Appendicitis is a common and urgent surgical illness with variable manifestations, generous overlap with other clinical syndromes, and significant morbidity, which increases with diagnostic delay. No single sign, symptom, or diagnostic test accurately makes the diagnosis of appendiceal inflammation in all cases.
Acute Appendicitis
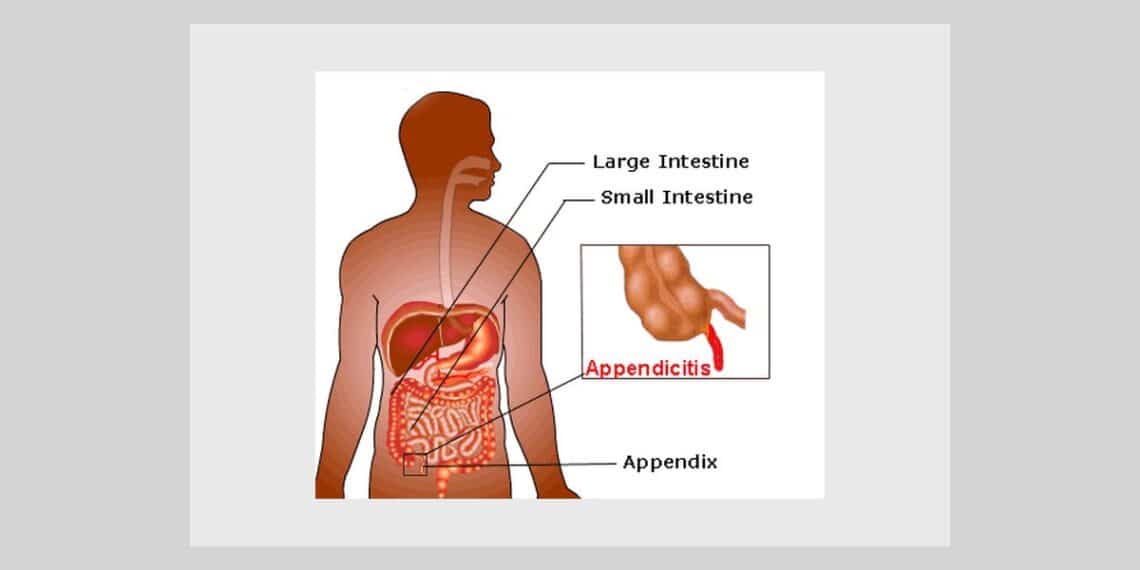
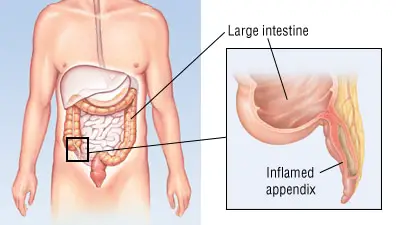
PATHOPHYSIOLOGY
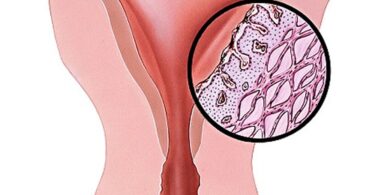
Obstruction of the appendiceal lumen is the primary cause of appendicitis (Homeopathy for Appendicitis). Obstruction of the lumen leads to distension of the appendix due to accumulated intraluminal fluid. Ineffective lymphatic and venous drainage allows bacterial invasion of the appendiceal wall and, in advanced cases, perforation and spillage of pus into the peritoneal cavity.
MORTALITY/MORBIDITY
Overall mortality rate of 0.2-0.8% is attributable to complications of the disease rather than to surgical intervention. Mortality rate rises above 20% in patients older than 70 years, primarily because of diagnostic and therapeutic delay. Perforation rates are higher in patients younger than 18 years and in patients older than 50 years, possibly because of delays in diagnosis. Appendiceal perforation is associated with an increase in morbidity and mortality rates.
SEX
Incidence of appendicitis is approximately 1.4 times greater in men than in women.
AGE
Incidence of appendicitis gradually rises from birth, peaks in the late teen years, and gradually declines in the geriatric years. Although rare, cases of neonatal and even prenatal appendicitis have been reported.
HISTORY
Variations in the position of the appendix, age of the patient, and degree of inflammation make the clinical presentation of appendicitis notoriously inconsistent. In addition, many other disorders present with symptoms similar to those of appendicitis. These include pelvic inflammatory disease (PID), tubo-ovarian abscess, endometriosis, ovarian cyst or torsion, degenerating uterine leiomyomata, diverticulitis, Crohn disease, colonic carcinoma, rectus sheath hematoma, cholecystitis, bacterial enteritis, mesenteric adenitis, and omental torsion.
