Introduction:
Migraine:
Headache is one of the most common and difficult clinical problems in medicine. In the majority of patients the cause is trivial and reversible and a careful clinical history and examination often allows a specific diagnosis there by avoiding unnecessary investigation.
Migraine is characterized by episodic headache, which is typically unilateral and often associated with vomiting and visual disturbance. The single most characteristic feature is the episodic nature of the headache.
Prevalence of migraine usually starts after puberty and continues until late middle life. Frequently women notice an aggravation of migraine symptoms during peri-menstrual phase or in patients taking oral contraceptives. Approximately half of patients who suffer from migraine have an affected relative, suggesting a genetic predisposition.
Recurrent episodes of this disease having a predisposing factors of dietary factors, including chocolate , cheese, and alcohol may precipitate attacks.
DEFINITION:
“Migraine” is a neurological diseases disease, of which the most common symptom is an intense and disabling episodic headache. Migraine headaches are usually characterized by severe pain on one or both sides of the head and are often accompanied by photophobia (hypersensitivity to light), hyperacusis (hypersensitivity to sound) and nausea.
The word ”migraine” is French in origin and comes from the Greek language |Greek ”hemi crania” (as does the Old English term ”megrim”). Literally, ”hemicrania” means “only half the head.”
SIGNS AND SYMPTOMS:
The signs and symptoms of migraine vary among patients. Therefore, what a patient experiences before, during and after an attack cannot be defined exactly. The four “signs and symptoms” below are common among patients but are not necessarily experienced by all migraine sufferers:
1. The prodrome, which occurs hours or days before the headache.
2. The aura, which immediately precedes the headache.
3. The headache phase.
4. The postdrome.
1.The first phase or prodrome:
Prodromal symptoms occur in 40% to 60% of migraineures. This phase consists of altered mood, irritability, depression or euphoria, fatigue, yawning, excessive sleepiness, craving for certain food (e.g., chocolate), and other vegetative symptoms. These symptoms usually precede the headache phase of the migraine attack by several hours or days and experience teaches the patient or observant family that the migraine attack is near.
2. The second phase or the “Aura”:
The migraine aura is comprised of focal neurological phenomena that precedes or accompany the attack. They appear gradually over 5 to 20 minutes and usually subside just before the headache begins. Symptoms of migraine aura are usually sensory in nature.
Visual aura is the most common of the neurological events. There is a disturbance of vision consisting usually of unformed flashes of white or rarely of multicolored lights (photophobia) or forma tions of dazzling zigzag lines (arranged like the battlements of a castle, hence the term fortification spectra or teichopsia). Some patients complain of blurred or shimmering or cloudy vision, as though they were looking through thick or smoked glass.
The somatosensory aura of migraine consists of digitolingual or cheiro-oral paresthesias, a feeling of pins-and-needles experienced in the hand and arm as well as in the ipsilateral nose-mouth area. Paresthesia migrates up the arm and then extend to involve the face, lips and tongue.
3. The third phase: The Headache:
The typical migraine headache is unilateral, throbbing, and moderate to severe and can be aggravated by physical activity. Not all of these features are necessary. The pain may be bilateral at the onset or start on one side and become generalized, usually alternates sides from one attack to the next. The onset is usually gradual. The pain peaks and then subsides, and usually lasts between 4 and 72 hours in adults and 1 to 48 hours in children. The frequency of attacks is extremely variable, from a few in a lifetime to several times a week, and the average migraine experiences from one to three headaches a month. The head pain varies greatly in intensity. The pain of migraine is invariably accompanied by other features. Anorexia is common, and nausea occurs in almost 90 percent of patients, while vomiting occurs in about one third of patients. Many patients experience sensory hyperexcitability manifested by photophobia, phonophobia, osmophobia and seek a dark and quiet room. Blurred vision, nasal stuffiness, diarrhea, polyuria, pallor or sweating may be noted during the headache phase. There may be localized edema of the scalp or face, scalp tenderness, prominence of a vein or artery in the temple, or stiffness and tenderness of the neck. Impairment of concentration and mood are common. Lightheadedness, rather than true vertigo and a feeling of faintness may occur. The extremities tend to be cold and moist.
4. The postdrome phase:
The patient may feel tired, “washed out”, irritable, listless and may have impaired concentration, scalp tenderness or mood changes. Some people feel unusually refreshed or euphoric after an attack, whereas others note depression and malaise.
