Definition
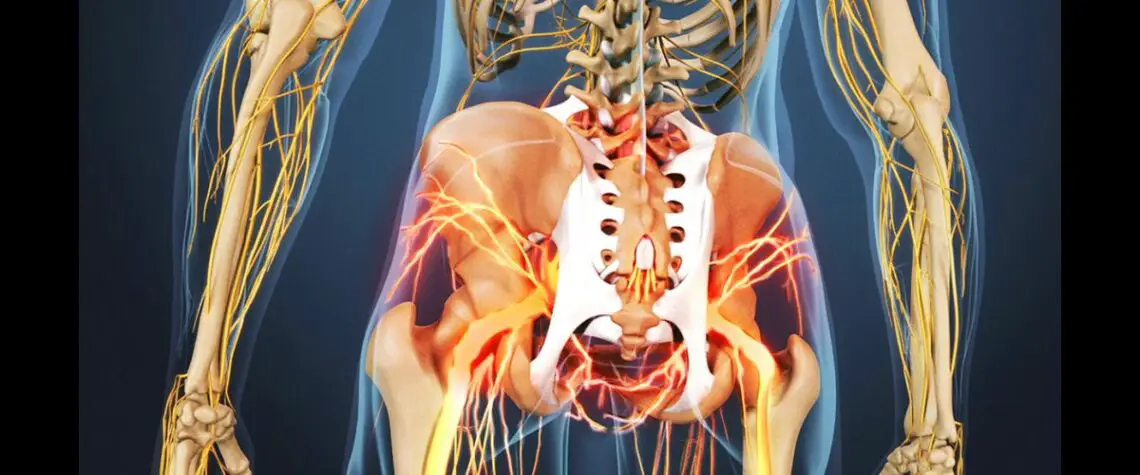
Ankylosing spondylitis (AS) is a chronic (Miasmatic), progressive (Miasmatic), painful inflammatory rheumatic disease (Pseudopsora), which affects the spinal joints, in particular the sacroiliac joints and the lumbar spine.
The disease typically begins in adolescence and young adulthood, and only rarely does it begin after the age of 45 years. Male to female ratio is 3:2.
As the disease advances, AS can result in gradually progressive stiffness (Pseudopsora/ Sycosis) and limitations of spinal mobility and also restricted expansion of the chest. In some people AS can affect other joints besides the spine, in particular the hip and shoulder joints.
Historical Background
Origin of the word
Greek – ankylos, meaning bent
It has now come to imply something that restricts motion due to stiffening and may ultimately result in fusion. When the joint loses its mobility and becomes stiff it is said to be ankylosed.
Greek – spondylos, meaning vertebra; – itis, meaning inflammation
Spondylitis means inflammation of the spinal vertebrae. The name therefore suggests that AS is an inflammatory disease of the spine that can lead to stiffening of the back.
Ancient History
The first definite description of AS can be credited to an Irish physician, Bernard Conner (1666–1698) who discovered an ancient sufferer the famous Egyptian Pharaoh Ramses II by examining his excavated skeleton.
The first clinical descriptions of the disease is from the late nineteenth century, and the medical interest in AS was stimulated by a series of publications in the 1890s by Vladimir von Bechterew (1857–1927) in St Petersburg, Russia.
Terminology
- Spondylitis ankylosans
- Spondylarthritis ankylopoetica
- Morbus Bechterew (Bechterew’s disease)
- Morbus Strümpell–Marie–Bechterew
- Marie–Strümpell’s spondylitis
- Poker back
- AS
- Bechterew disease
- Bechterew Syndrome
- Marie-Strumpell arthritis
- Marie Strumpell Disease
- Marie-Strumpell Spondylitis
- Von Bechterew-Strumpell Syndrome
Family History
AS does tend to run in families, and studies indicate that there is a genetic predisposition to it. This was clearly established in 1973, when researchers found a remarkable association of AS with a genetic marker called HLA-B27 (Human Lymphocytic antigen).
