It is axiomatic in mental health circles that treatment begins at the first phone call, possibly even before. Once a patient’s mind or heart reaches out for help, a certain healing has already been initiated. In this way, psychotherapy is very similar to homeopathy in that it accepts and utilizes the fact that all of God’s creation and therefore all healing is energetic. Thought and deed are not as distinct as we may have been led to believe.
This case began in the fall of 2009 with G’s intake. Thirty years old, she was referred by another client who told me that G was “falling apart.” G described herself the same way. Her voice quivered as she spoke. She couldn’t wait to get in to see me. She said, “I’m ready for this to stop.” I wasn’t sure what “this” referred to, yet, but readiness was a good beginning.
Spiritual, Mental & Emotional Status
G was born in Texas and at the time I met her she was a graduate student of psychology at a nearby university. She worked part-time in an internship and part-time in an unrelated job that brought in some money. She lived with her boyfriend of three years who was a doctor. Her mother lived in Texas. Her two siblings were in Colorado. When she came in, she walked straight into the office. She was slim, blonde, blue eyed, pretty and carried herself with a bearing and stride that suggested purposefulness and intensity. She was dressed appropriately for the weather and behaved appropriately in the situation. (No outstanding thermals or mental status red flags.) She made good eye contact.
“Please, have a seat,” I suggested.
She chose one quickly, sat forward at the edge of the chair and reached for the tissues. She was ready to either bolt or cry so I started with basics—some consent to treatment forms, her birth date, her current job, family members, boyfriend—and talked a bit about mundane things until she settled into the chair. When she finally did, I began to take her case with a simple question I learned 25 years ago in social work school: “So, what hurts?”
She answered quickly and emphatically: “Every damned thing!” She’d been suffering for quite a while, but what chased her into treatment was something that had transpired in school about a week prior. The students had been engaged in a role-playing exercise in which they were asked to do a reenactment of a suicidal teenager. She said, “I didn’t have to pretend! My daddy killed himself when I was in high school. He and my mom were going through a divorce. He was an alcoholic. He picked up booze again and he shot himself.”
As she spoke she held her head in her right hand as if it (and every thought it contained) were just too much for it to stay up on its own. She denied any head pain, but then talked about her father…
She could not remember details, but she had a vague body sense of something untoward occurring between her and her father when he was drunk and she was very young. She could not remember almost anything about herself as a child. She said, “I don’t know if anything happened literally. We were just very close. My mom was a safe person, but I was always a risk taker. Daddy and I understood each other that way. I looked up to him.” I noted this sexual ambiguity and underlined it three times, but, as you’ll see later, I didn’t specifically include it in the repertorization because it was unclear. Even though it was not part of the final “analysis,” it helped me to frame the essence of the case and, therefore, to select a remedy. As she unraveled her story, she often stared off into space, dissociative; it was evident that she was still in a subdued state of shock.
During the first few weeks of treatment, during which she came every week and I did NOT give her a remedy, I took her case carefully, pulling together the threads of a very fragmented tapestry. She had been in and out of treatment, suffering from acute alcoholism herself. She drank to black-out states on a daily basis while a teenager and young adult. She stopped drinking in college and went to AA, where she continued to go. She believed in God and tried to “turn her will over to Him” on a daily basis, but had a lot of trouble with this. She liked having her own hands on the wheel and didn’t have much faith that anyone would handle it better than she would.
Sober for 10 years, she was still, in her words, adventurous and passionate about life. She was very athletic and felt better (mentally/emotionally) when she stayed active or traveled. She was a hard worker, ambitious, and strived “for perfection.” She expressed a strong need to control both her own emotions and her circumstances. She tended to be fastidious both at home and with her work. Her boyfriend drove her “crazy” because he was slow to get things done as well as sloppy.
Diagnosed as clinically depressed by a local psychiatrist, she was put on 150 mg. of Welbutrin and 25 mg. of Lamictal, neither of which had helped her. In fact, she felt worse. “I feel sad in my heart, like an emptiness,” which she added she has felt as long as she could remember. She described her childhood as unhappy: “I was crying in every picture.” I encouraged her to stay on all medication until a doctor triturated her off as she got better, but noted that the medications could be making her more irritable and moody than she would have been otherwise.
She complained of chronic, causeless insomnia. She said it was steady since she’d been sober, but it had been with her off and on almost all her life. There was “no rhyme or reason to it.”
Although she didn’t realize it until it was pointed out, she bit her nails frequently during session. I asked her if she had done that before. She answered, “Always. But not usually in front of people.”