PATHOPHYSIOLOGY:
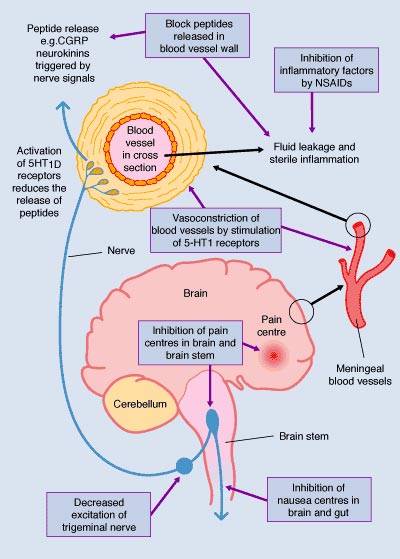
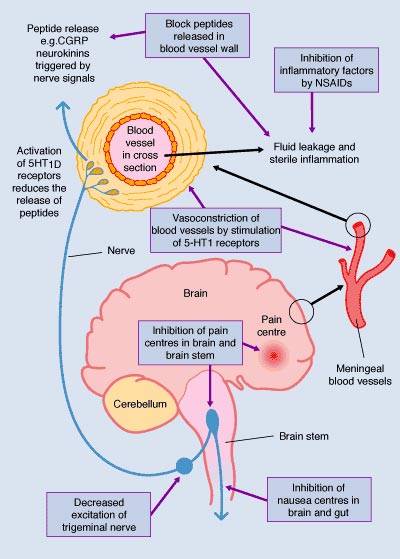
Research scientists are unclear about the precise cause of migraine headaches. There seems to be general agreement, however, that a key element is blood flow changes in the brain. People who get migraine headaches appear to have blood vessels that overreact to various triggers.
Scientists have devised one theory of migraine which explains these blood flow changes and also certain biochemical changes that may be involved in the headache process. According to this theory, the nervous system responds to a trigger such as stress by causing a spasm of the nerve-rich arteries at the base of the brain. The spasm constricts several arteries supplying blood to the brain, including the scalp artery and the carotid or neck arteries.
As these arteries constrict, the flow of blood to the brain is reduced. At the same time, blood-clotting particles called platelets clump together – a process which is believed to release the neurotransmitter – Serotonin. Serotonin acts as a powerful constrictor of arteries, further reducing the blood supply to the brain.
Reduced blood flow decreases the brain’s supply of oxygen. Neurological symptoms signaling a headache, such as distorted vision or speech may then result, similar to symptoms of stroke. Reacting to the reduced oxygen supply, certain arteries within the brain open wider to meet the brain’s energy needs. This widening or dilation spreads, finally affecting the neck and scalp arteries. The dilation of these arteries triggers the release of pain-producing substances called prostaglandins from various tissues and blood cells. Chemicals which cause inflammation and swelling, and substances which increase sensitivity to pain, are also released. The circulation of these chemicals and the dilation of the scalp arteries stimulate the pain-sensitive receptors. The result, according to this theory: a throbbing pain in the head.
More recent neuro-imaging techniques seem to show that migraine is primarily a disorder of the brain (neurological), not of the blood vessels (vascular). A spreading depolarization (electrical change) may begin 24 hours before the attack, with onset of the headache occurring at about the time of maximum brain coverage. The effects of migraine may persist for some days after the main headache has ended. Many sufferers report a sore feeling in the area where the migraine was, and some report impaired thinking for a few days after the headache has passed. In 2005, a research was made and published indicating that in some people with a patent foramen ovale (PFO), a hole between the upper chambers of the heart, migraine might result and that the occurrence of migraines might end if the hole were blocked.
MIGRAINE TRIGGERS:
Migraine is irregularly episodic, so there needs to be some explanation for why a particular migraine episode occurs at a particular time and not at another time.
A migraine trigger is any factor that on exposure or withdrawal leads to the development of an acute migraine headache. Triggers may be categorized as behavioral, environmental, infectious, dietary, chemical, or hormonal.
The trigger theory supposes that exposure to various environmental factors precipitates, or triggers, individual migraine episodes. Many people report that one or more dietary, physical, hormonal, emotional, or environmental factors precipitate their migraines. The most-often reported triggers include stress, over-illumination or glare, alcohol, foods, too much or too little sleep, and weather. Sometimes the migraine occurs with no apparent “cause.”
Migraine patients have long been advised to try to identify personal headache triggers by looking for associations between their headaches and various suspected trigger factors.
Patients are urged to keep a “headache diary” in which to note what they eat and when they get a headache, to look for correlations, and to try to avoid headache by avoiding factors they identify as triggers. Typically this advice is accompanied by a list of trigger factors.