The early Symptoms
Spinal features
Early physical signs include failure to demolish the lumbar lordosis on forward flexion (Psora), pain on sacroiliac compression (Psora), and restriction of movements of the lumbar spine in all directions (Pseudopsora/ Sycosis).
Symptoms are most marked in the early morning and after inactivity and are relieved by movement (Psora). As the spine becomes progressively ankylosed (Pseudopsora/ Sycosis), spinal rigidity (Sycosis) and secondary osteoporosis predispose to spinal fracture (Syphilis), presenting as acute, severe, well localised pain (Psora). Secondary spinal cord compression is a rare complication (Psora).
The characteristic symptom of AS is sacroiliitis (Pseudopsora), the inflammation of the sacroiliac joints. The pain caused by sacroiliitis is usually a dull diffuse ache (Pseudopsora), not localized, felt deep in the buttock area. In starting, it may be intermittent or on one side only (Psora), or alternate between sides (Psora); however, within a few months it generally becomes persistent and is felt on both sides (Pseudopsora/ Sycosis).

Bilateral sacroiliitis. Frontal radiograph shows bilateral sacroiliac joint erosions and iliac side subchondral sclerosis
Progressively the lower back becomes stiff and painful (Psora/Pseudopsora), with the inflammation extending to the spine. With time, the back pain can gradually extends up the spine. These initial symptoms usually start in late adolescence or early adulthood.
The characteristic symptom is chronic low back pain and stiffness that have come on gradually, for no apparent reason.
Extraspinal features
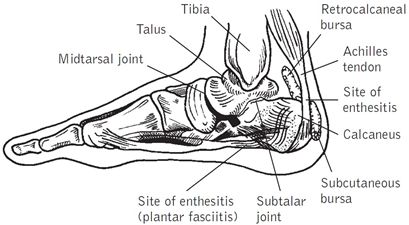
‘Pleuritic’ chest pain (Pseudopsora) aggravated by breathing results from involvement of the costovertebral joints (Pseudopsora). Plantar fasciitis (Psora/ Pseudopsora/ Sycosis), Achilles tendinitis (Psora/ Pseudopsora/ Sycosis) and tenderness over bony prominences (Psora) such as the iliac crest and greater trochanter result from inflammatory enthesopathy.
Fatigue is often a major complaint (Psora/ Pseudopsora) and may result from chronic interruption of sleep due to pain (Psora/Pseudopsora) and from chronic systemic inflammation (Pseudopsora/ Sycosis).
Extraspinal synovial joint involvement is usually asymmetrical at first and may cause inflammatory symptoms (Sycosis) mainly affecting hips, knees, ankles or shoulders. Involvement of a peripheral joint (mainly ankle, knee or elbow) precedes the development of spinal symptoms. In childhood pauciarticular juvenile idiopathic arthritis (Pseudopsora ) may develop.
Pathophysiology of AS
Enthesopathy
The inflammation in AS tends to start at the places where joint capsules, ligaments or tendons are attached to bone, resulting in pain or tenderness at these sites (Psora). The name enthesis is given to these sites, and the inflammatory lesion is called enthesitis or sometimes enthesopathy.
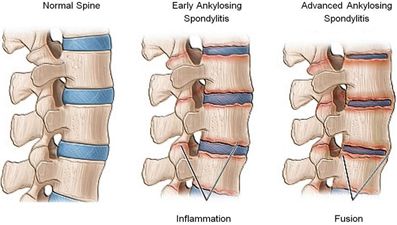
Scarring and bone formation
A process of healing and repair, which follows the enthesitis phase, results in gradual limitation of back motion due to scarring and subsequent bone formation (Psora/ Syphilis). This process may, after many years, lead ultimately to complete spinal fusion (Pseudopsora).
