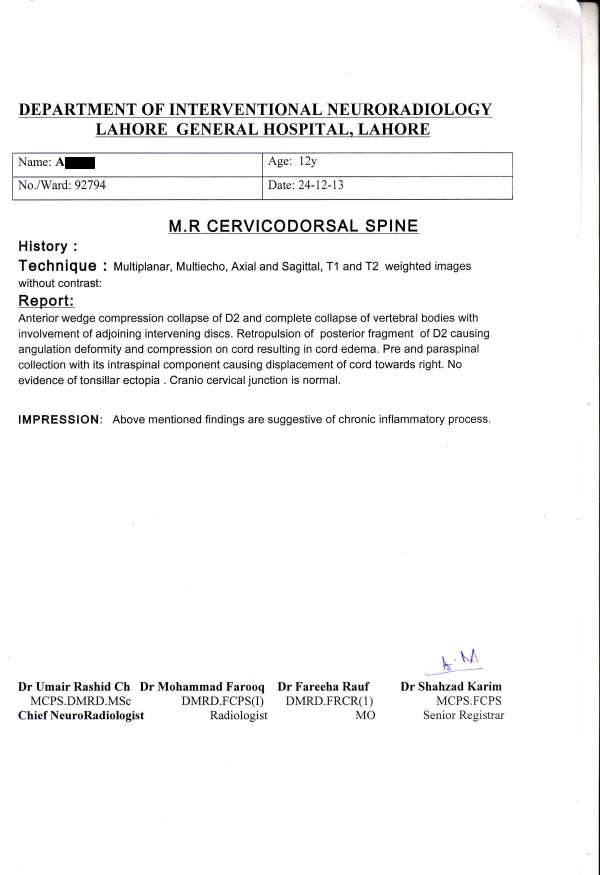
Treatment was started with Merc sol on the basis of its striking characteristics including profuse sweating with no relief, over-salivation with thirst, restlessness and a nightly aggravation. Merc sol in 30 potency started on 07-07-13 thrice a day. Within 2 weeks of treatment patient was getting immense relieved from pain and physical restlessness. The same treatment continued for 3 months because the patient was responding well and feeling better day by day. The patient started walking comfortably after 4 weeks. Menses appeared after 2 months. She received a dose of Merc sol 1M and afterward Pulsatilla 200 for reappearing mild back pain and some gastric problems. Medicinal treatment stopped and follow ups were with placebo. After 6 months, MRI Cervical Spine was advised. Results are very satisfactory (report attached). The patient stopped the treatment. After two months patient returned with lumbar pain with restlessness, better by motion. She experienced heat of soles and would patient uncover her feet. She received Sulfur 1M and afterward Rhus tox 1M. She is better now and still under observation.
REFERENCE
- Mosenthal AC, DH Livingston, J Elcavage, S Merritt and S Stocker (1995). Falls: epidemiology and strategies for prevention. J Trauma. 38:753-756.
- Runge M and G Hunter (2006). Determinants of musculoskeletal frailty and the risk of falls in old age. J Musculoskelet Neuronal Interact. 6(2):167-73.
- Lieberman IH and S Dudeney, MK Reinhardt, G Bell (2001). Initial outcome and efficacy of “kyphoplasty” in the treatment of painful osteoporotic vertebral compression fractures. Spine.15;26(14):1631-8.
- El Fatemi N et al. (2013). Upper cervical spine injuries: a management of a series of 70 cases, Pan African Medical Journal.15:57.
- Vialle R, L Rillardon, A Feydy, N Levassor, G Lavelle, P Guigui (2007). Spinal trauma with a complete anterior vertebral body dislocation: a report of three cases. Spinal cord. 46(2):154-158.
- Kumar P and M Clark (2009). Kumar & Clark’s Clinical Medicine, Seventh Edition, Elsevier Limited.
- Lindsay R, SL Silverman, C Cooper et al. (2001). Risk of new vertebral fracture in the year following a fracture. JAMA: the journal of the American Medical Association. 285: 320-323.
- Kim DH and AR Vaccaro (2006). Osteoporotic compression fractures of the spine; current options and considerations for treatment. Spine J. 6(5):479-87.
- Shen MS and YH Kim (2006). Vertebroplasty and kyphoplasty:treatment techniques for managing osteoporotic vertebral compression fractures. Bull NYU Hosp Jt Dis. 64(3-4):106-13.
- Barros Filho TEP, RP Oliveira, EK Barros, EF Von Uhlendorff, AS Iutaka and AF Cristante et al. (2002). Ferimento por proje´til de arma de fogo na coluna vertebral: estudo epidemiolo´gico [Gunshot wounds of the spine: epidemiological study]. Coluna/Columna.1(2):83-7.
- Cristante AC, TEP Barros Filho, RM Marcon, OB Letaif, ID Rocha (2012). Therapeutic approaches for spinal cord injury. Clinics (Sao Paulo). 67(10):1219-24.
- Morrison R (1998). Desktop Companion to Physical Pathology, Hahnemann Clinic Publishing, California.



we are hoping that she will recover completely..
May the doctor follow the case till she is recovered fully?
i’m trying my level best to follow ups until she achieved its maximum recovery.