1. Food:
Some suspected dietary trigger factors appear to genuinely promote or precipitate migraine episodes, but many other suspected dietary triggers have never been demonstrated to trigger migraines. The review authors found that alcohol, caffeine withdrawal, and missing meals are the most important dietary migraine precipitants. The authors say dehydration deserves more attention, and that some patients are sensitive to red wine. The authors found little or no
demonstrated evidence that notorious suspected triggers chocolate, cheese, or that histamine, tyramine, nitrates, or nitrites normally present in foods trigger headaches. The artificial sweetener aspartame has not been shown to trigger headache.
Dr. David Buchholz, who treats headaches as a neurologist at Johns Hopkins, has a longer list of suspected migraine triggers. Once again, he recommends eliminating the triggers from the diet altogether, and then reintroducing them slowly after many weeks to measure the effects. His list includes: Caffeine (including decaf), chocolate, monosodium glutamate, processed meats and fish (aged, canned, preserved, processed with nitrates, and some meats which contain tyramine), cheese and dairy products (the more aged, the worse), nuts, citrus and some other fruits, certain vegetables (especially onions), fresh risen yeast baked goods, dietary sources of tyramine (including the foods listed above), and “whatever gives you a headache”.
2. Weather:
Several studies have found some migraines are triggered by changes in weather. It has been noted that 62% of the subjects in the study thought that weather was a factor; in fact 51% were actually sensitive to weather changes. While those whose migraines did occur during a change in weather, often the subjects picked a weather change other than the actual weather data recorded. Most likely to trigger a migraine were, in order:
- Temperature mixed with humidity. High humidity plus high or low temperature was the biggest cause.
- Significant changes in weather
- Changes in barometric pressure
Another study says, Chinook winds (warm westerly winds occurring in Alberta, Canada) are a migraine trigger. Many patients had increased incidence of migraines immediately before and/or during the Chinook winds.
TREATMENT:
Medication that is used is quite different between attacks as compared to during an attack.
During a migraine attack non-steroidal anti-inflammatory drugs (=NSAIDs) and dihydroergotamine or sumatriptan, which stimulate serotonin receptors, are used. Drug dependency issues on narcotics have to be discussed frankly with the patient because of the danger of rebound migraines that are triggered by the continued use of narcotics. Sumatriptan can be given intranasally, but overuse and dependency on this medication also must be monitored by the physician and in males there is a higher risk for heart attacks as a side-effect of the medication. Prochlorperazine (brandname: Stemetil) can be given intravenously in the Emergency Room as a drip and can abort a migraine. Between migraine attacks there is a number of preventatives that are effective. They consist of beta-blockers such as propranolol, metoprolol, timolol and others; NSAIDs such as ASA, naproxen or ketoprofen; calcium channel blockers such as verapamil or flunarizine; antidepressants such as amitriptyline.
Gabapentin, which is used for treatment of chronic pain, has been found useful as well in the treatment of migraines as shown in several smaller studies. Gabapentin (brand name: Neurontin) releases GABA in some parts of the brain and inhibits the NMDA pain receptors.
Other medications for headache prevention are the anticonvulsant gabapentin; the MAO inhibitor phenelzine and the serotonin stimulating drugs methysergide and cyproheptatine. Unfortunately many of these medications do not work 100% and there is a lack of good randomized studies to prove effectiveness. It is important to include in the regimen of anti-migraine measures non drug regimens such as avoidance of triggering factors like certain foods (chocolate, red wine, certain cheeses and strong smells) or bright lights and noises. Consistent sleeping patterns and meal times need to be established. Counseling when emotional factors play a role, relaxation techniques like yoga, self hypnosis and biofeedback methods are all helpful as well. The more complex cases should be referred to a neurologist or even a multidisciplinary headache clinic.
Conventional treatment focuses on three areas: trigger avoidance, symptomatic control, and preventive drugs. Patients who experience migraines often find that the recommended treatments are not 100% effective at preventing migraines.
1. Trigger avoidance:
Patients can attempt to identify and avoid factors that promote or precipitate migraine episodes. Moderation in alcohol and caffeine intake, consistency in sleep habits, and regular meals may be helpful. Beyond an often pronounced placebo effect, general dietary restriction has not been demonstrated to be an effective approach to treating migraine.
2. Symptomatic control to abort attacks:
Migraine sufferers usually develop their own coping mechanisms for intractable pain. A cold or hot shower directed at the head, a wet washcloth, less often a warm bath, or resting in a dark and silent room may be as helpful as medication for many patients, but both should be used when needed. A simple treatment that has been effective for some is to place spoonfuls of ice cream on the soft palate at the back of the mouth. Hold them there with your tongue until they melt. This directs cooling to the hypothalamus, which is suspected to be involved with the migraine feedback cycle, and for some it can stop even a severe headache very quickly.