G was anxious, particularly subject to anticipatory anxiety, and was terribly fearful of not being good enough, of failing, although she was in fact an overachiever. She often wondered if she had done enough to help her father, whom she loved and looked up to, despite all the uncertainty around issues of sexual abuse. She had conflicting feelings about him and not a little suppressed anger at him for leaving the way he did. From an early age, her sense of responsibility had been over-inflated.
Because of the chaos in her household and the complexity of the adult relationships in her life, she learned “to be invisible, to not admit to any problems, to be a perfect little girl.” This was the crux of her case, as I saw it. This was the vow that she had made that kept her pathology afloat all these years, this was the promise she had made to herself as a child that made her so terribly unhappy as an adult: “I have to be perfect or something terrible will happen.”
As a result of this unconscious koan, when she was criticized or reproached, she became very emotional. She felt attacked easily and this had caused quite a bit of strife between her and her boyfriend. When there was that strife, she became even more anxious that she would be rejected. Thus the cycle, like an Ouroboros, fed upon itself.
Generals and Physicals
She described a great many chronic diseases in the family, including bipolar disorder, cancer, and suicide. She had fissures on her tongue which were sensitive but not terribly painful, and the edges on her tongue were frayed. She attached very little significance to this in early sessions. But I marked it for future reference, which, as it turns out, came in very handy.
She tended to be warm, but not overly so. She slept on her abdomen, but didn’t stick her feet out of the covers nor did she require fanning or constant supplies of fresh air. She liked being outdoors, but when she was able to get to sleep (usually by early morning), she was covered.
G reported no overwhelming food cravings, but expressed desires for salt (2x), chocolate and bread. She was very thirsty and drank in quantity. She didn’t prefer any particular beverage.
She loved being near the ocean and loved travel but she also had a great affinity for the mountains, where she hiked and skied all year round.
Most interesting to me was that there were no strong physicals in this case at all. Her birth and disease history were also markedly minimal. No childhood acutes whatsoever, but a rich family history of mental illness, suicide, chronic disease, and cancer. This picture always brings to my mind a miasmatic pathology, which has been stratified at the highest and deepest levels of her being—her spirit, her mind, and her heart (emotion) What we see in G is all too common in my practice—a person who has very few physical symptoms and a great deal of mental/emotional ones. When there are physical symptoms, most often they are of a chronic sycotic or syphilitic nature, usually appearing under the generals.
December 2009: Repertorization and Prescription
To start repertorizing a case like G’s I start with “the three-legged stool.” What are the observable facts I can sit on? What are the fundamentals of her state? Who am I looking at, as opposed to “what?”
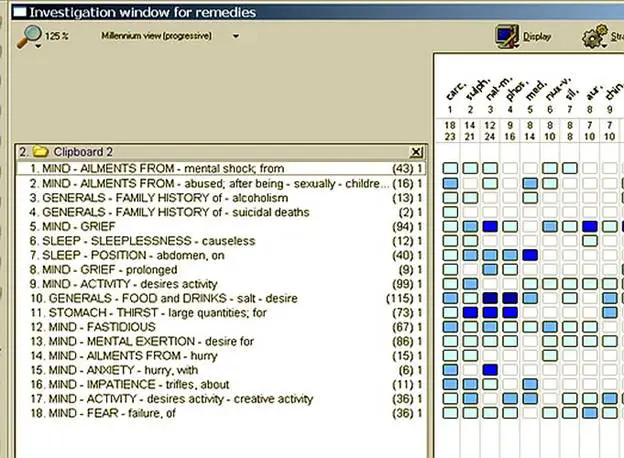
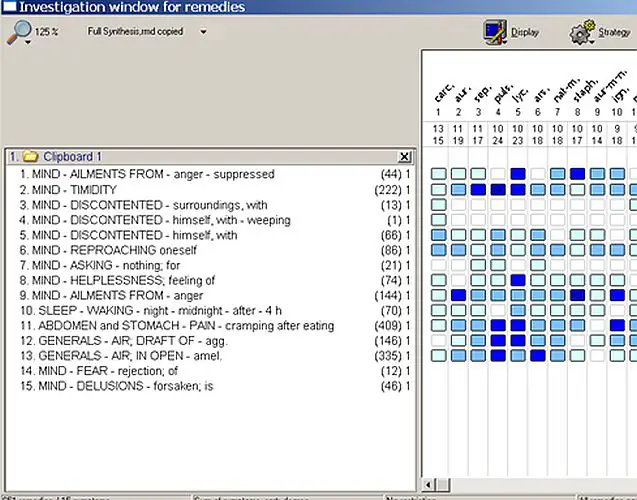
First and foremost in my approach is to see what holds up the visible pathology, which here was anxiety/fear, strife in her relationships, and insomnia. In her case (as in many others’) it was her childhood vow to herself: “To be a good little girl or something terrible will happen.” For this I chose two rubrics: 1) Too much sense of duty; and 2) Taking responsibility too seriously.