Sclerosis of the bones
The inflammatory changes affect the annulus fibrosus especially at its attachment to the corners of the vertebral bodies, resulting in increased bone density (Sycosis), called as sclerosis (Sycosis) of these corners. The bone at these corners may subsequently disappear (Syphilis), and this may ultimately result in squaring of the vertebral bodies (Pseudopsora).
Syndesmophyte
Gradually a thin layer of vertical bony outgrowths at the edges of the vertebrae bridges the gap (Sycosis) between the two adjacent vertebral bodies, replacing the superficial layer of the annulus fibrosus of the disc. This intervertebral bony bridging that surrounds the disc is called a syndesmophyte.

Vertebral body squaring. Lateral radiograph shows squaring of L3 and L4
vertebral bodies, L3-L4 anterior syndesmophyte, and lumbar facet joint fusion.
Spinal fusion and Bamboo spine
At the same time, inflammatory changes (Psora/ Sycosis) and slowly progressive bony fusion (Pseudopsora) may be going on in spinal joints called the apophyseal or facet joints. With severe disease, the inflammatory process of the spine may gradually, after many years, result in complete fusion (Pseudopsora) called bony ankylosis (Pseudopsora) of the whole spine. The X-ray of the spine may ultimately look like a bamboo and is sometimes called bamboo spine (Pseudopsora/ Sycosis).

Bamboo spine. Frontal radiograph shows complete fusion of the vertebral
bodies. Extensive facet joint ankylosis and posterior ligamentous
ossification produce the trolley track appearance.
Spinal osteoporosis
Spinal osteoporosis (Syphilis/ Psora) is also frequently observed among such patients, partly as a result of the lack of spinal mobility and aging.
Chest involvement
The inflammation of the costovertebral and costotransverse joints (Pseudopsora), and at the costochondral areas, can result in chest pain and tenderness. This pain can be aggravated by coughing or sneezing. Gradually chest expansion may be decreased Psora/ Pseudopsora).
Complications of AS
- Osteoporosis
- Spinal fracture
- Quadriplegia
- Spondylodiscitis
- Spontaneous subluxation of the atlantoaxial joint
- Cauda equina syndrome
- Glomerulonephritis
- Acute iritis/ uveitis
- Conjunctivitis
- Depigmentation and scarring of iris
- Cardiomegaly
- Pericarditis
- Aortic incompetence
- Mitral incompetence
- Cardiac conduction defects
- Amyloidosis
- Apical pulmonary fibrosis with cavitation
- Prostatitis
Diagnosis of AS
The generally accepted criteria for AS (modified New York criteria)
- Low back pain of at least 3 month’s duration improved by exercise and not relieved by rest
- Limitation of lumbar spinal motion in sagittal (sideways) and frontal (forward and backward) planes
- Chest expansion decreased relative to normal values for the same sex and age 4- Bilateral sacroiliitis grade 2–4 or unilateral sacroiliitis grade 3 or 4
Blood tests
ESR and CRP may be raised.
HLA B27 is frequently associated present.
Radiology
X Ray, CT scan, MRI Scan
Homoeopathic Treatment of AS
Aesculus hippocastanum
Important remedy in ankylosing spondylitis. Marked stiffness and pain over the sacroiliac joint. Worse: Rising from a seat or from stooping.
Alloxanum
BACK – ANKYLOSING spondylarthritis
Aurum metallicum
Serious or advanced rheumatism with marked stiffness. Rheumatism with stiffness or spasms of the chest wall. Severe spasm or tearing pains. Pains also described as “paralytic.”
An important remedy in ankylosing spondylitis. Wandering arthritis; moving spot to spot from one week to next. Worse: Night. Morning in bed. Hip pain worse rising from a seat or from walking. Chest wall pain and spasm worse first motion and inspiring. Better: Motion. Location: Wandering arthritis. Back. Chest and ribs. Hip.
Bacillus 7
Sensation of stiffness and ankylosis of the articulations. Shoulders painful, stiff, movements limited and difficult. Dorsal pains, aggravated by movements. Pains of all the articulations, drawing with the sensation of being drawn and rigid, aggravated when waking up after a long rest. Aponeurotic and ligamentary retraction.