The classic history of anorexia and periumbilical pain followed by nausea, right lower quadrant (RLQ) pain, and vomiting occurs in only 50% of cases.
Migration of pain from the periumbilical area to the RLQ is the most discriminating historical feature, with sensitivity and specificity of approximately 80%. When vomiting occurs, it nearly always follows the onset of pain. Vomiting that precedes pain is suggestive of intestinal obstruction, and the diagnosis of appendicitis should be reconsidered. Nausea is present in 61-92% of cases; anorexia is present in 74-78% of cases. Diarrhea or constipation is noted in as many as 18% of patients. Duration of symptoms is less than 48 hours in approximately 80% of adults but tends to be longer in the elderly and in those with perforation. Approximately 2% of patients report duration of pain in excess of 2 weeks. History of prior similar pain is reported in as many as 23% of cases.
An inflamed appendix located in proximity to the urinary bladder or ureter can give rise to irritative voiding symptoms and hematuria or pyuria. Remember that cystitis in males is rare in the absence of instrumentation. Consider the possibility of an inflamed pelvic appendix in males with apparent cystitis.
PHYSICAL EXAMINATION
RLQ (Right lower quadrant) tenderness is present in 96% of patients but is a very nonspecific finding. The most specific physical findings are rebound tenderness, pain on percussion, rigidity, and guarding.
Rovsing sign (ie, RLQ pain with palpation of the LLQ), obturator sign (ie, RLQ pain with internal rotation of the flexed right hip), and psoas sign (ie, RLQ pain with hyperextension of the right hip) are present in a minority of patients with acute appendicitis. Their absence never should be used to rule out appendiceal inflammation.
A positive cough sign (ie, sharp pain in the RLQ elicited by a voluntary cough) may be helpful in making the clinical diagnosis of localized peritonitis. Similarly, RLQ pain in response to percussion of a remote quadrant of the abdomen, or to firm percussion of the patient. The
literature is inconsistent as to whether rectal examination is helpful in making the diagnosis; however, failure to perform a rectal examination is cited frequently in successful malpractice claims.
CAUSES
Appendicitis is usually precipitated by obstruction of the appendiceal lumen. Causes of luminal obstruction include fecaliths, lymphoid follicle hyperplasia, foreign bodies (eg, shotgun pellet, intrauterine device), and tumors. Fecoliths form when calcium salts and fecal debris become layered around a nidus of inspissated fecal material located within the appendix.
Lymphoid hyperplasia is associated with a variety of inflammatory and infectious disorders including Crohn disease, gastroenteritis, amebiasis, respiratory infections, measles, and mononucleosis.
DIFFERENTIALS
- Cholecystitis and Biliary Colic
- Constipation
- Diverticular Disease
- Endometriosis
- Gastroenteritis
- Inflammatory Bowel Disease
- Mesenteric Ischemia
- Ovarian Cysts
- Ovarian Torsion
- Pediatrics, Intussusception
- Pelvic Inflammatory Disease
- Spider Envenomations, Widow
LAB STUDIES
- Complete blood count
- C-reactive protein test
- Computed tomography
- Ultrasonography
- Abdominal radiography
- Barium enema
- Radionuclide scanning
- Clinical diagnostic scores – Diagnostic scoring is done by a finite number of clinical variables which are elicited from the patient and each is given a numerical value. The sum of these values is used to predict the likelihood of acute appendicitis.
The best known of these is the MANTRELS score, which tabulates presence or absence of migration of pain, anorexia, nausea/vomiting, tenderness in the RLQ, rebound tenderness, elevated temperature, leukocytosis, and shift to the left.
- Computer-aided diagnosis – A retrospective database of clinical features of patients with appendicitis and other causes of abdominal pain is entered into a computer. It is then utilized in prospectively assessing the risk of appendicitis. Computer-aided diagnosis can achieve sensitivity greater than 90% while reducing rates of perforation and negative laparotomy by as much as 50%.
TREATMENT of Acute Appendicitis
It includes the following-
EMERGENCY DEPARTMENT CARE
Treatment guidelines for patients with suspected acute appendicitis include the following -Aggressive crystalloid therapy to patients with clinical signs of dehydration or septicemia. Restriction of anything by mouth to patients with suspected appendicitis. Consideration of ectopic pregnancy in women of childbearing age and obtain a qualitative beta-hCG in all cases.
Homeopathic Remedies for Acute Appendicitis
The goals of therapy are to eradicate the infection and prevent complications.