For patients who have been diagnosed with recurring migraines, doctors recommend taking painkillers to treat the attack as soon as possible. Many patients avoid taking their medications when an attack is beginning, hoping that “it will go away”. However in many cases once an attack is underway, it can become intensely painful, last for a long time (sometimes even for several days), and become somewhat resistant to medical treatment. In contrast, treating the attack at the onset can often abort it before it becomes serious, and can reduce the frequency of subsequent attacks in the near-term.
- The first line of treatment is over-the-counter abortive medication. Doctors start patients off with simple analgesics, such as paracetamol, aspirin and caffeine .They may provide some relief, although they are not effective for most sufferers. Some patients find relief from taking Benadryl or anti-nausea agents.
Narcotic pain killers (for example, codeine , morphine or other opiates ) provide variable relief, but their side effects, the possibility of causing rebound headaches or analgesic overuse headache, and the risk of addiction contraindicates their general use. - If over-the-counter medications do not work, the next step for many doctors is to prescribe a barbiturate and caffeine.
Anti-emetics may be needed in cases where vomiting dominates the symptoms. The earlier these drugs are taken in the attack, the better their effect.
Sumatriptan and related selective serotonin receptor agonists are now the therapy of choice for severe migraine attacks that cannot be controlled by other means. They are highly effective, reducing the symptoms or aborting the attack within 30 to 90 minutes in 70-80% of patients. Some patients have a recurrent migraine later in the day, and only one such recurrence in a day can be treated with a second dose of a triptan. They have few side effects if used in correct dosage and frequency.
Evidence is accumulating that these drugs are effective because they act on serotonin receptors in nerve endings as well as the blood vessels. This leads to a decrease in the release of several peptides, including CGRP and Substance P.
PREVENTIVE DRUGS:
Patients who have more than two headache days per week are usually recommended to use preventives and avoid overuse of acute pain medications.
Preventive medication has to be taken on a daily basis, usually for a few weeks, before the effectiveness can be determined. It is used only if attacks occur more often than every two weeks. Supervision by a neurologist is advisable. The effectiveness of individual medications varies widely from one patient to the next.
The most effective prescription medications include several classes of medications including beta blockers, antidepressants, and anticonvulsants.
ALTERNATIVE APPROACHES:
Because the conventional approaches to migraine prevention are not 100% effective and can have unpleasant side effects, many seek alternative treatments.
Physical therapy:
Many physicians believe that exercise for 15-20 minutes per day is helpful for reducing the frequency of migraines.
Massage therapy and physical therapy are often very effective forms of treatment to reduce the frequency and intensity of migraines. However, it is important to be treated by a well-trained therapist who understands the pathophysiology of migraines. Deep massage can ‘trigger’ a migraine attack in a person who is not used to such treatments. It is advisable to start sessions as short in duration and then work up to longer treatments.
Chiropractic adjustments to the upper cervical spine are very effective in treating migraine headaches. There is research to support these claims. One study found that the upper cervical adjustment was just as effective as drug therapy for chronic cases. It is also noted that routine spinal adjustments help prevent the frequency, duration, and intensity of the headaches.
Prism eyeglasses:
British studies have shown a relationship between the use of eyeglasses containing prism and a reduction in migraine headaches.
In that study, Dr.Turville suggests that many patients were provided with complete relief from migraine symptoms with proper eyeglass prescriptions that included prescribed prism.
Most optometrists avoid prescribing prism because, when incorrectly prescribed, it can cause headaches.
Herbal and nutritional supplements:
50 mg or 75 mg/day of butterbur (”Petasites hybridus”) rhizome extract was shown in a controlled trial to provide 50% or more reduction in the number of migraines.
Cannabis was a standard treatment for migraines from the mid-19th century until it was outlawed in the early 20th century in the USA. It has been reported to help people through an attack by relieving the nausea and dulling the head pain. There is some indication that semi-regular use may reduce the frequency of attacks.
The plant feverfew (”Tanacetum parthenium”) is a traditional herbal remedy believed to reduce the frequency of migraine attacks. Clinical trials have been carried out, and appear to confirm that the effect is genuine (though it does not completely prevent attacks).
Kudzu root (”Pueraria lobata”) has been demonstrated to help with menstrual migraine headaches and cluster headaches. While the studies on menstrual migraine assumed that kudzu acted by imitating estrogen, it has since been shown that kudzu has significant effects on the serotonin receptors.
Magnesium citrate has reduced the frequency of migraine in an experiment.
Non-drug medical treatments:
Botulin toxin has been used by some sufferers in an attempt to reduce the frequency and/or severity of migraine attacks.
Spinal Cord Stimulators are an implanted medical device sometimes used for those that suffer severe migraines several days each month.
Other alternatives:
Some migraine sufferers find relief through acupuncture which is usually used to help prevent headaches from developing. Sometimes acupuncture is used to relieve the pain of an active migraine headache.