Butyricum acidum
Morbus coxae senilis. Ankylosing spondylitis. Tired feeling and dull pain in small of back, worse walking. Pain in ankles and up back of leg. Pain low down in back and limbs.
Calcarea carbonica
EXTREMITIES – ANKYLOSIS
Carboneum sulphuratum
EXTREMITIES – ANKYLOSIS
Carcinosinum – BACK
ANKYLOSING spondylarthritis
Causticum
Extremities, Pain, Rheumatic, Chronic, Ankylosis, with.
Colchicum autumnale
Pain with ankylosis of the back and neck. Burning pain in the neck, ameliorated by movement. Pain in the renal region. Pain in the left scapula, aggravated on waking, by movement, and by lying on the left side. Ankylosing arthritis of the vertebral joints. Noninflammatory chronic rheumatism of the hip and knee.
Cuprum metallicum
Cramps in calves and soles. Jerking, twitching of muscles in hands and feet. Clenching of thumb in palms. Cramps in palms, calves and soles. Coldness of hands. Joints contracted. Great weariness of limbs. Ankles painfully heavy. Ankylosis of shoulder joint. Knees double up involuntary when walking, bringing him down.
Dichapetalum
Fatigue and rheumatic pains in the limbs, and legs feel like rubber. Heaviness in the calves. Stiffness at the nape of the neck , with pain starting at the 7th cervical vertebra, spreading up the nape and accompanied by right frontal hemicrania. Pain between the shoulders.
Pain in the right shoulder, spreading towards the neck. Dorsal pain and stiffness, like ankylosis. Severe pain, and stiffness in the lumbar region, when seated or when walking. Pain in the lumbar region, with drawing pains around the thighs. Drawing pains in the sacrum, ameliorated by urinating or expelling wind, worse when standing.
Eupatorium perfoliatum
EXTREMITIES – ANKYLOSIS
Ferrum metallicum
Partial immobility of the arm and slight ankylosis of the wrist.
Fluoricum acidum
EXTREMITIES – ANKYLOSIS – Fingers – Distal joint
Kalium iodatum
Weakness, emaciation. Arteriosclerosis. Cachexia. Contraction of muscles and tendons, chronic arthritis with spurious ankylosis.
Mandragora officinarum
BACK – ANKYLOSING spondylarthritis
Manganum-act. + -c.
Ankylosis spondylitis.
Medorrhinum
BACK – ANKYLOSING spondylarthritis
Mercurius solubilis
Local signs of inflammation, marked deformity, extreme atrophy of muscles, swelling of soft parts, subcutaneous nodules, fibrous or bony ankylosis. Marked deformity, extreme atrophy of muscles, swelling of soft parts, subcutaneous nodules, fibrous or bony ankylosis. Marked pain.
Oleum jecoris aselli
Ankylosing spondylitis; lumbago.
Parathyreoidinum
Fouche’ noticed that the removal of the parathyroid gland improves the condition of patients with chronic ankylosing rheumatism, but only temporarily.
Perhexilinum maleatum
Scapulo-humeral periarthritis, localized chiefly on the left. Rheumatoid polyarthritis. Ankylosing spondylitis.
Phosphorus
Paralysis of spine, especially the sacrum, from spondylitis. The chest becomes rigid or immovable. Pain, heat and burning in the spine and sciatic nerve. Sensitive, tender spinous process – especially the dorsal spine.
An important remedy in ankylosing spondylitis with rigid spine and fixed chest wall. Worse: Cold. Rising from a seat. Lying on the left side. Laughing. Crossing the legs in bed. Better: Heat. Lying on right side or on back. Rubbing. Motion.