Belladonna
TYLER- Medicine acute intest. conditions, colic – Abdominal pains, violent; come and disappear suddenly – squeezing; clawing; as if griped by nails; violent pinchings. “Violent colic, intense cramping pain, face red as fire.” Tenderness of abdomen, worst least jar. Frequent urging to stool, little or no result (Nux). Spasmodic contraction of sphincter ani. Great pain in ileo-caecal region: cannot bear slightest touch, even of bedclothes (early appendicitis. Local external applications to abort). Typical Belladonna has red, hot face; big pupils: is sensitive to pressure draughts, jar.
TYLER – Special remedies of appendix and caecum – Years ago, when making diagrams to show the action of remedies on parts of the body, one grasped the fact that two drugs seemed to share the honours in this area- Belladonna and Mercurius corrosivus. And one knows that Belladonna has earned a great reputation for early, simple inflammation of appendix. Among its symtoms are : Great pain in right ileo-caecal region. Cannot bear the slightest touch, not even of bed covers. Tenderness aggravated by least jar.(KENT says, “The jar of the bed will often reveal to you the remedy”). Belladonna has much swelling. Its inflammations throb, feel bursting. Kent also says, “There are instances where Belladonna is the remedy of all remedies in appendicitis”.
Mercurius corrosivus
TYLER – Medicine acute intest. conditions, colic. -Peculiar bruised sensation about caecum and along transverse colon. Tender to pressure. Appendicitis. (Bell). Painful bloody discharges (from rectum) with vomiting. Tenesmus, persistent, incessant, with insupportable cutting, colicky pains. Diarrhoea dysentery with terrible straining before, with, and after stool. Mercurius cor. is almost specific for dysentery. Very distressing tenesmus, getting worse and worse: nothing blood.
TYLER – Special remedies of appendix and caecum –Kent has this drug down in black type for appendicitis. Mercurius corr. is violent and active. Has far more activity, excitement and burning. Caecal region and transverse colon painful. Bloated abdomen. Characteristic: Great tenesmus of rectum, the “never-get-done” remedy. Abdomen bruised, bloated, tender to least touch. Tenesmus of bladder, also. Hot urine passed drop by drop.
TYLER – Special remedies of appendix and caecum – Appendicitis : peritonitis. Must keep very still; stools hard, dry, as if burnt. Pain in a limited spot : dull, throbbing or sticking. Bryonia is better lying on painful side, from pressure and to limit movement. Lies knees drawn up. Better for heat to inflamed part.
Echinacea purpurea
TYLER – Special remedies of appendix and caecum – (In Repertory for Appendicitis). Boericke says : “It acts on appendix and has been used for appendicitis. But remember, it promotes suppuration, and a neglected appendix with pus formation would probably rupture sooner under its use”. –
BOERICKE – Lymphatic inflammation; crushing injuries. Compare : Iris florentina-Orris-root-(delirium, convulsions, and paralysis); Iris factissima (headache and hernia); Iris germanica-Blue Garden Iris-(dropsy and freckles); Iris tenax -1.minor-(dry mouth; deathly sensation at point of stomach, pain in ileo-caecal region; appendicitis. Pain from adhesions after).
CLARKE -Echinacea angustifolia – Clinical – Appendicitis.
Natrium sulphuricum
BORLAND – Digestive drugs – Apparently, it is a retro-cecal appendix, because they always complain of extreme pain going right round to the back, rather than of pain of McBurney’s Point. It is the type of appendix which is associated with a degree of jaundice. Some of the most striking results from Natrum sulph. have been in cases of appendix abscesses, where there has been a retro-cecal appendix and a tendency for the inflammation to track up and conditions suggesting a sub-phrenic. There is one other rather interesting point about this remedy, and it has no connection with the digestive system. Natrum sulph. is sometimes very well indicated in acute hip joints, particularly when it is the right hip which is affected. The pain is very similar in character to that experienced in cases of appendicitis, and if there are any Natrum sulph. indications, it is worthwhile to consider its use. Two cases in hospital cleared up remarkably well on Natrum sulph., and it is apt to be forgotten for this condition.
KENT – Natrium sulphuricum – It has cured many cases resembling the first stage of appendicitis. Pain and tenderness in the whole abdomen. Flatulence; colic; rending, tearing, cutting pains throughout the abdomen; stitching pains in the abdomen; violent neuralgic pains in the abdomen; inflammation of the bowels, of the peritoneum; appendicitis.
KENT – Do not forget the symptoms of Arnica in appendicitis if you know Bryonia, Rhus tox., Belladonna, Arnica and similar remedies. The homoeopathic remedy will cure these cases, and, if you know it, you need never run after the surgeon in appendicitis except in recurrent attacks. If you do not know your remedies, you will succumb to the prevailing notion that it is necessary to open the abdomen and remove the appendix. It is only deplorable ignorance that causes appendicitis to be surrendered to the knife.