TYPES OF MIGRAINE
1. Basilar type migraine:
”’Basilar type migraine (BTM)”’ is an uncommon type of migraine with aura that occurs in the brainstem. To meet the criteria for diagnosing BTM, aura symptoms must include at least two of the following: diplopia, simultaneous bilateral nasal and temporal visual changes, hypacusia (impaired hearing), tinnitus, dysarthria, ataxia, vertigo, simultaneous bilateral paresthesias, or unconsciousness/decreased level of consciousness.
Muscle weakness (called “motor weakness”) is not part of the aura of BTM. BTM aura symptoms are reversible, and a migraine headache occurs either during the aura or within 60 minutes. Other neurological disorders may also cause these types of symptoms, so further evaluation is generally needed. This type of migraine is also called ”’Basilar artery migraine”’, ”’Basilar migraine”’, and ”’Bickerstaff syndrome”’.
2. Familial hemiplegic migraine:
Familial hemiplegic migraine ”’FHM”’ is a type of migraine with a genetic component. These headaches typically last 1-3 days and are caused by calcium channel mutations, which occur in the pore and elsewhere. There are slightly different symptoms associated with the disorder depending on the location of the defect.
3. Acephalalgic migraine:
Acephalalgic migraine is a neurological syndrome. It is a variant of migraine in which the patient may experience aura, nausea, photophobia, hemiparesis and other migraine symptoms but does not experience headache. Acephalalgic migraine is also referred to as ”’amigrainous migraine”’, ”’ocular migraine”’, ”’optical migraine”’ or ”’scintillating scotoma”’.
Sufferers of acephalalic migraine are more likely than the general population to develop classical migraine with headache.
The prevention and treatment of acephalalgic migraine is broadly the same as for classical migraine. However, because of the absence of “headache,” diagnosis of acephalalgic migraine is apt to be significantly delayed and the risk of misdiagnosis significantly increased. Visual snow might be a form of acephalalgic migraine.
Migraine and stroke risk:
Recent studies have suggested that migraine sufferers may be at increased risk of stroke in later life. Young adult sufferers and women taking the oral contraceptive pill are at particular risk. The mechanism of any association is unclear, but chronic abnormalities of cerebral blood vessel tone may be involved.
HOMOEOPATHIC VIEW POINT:
There is a vast difference between the fundamental concept of disease evolution of the so called modern medical science (Allopathy) and Homeopathy. Homeopathy deals with the principle of individualization. It treats the man, rather than the disease.
Individualization is the integral part of Homoeopathic treatment. No two persons are alike in health or in disease. Every individual is characterized by some unique features which serve to denote that a particular individual is different from another individual belonging to the same class of group.
Dr. Hahnemann first introduced the concept of individualization in performing cures. According to him unique features that are present in a person serve to the purpose of individualization. This very approach is the basis of the homeopathic system of medicine. Individuality is the unit of nature. It is the hub around which the whole system revolves. In the drug provings, in the study of the materia medica compiled from those provings, in examination of patients, in study cases, in selection of the remedy and in conduct of whatever auxiliary treatment when required, we seek always to individualize. The question of individuality is due to the individual variation of susceptibility. The individuality is best manifested through personality reactions and in their emotional temperament, likes and dislikes. No two persons are alike in this world hence the exact character of disease varies from patient to patient while suffering from the same disease from the nosological point of view and they require individualization for their treatment. Disease individualization is not merely disease determination; it is more relevant for therapeutic purpose. Disease determination is enough for the diagnostic purpose but disease individualization is indispensable for treatment purpose. In aphorism118 of Organon, Dr. Hahnemann tells us about the individualization of the medicines. It is crystal clear that the pathogenetic power varies in each medicine hence there can be no question of substitution and the doctrine of the substitution can not be entertained at any cost. The success of a prescription resulting in cure depends on the accuracy of the person, disease and drug individualization.
THE PRINCIPLES AND PRACTICE OF HOMOEOPATHY -Richard Hughes:
HEADACHE: It is one of the glories of Homeopathy that it has brought within the range of curative treatment a multitude of minor ills hitherto thought unworthy of the practitioner’s attention. Who ever contributes to the LANCET and its fellows a case of chronic or recurrent Headache successfully treated? It is one of the most prevalent of complaints, especially in women; but it has come to be regarded as a necessary evil, and neither physicians nor patients think of it as curable. It is just the reverse with Homeopathy. Our literature abounds with cases of the cure of Headache – Dr. Peters had collected 169 in his treatise on the subject; and the relation of many of our medicines to this form of pain is accurately fixed. For full details I refer you to the “Treatise on headaches” by Dr. Peters, which I have mentioned; to the admirable papers “on Headaches” by Dr. Black in the Fifth Volume of the BRITISH JOURNAL OF HOMCEOPATHY; and to a semi-popular but really excellent sketch of the subject by Dr.Shuldham, entitled “Headaches; their Causes and Treatment.” I will myself endeavour to sketch for you the treatment of the leading forms of the malady.
