
A 79 year old female came to my clinic on 5th September 2018, with a complaint of high fever of intermittent type. When she entered the clinic, she was gasping for breath. Her daughter stated that she had been suffering from high fever since the last two days. During fever she hadthe typical malarial syndrome of chill, heat and sweat. She was also suffering from diarrhoea and vomiting. The patient remarked that she was feeling completely drained and was having great difficulty in breathing. At night she got up from her bed and sat bent forward as she was having palpitations and spasmodic bouts of cough as soon as she lay flat on her back, which was accompanied by a smothering sensation. The patient had absolutely no appetite or thirst and all she was able to take was a small cup of soup. She was slightly better off in open air and felt completely claustrophobic indoors. The daughter stated that she was extremely restless and was sitting the whole night in the drawing room, because of her breathing discomfort. In the morning she looked completely exhausted. The patient was extremely anxious and distressed and did not wish to have anyone around her.
On examining the patient, I observed a dropsical swelling of both the feet. She had bilateral wheezing on auscultation. Her pulse was extremely slow and weak. The cough was of a dry character and there was hardly any expectoration. She felt a sense of weight on her chest.
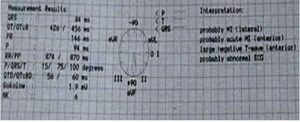
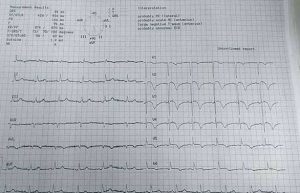
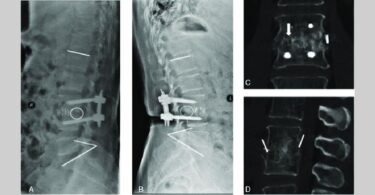
I advised the patient to undergo electrocardiography (ECG) and sent her with the medication (which I shall disclose at the end of the article). Patient underwent ECG on morning of Sept. 6th. By that time her fever was lower than before and she was in less general discomfort. In the afternoon the patient’s daughter called and said that the fever did not increase beyond 99 degrees and all other discomforts such as palpitations, restlessness, dyspnoea and chest pain were markedly reduced.
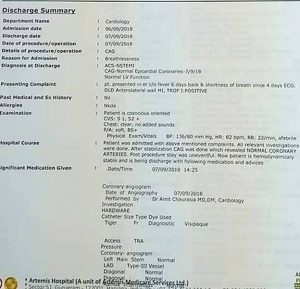
At around 8 pm (6th September), I received the ECG report. The report showed changes of Non ST elevation myocardial infarction of anterior and lateral walls of the heart. I called the daughter and insisted on getting her mother admitted to the emergency department of the nearest hospital. To my surprise the patient’s daughter said that her mother had absolutely no discomfort. However, on my advice they took her to Artemis Hospital and she was kept under observation.
On the morning of Sept 7th, the cardiologists performed a coronary angiography which revealed normal coronary arteries. Patient was conscious, oriented and even the chest examination revealed no added heart sounds. The post procedure stay was also uneventful and the patient was discharged that afternoon.
I bow to the salutary powers of Homoeopathy to help a sick individual come out of such a precarious condition without the need of interventions like CABG or coronary angioplasty, thereby,maintaining the integrity of the person as well.
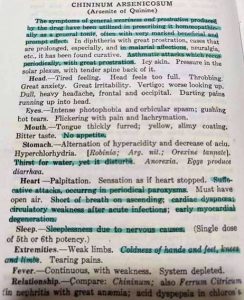
My prescription in this case was CHININUM ARSENICOSUM LM 1(one hourly). The remedy was selected based on:
WeaknessMalarial affectionsPeriodicity of respiratory complaintCardiac dyspnea – circulatory weakness after acute affections – early myocardial degeneration( Boericke)
No appetite and thirst.
The anxiety, restlessness and weakness of Arsenic album along with the periodicity and malarial affection of China.

Beautiful case!
Yes, the LM potencies can be very effective in acute situations too – something to remember.
Congratulations and thanks for sharing! 🙂