“Great pain in the ileo-caecal region; cannot bear the slightest touch, even the bed clothes.”
Alfalfa
BOERICKE- Abdomen – Flatulence with distention. Shifting, flatulent pain along colon several hours after meals. Frequent, loose, yellow, painful stools, with burning of flatulence. Chronic appendicitis.
Cascara sagrada
BOERICKE – Relationship – Compare : Hyd.; Nux.; Rhamnus Californica (tincture for constipation; tympanites and appendicitis and especially rheumatism). Acts on vermiform appendix. Thus has been used for appendicitis, but remember it promotes suppuration and a neglected appendicitis with pus formation would probably rupture sooner under its use.
Ammoniacum gummi
CLARKE -clinical- Appendicitis. Stitches in the caecum at 7 p.m., alternating with pains elsewhere. This should make it appropriate in some cases of appendicitis. As an external application in the form of compresses, Lime-water has an ancient repute in allaying inflammation of many kinds.
Calcarea caustica
CLARKE –Characteristics – It has rapidly dispelled all inflammatory action in cases of appendicitis; and has removed all suffering in an aggravated case of phagedaenic piles.
Lachesis mutus
CLARKE – – Clinical – Appendicitis. Acute pain in liver extending towards stomach,” though contrary to the general “left to right” direction, is characteristic, as I can testify. Lachesis is also one of the most prominent remedies in appendicitis.
Scrophularia marylandica
CLARKE – Clinical. – Appendicitis. Breast, tumours of. Colic. Colic just below navel and some griping in the side in afternoon. Griping below navel, 7 a.m. (after a slight vexation). Pain in sigmoid flexure. Dull, heavy, periodic pain < when abdomen compressed, legs extended. (Appendicitis as a local remedy. – R. T. C.). Several stools daily with tenesmus. Albuminuria.
Tuberculinum bovinum kent
CLARKE – Clinical. – Appendicitis. “Sensitive to music” was observed in one of Nebel’s patients; another had pains in the region of the appendix vermiformis, which should lead to serviceable action in appendicitis cases.
Phosphorus
KENT – Yellow, brown spots on the abdomen; petechiae over the abdomen during typhoid fever. Pale face in pleura/peritoneum-disease, red face in articular affections.
REFERENCES
- All-in-One Care Planning Resource- 2008, by Pamela Swearingen
- Atlas of Gastrointestinal Imaging: Radiologic-Endoscopic Correlation- 2007, by Perry Pickhardt
- Clinical Companion for Wong’s Essentials of Pediatric Nursing- 2009, by Marilyn Hockenberry
- Clinical Companion to Medical Surgical Nursing – CD-ROM PDA Software- 2007, by Sharon Lewis
- Cost Effective Diagnostic Imaging- 2006, by Zachary Grossman
- Crash Course: Foundation Doctor’s Guide to Medicine and Surgery- 2008, by Daniel Horton-Szar
- EH
- Emergency Medicine- 2008, by Erik Barton
- Encyclopedia of Gastroenterology, 2004, by Leonard Johnson
- Essentials of Surgery- Nelson Textbook of Pediatrics- 2007, by Robert Kliegman
- Ferri’s Color Atlas and Text of Clinical Medicine- 2009, by Fred Ferri
- Goldman Cecil Medicine- 2008, by Lee Goldman
- Hematology and Oncology Pearls- 2005, by Michael Danso
- Manual of Medical-Surgical Nursing- 2011, by Frances Monahan
- Medical Communication Skills and Law Made Easy- 2009, by Tsong Kwong
- Medical Imaging of Normal and Pathologic Anatomy- 2011, by Joel Vilensky
- Mosby’s Handbook of Patient Teaching- 2006, by Mary Canobbio
- Mosby’s Nursing Video Skills: Physical Examination and Health Assessment- 2012, by . Mosby
- Mosby’s Pediatric Nursing Reference- 2008, by Cecily Betz
- Nelson Textbook of Pediatrics e-dition- 2007, by Robert Kliegman
- Netter’s Illustrated Human Pathology- 2005, by Maximilian Buja
- Pediatric Emergency Medicine- 2008, by Jill Baren
- Pediatric Surgery- 2006, by Jay Grosfeld
- Practical Guide to the Care of the Medical Patient- 2011, by Fred Ferri
- RADAR 10
- The Extra Step, Physician-Based Coding Practice, 2010 Edition- 2010, by Carol Buck
- The Family Medicine Handbook- 2006
- The Physician Assistant Medical Handbook- 2004, by James Labus
- Ulrich & Canale’s Nursing Care Planning Guides- 2011, by Nancy Haugen
- Year Book of Emergency Medicine- 2009, by Richard Hamilton
© Dr. Rajneesh Kumar Sharma