Radium bromatum
In Europe, Ra-224 [isotope with a half-life of about three and a half days] was used for more than 40 years in the treatment of tuberculosis and ankylosing spondylitis. The treatment of children was abandoned in the 1950s, but the ability to relieve debilitating pain from ankylosing spondylitis in adults has prolonged its use.
Rhus toxicodendron
EXTREMITIES – ANKYLOSIS. Numbness and formication, after overwork and exposure. Tension as from shortening of muscles. Numbness of limbs on which he lies; esp. arms. Stiff and paralysed sensation in joints from sprains, overlifting and overstretching.
Internal coldness in limbs. As if skin around diseased parts were too tight. PA Tearing, in tendons, ligaments and fasciae. Rheumatic, spread over a large surface at nape, loins, and limbs; amel. motion [Agar.]. Soreness of condyles of bones. 5 Rheumatic gnawing, & desire to move limbs frequently, which amel..
Drawing or tearing, in limbs during rest. OB Hot, painful swelling of joints. Limbs stiff, paralysed. Paralysis; trembling after exertion. Paraplegia; after parturition; sexual excess; fevers. Lameness, stiffness and pain on first moving after rest, or on getting up in morning; amel. continued motion; but soon fatigued, requiring rest again. Cold hands and feet. Cracking of joints when stretched. Synovitis; spurious ankylosis.
Sarcolacticum acidum
Cramping pains predominantly in the back and lumbar region, aggravated when standing. At the extremities: cramp, paraesthesia, articular numbness and pains. Difficulty in brushing hair. Tiredness of the wrist when writing. Ankylosis, muscular contracture and jerking, paresis (partial paralysis) when trying to climb.
Silicea terra
Synovial cysts. Enlarged bursa over patella. Large cyst on patella; not inflamed but extremely sensitive. Chronic synovitis of knee with great swelling and ankylosis. Icy coldness of feet; or foot-sweat, often very offensive; or suppressed foot-sweat.
Sulphur
Continued use of large doses of sulphur, had caused a general emaciation with paralysis, ankylosis, contraction and deformity of the extremities.
Thiosinaminum
Are solvent, externally and internally, for dissolving scar tissue, tumors, enlarged glands; lupus, strictures, adhesions. Ectropion, opacities of cornea, cataract, ankylosis, fibroids, scleroderma.
Thuja occidentalis
Spinal Curvature-The spine from the fifth to the twelfth vertebra bent backwards, the lung dorsal muscles in the region atrophied. The patient, a boy, æt. eleven, cannot stand erect, is bent forward and supports his body by putting his hands upon his knees.
When sitting upon a chair, he supports himself by holding fast to the back of the chair; when sitting upon the floor, his head sinks down upon his knees. His hair is thin and of slow growth; the urethra is reddened; his belly is enlarged (pot-bellied) and his nose is always stopped up.
“I gave Thuja 3c. A month after this he was much better; he moves about more handily and can sit erect in a chair for a short time; the improvement continued, but the restoration of the back to the normal state took about two years.” -C. Kunkel.
Paralysis- “A woman, aged twenty-two, of feeble constitution and earthy, pale countenance came to me with stooping gait and faltering steps. Since her fourteenth year, she has had frequent vomiting and water-brash. For two months the vomiting has ceased and she now complains of her back and legs being very weak, almost paralyzed; her eyesight is very poor and she can only read a line at a time.
For some time past she has had urinary tenesmus and incontinence. Menstruation has always been irregular and is sometimes suppressed; she often has leucorrhoea. Thuja 30th first relieved the urinary symptoms, then the leucorrhoea and menstruation returned regularly.
Then the paralytic symptoms were much relieved and there developed much desquamation of the skin. In four months the patient was well, except slight anæsthesia of the legs.- Dr. Rueckert. “
Tuberculinum residuum Koch
Acts primarily on the fibrous tissues and produces fibro-chondro-osteo-mesenchymatic sclerosis! Lean weak people with grey colour of face and blue lips. Cicatrices. Dupuytren’s contraction. Chronic rheumatism with ankylosis. Periarthritis. Arthrosis. Ankylosis of the vertebral column. Tubercular rheumatism.