TOUMIC (Syphilitic, Gouty, and Rheumatic) and SYMPATHETIC Headaches: I need not speak particularly. Their treatment must be that appropriate to the blood-poison or the disordered organ on which they depend. Nor will I deal here with Migraine. Recent understanding of this affection has given it a place among the neuroses, with which we shall consider it. The three great types which come under our present notice are the NERVOUS, the CONGESTIVE, and the “SICK” Headache.
INDIVIDUALIZATION OF DRUGS:
Homeopathy recognizes the individuality of each drug and substance in nature. Its method of testing or proving drugs upon healthy human beings is designed and used for the purpose of bringing out the individuality of each drug so that its full power and relations are established. During homeopathic drug proving the effect of a drug is closely studied on all parts of the body and in a large number of people. This gives us the full range of action of the medicine.
The crude sensations and symptoms like pain abdomen, colic, diarrhoea etc. are not much use to homeopathy and in homeopathy drug proving much finer symptoms are elicited. For e.g if a medicine produces headache during a homeopathic drug proving, then the symptom is completed with the location of pain, type of pain (throbbing, aching, burning, etc.), aggravating and ameliorating factors, concomitant symptoms, etc. The complete information allows us to differentiate various medicines producing pain abdomen in drug -proving or to say in other words the information allows us to differentiate various medicines capable of curing headache.
In aphorism 118 of Organon of Medicine, Dr. Hahnemann writes:
“Each medicine exhibits peculiar action on the human frame which is not produced in exactly the same manner by other medicinal substance of different kind.
Again in the footnote of the aphorism 119, Dr.Hahnemann writes:
Anyone who has a thorough knowledge of, and can appreciate the remarkable difference of effects on the health of man of every single substance from that of every other, will perceive that among them there can be no equivalent remedies, no surrogates.
It means there are no substitutes in the selection of a remedy. Either a medicine is indicated in a case or it is not. Symptomatic comparisons between similar drugs are carried out to find their individuality.
Manifestation of symptoms in various miasms
H.A.Roberts:
Psoric Manifestation:
Modern medicine tells us that migraine has as its underlying cause emotional disturbances. In other words, this is a verification of Hahnemann’s teaching on the disturbances roused in the psoric patient by grief, sorrow or other harrowing emotions.
Syphilitic Manifestation:
These headaches usually come on in the night and are almost always in the back of the head; they will ache all night, get better in the morning, only to come on again at night. The headaches are dull, heavy, yet lancinating; they are persistently constant at the base of the brain or on one side.
The headaches that come on Sundays or when they are away from their usual vocations are usually psoric and syphilitic combinations. Syphilitic headaches are usually < riding, > by motion, < by exertion, either mental or physical. They are usually accompanied by a great deal of coldness of the body, sadness and prostration. They are < by warmth or heat and > by cold applications; < by quiet rest, by lying down at night and by sleep, and > by nosebleed. (Note the indications for the syphilitic headache as being almost exactly opposite those of the psoric type, which are > by rest, by lying down, > by hot applications; the psoric headaches come on in the daytime while the syphilitic are manifest at night).
Sycotic Manifestation:
The headache in the vertex is sycotic in its origin; or there may be frontal headache. These are < lying down and at night, especially < after midnight. There are feverish headaches of children. This patient is restless and wants to be kept in motion, which >. The head symptoms resemble the syphilitic in that they have the night aggravations, and there is the same type of vertigo at the base of the brain.