Next, as I saw it, was the utter absence of childhood illness or physical symptoms while at the same time there was a plethora of syphilitic and sycotic disease. For this I chose three rubrics: 1) Generals, personal history, absence of childhood disease; 2) Family history of alcoholism; and 3) Family history of suicidal deaths.
The third leg of the stool was her fear of failure, which was linked directly to her hypervigilance and the consuming need for control.
I included these three and the following rubrics in choosing her first remedy.
I do not always choose the first remedy on a repertorization in RADAR simply because it comes up first. I read the Materia Medica, do an extraction and get a sense of the top five or sometimes ten remedies to see which is most similar to the essence of the case.
In this instance, the rule out for Natrum Muriaticum was based primarily on her lack of retention and her amelioration from activity/movement and reassurance. While she strove for perfection, she was not nearly as inhibited as a person who generally needs Natrum Muriaticum. While a person might make a case for Sulphur in that she longed for perfection (which might be thought of as “the good opinion of others”), Sulphur wouldn’t have addressed the long-standing syphilitic line in the family or the chronic grief in the same way that Carcinosin would. And Phosphorous, even though often indicated for grief, would not have gone deep enough to address the “emptiness” and prolonged unhappiness, addiction, and anxiety. Nux Vomica did strike me as a good candidate because of her impatience, her history of alcohol abuse, and her discontent. But those qualities in her were born of a reservoir of grief and an exaggerated responsibility to other people more than the result of a position lost or an exaggerated ambition.
In my estimation, the first remedy, Carcinosin, was indisputable. It was indisputable not because she loved salt or chocolate, not because she was fastidious, not because she liked travel and was adventurous…although all those things were true, as were the other corroborating rubrics (SLEEP, position, abdomen – on) . It was indisputable because she was a sensitive, supremely diligent individual with an exaggerated sense of both her responsibility to others and her power. Her need to control and her fear of failing herself or someone else compelled her to do things unconsciously (like bite her nails or over-react to her boyfriend because she felt attacked). Furthermore, her family history made Carcinosin the most likely candidate. I believed that we needed a nosode to reach back far enough to help her.
One of my teachers, David Kramer, once described Carcinosin as the indicated remedy when there is a lack of “center.” This was G. All of her was spinning, like a centrifuge, on the periphery of her own life. In the heart of her was an empty feeling, a grief and unhappiness buried so deep, she had forgotten it was there.
Potency and dosing
After several weeks of interviewing, G was started on Carcinosin LM1, 7 succussions, once a day to start. I chose the LM potencies in moderate dosing for a number of reasons: 1) Even though she presented a front of high-spiritedness and strength, she was in fact emotionally fragile; 2) She had never used homeopathy before and, with such a highly concentrated reservoir of fear, shock, and grief, I didn’t want to create a healing crisis for her that would send her reeling. Where there is no need for roundhouse punches, I keep it simple; 3) She was taking a couple of psychotropic drugs and I believed that the repetition in gentle measure would be more useful and allow for their gradual trituration and final elimination.
The way I see LM’s is the way I see a misty, light rain on the soil as opposed to a gully washer. Sometimes a hard rain must fall. Sometimes, however, it doesn’t. This was one of those times that a gentle administration went a long way.
December 2009 to Fall 2010: Progress and Cure
G stayed on Carcinosin, working her way up the LM scale over the course of many months. We started to see progress within a week, particularly in her energy level and overall mood. After two weeks, she was taken off the Lamictal by her doctor, which resulted in a mild discomfort for a day or two. We used scaling questions (1 – 10, where 10 is the best she’s ever been and 1 is the worst) to monitor progress. She said that she felt she had been at a 3 or 4 when she walked in the office for the first time and after a few weeks of the Carcinosin felt she was closer to a 7. She stated she was able to formulate thoughts more clearly and speak without hysteria. “I was able to set some limits at work. Before, I would’ve been afraid that they wouldn’t understand me.”
She had her first aggravation as soon as she hit LM2. She had a 3-day fever, the first she could remember having. She complained that her head was congested; she was having drug and alcohol dreams, and felt it hard to leave her bed. I explained to her the meaning of aggravations and why that sort of discharge is a blessing. Like most of my patients, she laughed, “I don’t feel blessed.” We stopped the LM2 as soon as the fever started, then moved to LM3 when she reported feeling clear and kept her there until she reached a plateau (lack of any further movement).