Viscum album
Arthrosis. Painful post-traumatic osteoporosis, linked with vaso-motor and tropho-cutaneous complaints. Dupuytren’s disease. Periarthrosis of the scapula and humerus. Arthrosis of the hip. Ankylosing spondylitis. Gonococcal rheumatism. Juvenile growth disorders.
Wiesbaden aqua
Rheumatism and gout. Abdomen full and tense. Passive or atonic gout. Contractions of muscles and tendons. Complete ankylosis. Stiffness of old fractures.
References
Ankylosing Spondylitis Clinical Neurology > Chapter 6. Disorders of Somatic Sensation > Pain
Syndromes > Back & Neck Pain > Low Back Pain
Chapter 17. Ankylosing Spondylitis and the Arthritis of Inflammatory Bowel Disease CURRENT Rheumatology Diagnosis & Treatment
7-16. The linear ossification connecting the cervical vertebral bodies in Case 7-16 (Figure 7-38)… Basic Radiology, 2e > Chapter 7. Imaging of Joints > Exercise 7-4. Arthritides
Ankylosing Spondylitis (AS) CURRENT Diagnosis & Treatment: Surgery, 13e > Chapter 40.
Orthopedic Surgery > Joints > Arthritis
Ankylosing spondylitis (AS) occurs in about 10% of IBD patients and is more common in CD than… Harrison’s Online > Chapter 295. Inflammatory Bowel Disease > Extraintestinal Manifestations > Rheumatologic
Ankylosing Spondylitis Adams and Victor’s Neurology > Chapter 44. Diseases of the Spinal Cord >
Syndrome of Subacute or Chronic Spinal Paraparesis with or Without Ataxia > Cervical Spondylosis with Myelopathy (Spondylitic Myelopathy)
Ankylosing Spondylitis Adams and Victor’s Neurology > Chapter 11. Pain in the Back, Neck, and
Extremities > Pain in the Lower Back and Limbs > Other Causes of Sciatica and Low Back Pain
Ankylosing spondylitis affects males more frequently than females, and the onset is in the… Vaughan &
Asbury’s General Ophthalmology, 18e > Chapter 16. Immunologic Diseases of the Eye > Antibody-Dependent &
Antibody-Mediated Diseases > Joint Diseases Affecting the Eye
Ankylosing Spondylitis CURRENT Diagnosis & Treatment Emergency Medicine, 7e > Chapter 21.
Arthritis & Back Pain > Emergency Treatment of Specific Conditions Causing Acute Arthritis—Monarthritis or
Oligoarthritis > Polyarthritis > Spondyloarthropathies
Ankylosing Spondylitis CURRENT Diagnosis & Treatment in Orthopedics > Chapter 5. Disorders, Diseases, & Injuries of the Spine > Inflammatory Diseases of the Spine
Ankylosing Spondylitis CURRENT Diagnosis & Treatment in Orthopedics > Chapter 7. Adult Reconstructive Surgery > Arthritis & Related Conditions > Inflammatory Arthritis
Ankylosing Spondylitis CURRENT Medical Dx & Tx > Chapter 20. Musculoskeletal & Immunologic Disorders > Seronegative Spondyloarthropathies
Ankylosing Spondylitis Harrison’s Online > Chapter 15. Back and Neck Pain > Causes of Back Pain >
Arthritis
Ankylosing Spondylitis Harrison’s Online > Chapter 325. The Spondyloarthritides
Ankylosing Spondylitis Principles of Critical Care > Chapter 94. Spine Injuries > Pitfalls in the
Assessment of Spinal Injuries
Ankylosing Spondylitis Tintinalli’s Emergency Medicine > Chapter 281. Acute Disorders of the Joints and Bursae
Ankylosing Spondylitis Tintinalli’s Emergency Medicine > Chapter 279. Emergencies in Systemic Rheumatic Diseases > Neurologic Emergencies > Spinal Cord Compression
Ankylosing Spondylitis Tintinalli’s Emergency Medicine > Chapter 276. Neck and Back Pain > Back Pain: The Thoracic and Lumbar Pain Syndromes > Differential Diagnosis and Management