REPERTORIAL REFERENCES FOR MIGRAINE
Rubrics related to migraine in Kent’s repertory:
Chapter – Head
Pain in head on one side :
Aconite, agar., agn., Alumina, ambr., am-c., am-m., anac., ang., ant-c., ant-t., apis, arg-m., Arg-n., arn., ars., ars-i., arund., asaf., asar., aur., bar-c., bar-m., bell., bism., bor., bov., bry., bufo., cact., cale., calc-p., camph., cann-i., cann-s., canth., caps., carb-an., carb-s., carb-v., caust., cham., chel., chin., chin-a., chin-s., cina, cinnb., clem., cocc., coff., colch., coloc., con., cop., corn., croc., crot-h., cupr., cycl., dig., dios., dros., dulc., elat., elaps, eug., euph., euphr., eup-per., ferr., ferr-ar., ferr-i., ferr-p., gels., glon., graph., guaj., hell., hyos., ign., iod., ind., ip., iris, kali-ar., kali-bi., kali-br., Kali-c., Kali-i., kali-n., Kali-p., kali-s., kalm., kreos., lac-d., lach., laet., laur., led., lyc., mag-c., mag-m., manc., mang., meny., merc., mez., mil., mosch., murx., mur-ac., nat-a., nat-c., nat-m., nat-p., nicc., nit-ac., nux-m., murx., olnd., par., petr., Ph-ac., phos., phyt., Platina, plb., psor., Pulsatilla, ran-b., ran-s., rheum, rhod., rhus-t., ruta, rob., sabad, sabin., samb., sang., Sarsaparilla, selen., seneg., sep., sil., Spigelia, spong., squil., stann., staph., stict., stram., stront., sulph., Sulph-ac., syph., tab., tarax., tarent., teucr., Thuja, ustiI., valer., verat., Verb., viol-o., viol-t., Zincum met., zing.
Pain in right side :
Alumina, arg-m., ars., asaf., Belladonna, bism., bov., bry., bufo, cact., Calcarea, carb-an., Carb-v., caust., cham., chel., cist., coca, coc-c., coff., can., croc., crot-c., crot-h., cycl., euph., ferr-ar., gels., gins., gran., graph., grat., guaj., hep., Ignatia, iod., Iris., jac., kali-c., lach., lyc., rnag-c., meny., merc., mere-i-r., mez., mil., mosch., nat-m., nit-ac., nux-m., ol-an., plat., plb., ran-b., rat., rheum, rhod., rhus-t., ruta, Sabad., sang., Sepia, sil., spong., suIph., tarax., tarent., thuj., urt-u., verat., zinc.
Pain in left side :
Aloe, alum., ambr., ars., ars-i., asaf, asar., bell., bism., bov., Bromium, bry., calad.,.calc., calc-p., cann-s., canth., carb-s., carb-v., caust., cham., chel., chin-a., chin-s., cimic., cina, coloc., can., cony., croc., crot-h., cupr., cycl., eup-pur., euph., ferr., ferr-i., fl-ac., graph., guaj., gymn., ham., hydr., ign., iod., kali-c., lac-c., lach., lac-ac., lil-t., lith., lob., lyc., mag-c., med., merc., merc-i-f., merc-i-r., murx., nat-m., nitricum acidum, Nux-m., olnd., pall., par., phel., phos., plan., plat., plb., ptel., ran-b., ran-s., rhodo., rhus-t., sabad., samb., sec., sel., Sepia, Spigelia, sulph., tab., tarax., thuj., trom.. verat-v., viol-a., viol-t., xanth., zinc., zing., ziz.
Headache from noise :
Aconite, agar., anac., anan., ang., arg-n., ars., ars-i., bapt., bar-c., bar-m., Belladonna, bor., bry., bufo, cact., calad., Calcarea, calc-s., cann-s., caps., carb-an., carb-v., caust., chin., chin-a., cic., cocc., coff., colch., con., ferr-p., gels., graph., hell., hyos., ign., iod.,.
kali-ar., kaIi-bi., kali-s., lac-c., lac-d., lach., lyc., lyss., mag-m., manc., merc., merc-i-f., mur-ac., Nat-a., nat-c., nat-p., nitricum acidum, nux-v. ph-ac., phos.; ptel., sang., sanic., sil., sol-n.,
spig., stann., stict., tab., Theridion, yue., zinc
Headache from odors :
Aconite, Anacardium, arg., aur., bell., cham., chin., coff., colch., graph., ign., lyc., nux., phos., selen., sil., sulph.
Periodic headache:
Act-sp., aloe, Alumina, ambr., ammc., anac:, apis, aran., arn., Arsenicum, ars-i., asaf., bell, benz-ac., cact., calc., calc-s., carb-v., Cedr., cham., China, chin-a., Chin-s., Coloc., cupr., eup-per., ferr., ferr-ar., ign., kali-ar., kali-bi., kreos., lac-d., lach., laur., lob., lyc., mur-ac., nat-a., nat-c., Natrum mur., nat-p., nat-s., nicc., nitricum acidum, Nux-v., phos., plat., prun., rhus-t., Sanguinaria, sel., Sepia, Silicea, spig., stram., sulph., tab., zinc.