May 2010
By LM4 she reported her first real night’s sleep “ever.” This potency had the effect of releasing her to sleep, a marked sign of progress in my thinking for it is in deep slumber that we truly heal, that we feel safe enough to let go and convalesce. She stayed at LM4 for quite a while and produced a quantity of dream material.
August 2010
After about two or three months of weekly sessions, we went up to LM5 at which point memories starting surfacing. Prior to Carcinosin, she had no memories of her childhood except for the pictures she found in family albums, in which she was always crying, and stories her parents and siblings told her. One memory came up in which she was hiding in a closet to escape one of her father’s drunken rages. We processed this therapeutically and I explained how discharges of pathology could happen not only via fevers and colds or eruptions, but in dreams and memories, so that that which is buried may be seen, and that which is silent may be heard. How could anyone feel safe or centered if there really was a boogeyman in the closet?
September 2010
By LM 6, she was sleeping through the night every night. Her dreams continued, bringing forward valuable information.
October 2010
After she’d been on LM7 for a while, she developed an incapacitating boring headache, a hypersensitivity to light and odors, and a sense of terror. Her headache was so intense, she was unable to function. She had never had headaches like these before that she could remember. They came every day between 2 and 3 p.m. (closer to 3) and came with unbearable waves of nausea, which were aggravated by motion, light, and odor. This was a strong acute and because of its debilitating nature I decided to treat it as a layer with an intercurrent. I repertorized it simply, sticking with the headache itself, bearing in mind Boenninghausen and the beautiful notion that the pathology is expressed in every symptom, that the organism is, in essence, fractal:
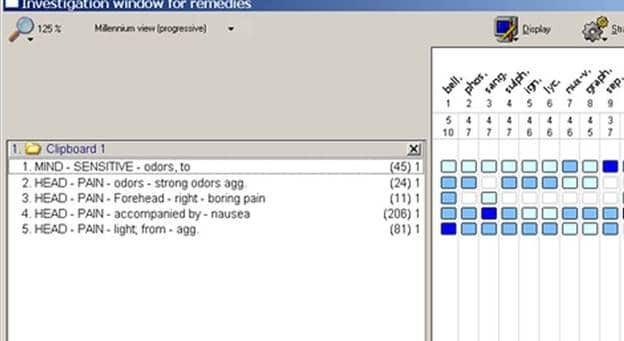
Because she’d never had these headaches before and they were not following Hering’s Law of Cure, I opted for Belladonna 30c. She felt immediately better—more calm, less fearful, and no head pain. She then erupted in pimples all over her chest and back, which was, in fact, in line with Hering’s Law of Cure. Perhaps this was what she needed when she was a child, terrified in the closet?
November 2010
After that, we waited until everything calmed down. After a couple of weeks, when the issues that brought her in returned in milder form, we brought her back to Carcinosin. She reported gains in every area as we moved through LM 7 and 8, increasing succussions to 10 and repetitions to twice a day. Within a month or two, she began trituration off the Welbutrin. She was fully off the anti-depressant in a month. Within a few more months, she announced her plans to get married.
January to March 2011
Her progress continued through LM9, 10, 11, 12. Here, even with increased succussions and repetition, her progress seemed to have reached a plateau and new symptoms started developing.
January 2011
She complained of rushing thoughts, particularly in bed, where she flopped around making mental lists of all the things she needed to do. Even though she’d had it for years and it didn’t bother her when we started our work together, she was suddenly very uncomfortable about her tongue. (This was what I had been waiting for when I noted it and put it to the side in the initial case-taking.) I asked her to stick her tongue out and it was coated white. When I asked her what made it worse/better, she stated unequivocally that she could not tolerate lemons, oranges or anything acidic.