Ankylosing Spondylitis Vaughan & Asbury’s General Ophthalmology, 18e > Chapter 15. Ocular Disorders Associated with Systemic Diseases > Multisystem Autoimmune Diseases
Arthritides Clinical Anesthesiology > Chapter 18. Pain Management > Selected Pain Syndromes > Low
Back Pain & Related Syndromes
Chapter 93. Ankylosing Spondylitis The Color Atlas of Family Medicine
Chronic synovitis of the spine occurs in patients with ankylosing spondylitis. Patients with… Hurst’s The Heart > Chapter 14. The History, Physical Examination, and Cardiac Auscultation > Syndromes Associated with Congenital Heart Disease > Disorders Affecting the Valves
Figure 7-45. Frontal view of the thoracolumbar spine showing the classic “bamboo”… Basic Radiology, 2e
> Chapter 7. Imaging of Joints > Exercise 7-4. Arthritides > Discussion > Connective Tissue Diseases and Seronegative Spondyloarthropathies
Key Sign Spondyloarthritis DeGowin’s Diagnostic Examination > Chapter 13. The Spine, Pelvis and Extremities > Musculoskeletal and Soft Tissue Syndromes > Axial Skeleton: Spine and Pelvis Syndromes
Low back pain that worsens with rest and improves with activity is characteristic… CURRENT Medical
Dx & Tx > Chapter 20. Musculoskeletal & Immunologic Disorders > Pain Syndromes > Low Back Pain > Clinical
Approach to Diagnosis > History of Back Pain
Prognosis CURRENT Diagnosis & Treatment: Cardiology > Chapter 33. Connective Tissue Diseases & the Heart > Ankylosing Spondylitis > Myocardial Disease, Pericardial Disease, & Bacterial Endocarditis
Psoriasis, Reiter’s disease, ankylosing spondylitis, and inflammatory bowel disease comprise the… Basic Radiology, 2e > Chapter 7. Imaging of Joints > Exercise 7-4. Arthritides > Discussion > Connective Tissue Diseases and Seronegative Spondyloarthropathies
Table 279-3 Common Features and Complications of Systemic Rheumatic Diseases Tintinalli’s Emergency Medicine > Chapter 279. Emergencies in Systemic Rheumatic Diseases > Clinical Features Table 315–1. Significant HLA Class I and Class II Associations with Disease Harrison’s Online >
Chapter 315. The Major Histocompatibility Complex > MHC Structure and Function > Association of HLA Alleles with Susceptibility to Disease
While this explanation may suffice for rheumatoid arthritis, patients with the ocular complications…
Vaughan & Asbury’s General Ophthalmology, 18e > Chapter 16. Immunologic Diseases of the Eye > Antibody-
Dependent & Antibody-Mediated Diseases > Joint Diseases Affecting the Eye > Immunologic Pathogenesis
Ankylosing spondylitis (AS) is a rheumatic disease causing arthritis of the spine and sacroiliac… Basic Radiology, 2e > Chapter 7. Imaging of Joints > Exercise 7-4. Arthritides > Discussion > Connective Tissue Diseases and Seronegative Spondyloarthropathies
Radar 10
Encyclopedia Homoeopathica




I am a huge proponent of homeopathy. We need to spread the knowledge to as many people as possible. For this reason I don’t understand why this article does not have “Send to” symbols, either on top or bottom? It would make life so easy if it did. Thank you. This is an excellent article. I have AS of my spine.
Thanks Sir
i have AS OF THE SPINE
hereditary on both sides of my family
the miasims identification a huge help
clearly seen in members of family cousins aunts uncles parents siblings