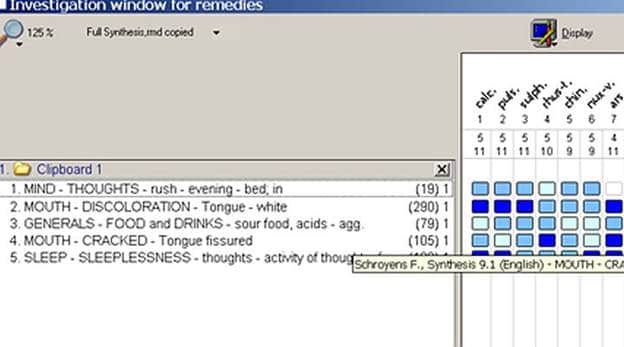
Although it repertorized out with Calcarea in the lead position, I was not satisfied with what I saw in the top five. When I went back to clarify a few things, it turned out that she was quite thirsty, but only for sipping. And even though Arsenicum Album was not covered in the rubric, MIND, THOUGHTS, rush, evening, bed; in, it was covered under restless at night, fastidiousness (lists, lists and more lists!), and was certainly covered by the sipping of water. Calcarea, in my eyes, did not fit G as a person. In both the concrete and most poetical senses, she had good bones. It was not an issue of assimilation, of “duty” in the way that Calcarea responds to it, which has always seemed to me to be more like obligation or holding onto a position in the household or the fear of being “found out”. Nor was it the Nux state of anxiety for business or position or ambition. Despite it being lower on the list, Pulsatilla suited a great deal of G’s mental state—a sense of being forsaken, fastidiousness—but the thermals were wrong.
It came down to essence: For G, it was an issue of order and safety and her need to maintain control for fear that others would drop the ball. I chose Arsenicum 30c, once a day for three days.
February 2011
This was not the first homeopathic miracle I’d ever seen, but it was one of the most memorable. For not only did the Arsenicum Album give her emotional and mental relief, but, over a relatively brief period of time (a few weeks), the actual tongue fissures started to smooth out. Within those same few weeks, her tongue looked clear (uncoated) and, more importantly, she felt mentally and emotionally clear. “I feel safe in my own skin!”
Rx: WAIT!
March 2011 through January 2012: Cure Comes Full Cycle
We waited a while. About eight months passed, during which time she took a break from therapy, got married, started a new job, and enjoyed a wonderful time with friends and family. Around the ninth month she started to present some symptoms again.
January 2012
She came in complaining of simultaneous stomach and abdominal cramps that were aggravated by eating. No particular food caused it, but she said she liked ice cream. She wasn’t clear whether the pain was actually ameliorated by it. I asked her when they started and she frowned, “I don’t know. I hate my house. I’m not so happy with my job. Things are not what I thought they’d be.” There was no clear date of etiology or causal relationship. It was a state that seemed to creep up on her.
She was upset with her new husband for not fixing up the home they lived in, but could not show it for fear, once again, of rejection. She wept that sometimes she believed he didn’t really love her, that he wasn’t as available anymore. She felt that work at her new job was “okay,” but that she should be “doing more.” I asked her if she could think of anything that might have triggered what she was feeling, and, similar to our first meeting, she explained that she’d recently been to a psychology training and it uncovered a great deal of what she termed “emotional incest” with her father. “I don’t think it was outright sexual abuse, but I was his wife. It was covert, but it was there.” She felt powerless, “out of control,” (there it was again) and was starting to have trouble sleeping, waking around 4 a.m. without cause. Her thermals and generals were similar to when I first met her with an interesting twist: She hated drafts but loved open air. No major physical complaints besides the stomach/abdomen pain.
Her discontent and suppressed frustration had spread to every corner of her life. The rubrics I chose were as follows:
And like a spiral moving upwards, there was Carcinosin again. This was not the first time I’d seen a remedy return this way, progressing with the patient into a higher realm of healing. I moved her this time to Carcinosin 1M. I chose the 1M potency because of her increased vigor and vitality. She had been in treatment by this point for about 1-1/2 – 2 years, responding beautifully to each remedy with more and more strength. As I hoped, her response was equally strong. Within days she called and laughed in between coughs, “I know you’ll tell me this is wonderful. But I’ve got snot and phlegm everywhere!”
January 2012
After the cold passed, she once again slept normally, her discontentedness was relieved, her ability to communicate with her husband and her colleagues was improved and now fruitful. She said, “I can see things more clearly. I’m not as afraid.” She no longer felt unloved or forsaken.
July 2012
It has been about six months with no return of symptoms.
For now—at least until G’s next psychology training—case cured.
www.JudithAcostaLISW.com


Hi. I would give this lady Carcinocin.
I like to read your case, it is wonderful explained, and I agree with you regarding the LM potencies, I have the same opinion. Thank you for your sharing.
That was such a well explained case, your insights into the therapeutic process are very helpful. Seeing how LM ‘s work in the real world is really beneficial for a newbie homeopath as myself. Thank you for sharing this great case. I am probably idealistic, but I do believe we are in the business of helping people turn their lives around, in a gentle yet profound way which is a huge privilege and a blessing all round. To read about this case is enormously encouraging. Thank you.