Paroxysmal pains :
Aconite, agar., ambr., ant-t., arn., ars., asaf., Belladonna, bufo, calc., carb-v., cedr., cham., chin., chin-a., cocc., colch., coloc., crot-t., cupr., dig., ferr., ferr-ar., ferr-p., ign., kali-ar., kali-c., kali-n., kali-p., Lachesis, lyc., mag-p., mosch., mur-ac., murx., nat-a., nat-c., nat-p., nicc., nit-ac., nux-m., petr., ph-ac., plat., psor., ran-b., Sanguinaria, sars., sep., sil., spig., spong., squil., stann., stram., stront., thuj., valer., verat., viol -t., zinc
Headache from light :
Aconite, agar., anan., ant-t., arg-n., arn., ars., Belladonna, bor., bry., bufo., cact., Calcarea, chin., cocc., coff., euphr., ferr-p., gels., ign., kali -bi., kali-p., lac-c., lac-d., lyc., nat-a., nat-c., nat-m., nat-p., nux-v., ph-ac., phos., Podophyllum, sang., sanic., sep., sil., sol -n., stict., stram., sulph., tab., tarent., ziz.
Headache > by lying in a dark room:
Aconite, Belladonna, Bromium, bry., lac-d., podo., sang., sep, sil.
Headache > by darkness:
Aconite, arn., bell., brom.,chin., hipp., lac-d., mag-p., mez., sang., sep., sil., stram., zinc.
Headache with blindness:
Asarum europaeum, aster., bell., caust., Cyclamen, ferr-p., gels., Iris., lac-d., Lil-t., nat-m petr., Phosphorus, psor., sil., stra., sulph.
Headache with vomiting :
Arg-n., asar., calc., cycl., gels., glon., kali-bi., lach., lac-d., manc., op., raph., sang., sep., sil., stann., sul-ac., tab.
Rubrics Related to Migraine in Boenninghausan’s Therapeutic Pocket Book.
Chapter – Head.
One-sided in General:
Aconite, AGAR., Agn., ALUM., Ambr., Am. carb., Ammonium muriaticum, ANAC., Ant. cr., Antim tart., ARG., Arnica, Arsenicum, ASAF., Asarum europaeum, Aurum, BAR. C., Belladonna, Bism., Borax, Bovista, Bryonia, CALC. C., Camph., Cannab. s., CANTH., Caps., Carbo animalis, Carb V., Causticum, Ced., Chamomilla, Chelidonium, China, Cicuta; CINA, Clem., Cocc., Coffea, Colchicum, Coloc., Conium, Croc., Cuprum, Cyclamen; Digitalis, Drosera DULC… Euphorb., Euphr., Ferrum, Graphites, GUAI., Helleborus, Hepar, Hyoscyamus, Ignatia, lod., K. CARB., K. nit., Lachesis, Laur., Ledum, Lycopodium, Magnesia carb., Magnesia muriatica, .MAN.G., Mar., Meny., Mercurius, Mez., Mos., MUR. AC., Natrum carb., Natrum mur., Acid nitricum, Nux moschata, Nux V., OLEAND., PAR., Petrol., PHOS., PHO. AC., PLAT., plb., Ranunculus bulbosus, Ranunculus S., Rheum, Rhodo., Rhus, Ruta, SABA., SABI., Sambucus, SARS., Sele., Seneg., Sepia, Sil, SPIG., Spo., Squ., Stannum, SuI., SUL. AC., Tar., Thuja, Valer., Veratrum a., VERB., Vio. o., Vio. t., Zing.
Left Side:
Aconite, Agaricus, Alumina, Amnc., Anacardium, Ant. cr., ANAC., Aurum, Belladonna, Baryta, Bromium, BRY., CALC. C., CANTH., Caps.,CARB. AN., Carbo V., Causticum, Chamomilla, Chelidonium, CHIN., CLEM., Cocc., Coloc., DIG., DULC., Euphorb., GRAPH., Hepar, lod., K. carb., K. nit,. Laur., Lycopodium, Mag. C., Magnesia muriatica, Mang., Meny., MERC., Mercurius c., Millef., Acid Muriaticum, Natrum carb., NAT. M., Acid nitricum, Oleand., Onos., Petrol., Pho. ac., Platina, Rhodo., Rhus, RUTA, Seneg., Sepia, Silicea, spig., Staphysagria, Stro., SUL., Tar., THUJ., Verb., Vio. t., Zincum met.
Right Side:
AGAR., Agn., Alumina, Ambr., Am. carb., Ammonium muriaticum, ANAC., Aurum, Belladonna, Baryta, Bromium, BRY., CALC. C., CANTH., Caps., Carbo animalis, Carbo V., Causticum, CHEL., China, Clem., Coloc., CON., Digitalis, DROS., Graphites, Guai., Hepar, lod., K. CARB., K. nit., Kre., Laur., Ledum, Lycopodium, Magnesia muriatica, Mang., MENY., Merc:, Mez., Acid Muriaticum, Natrum carb., Natrum mur., NIT. AC., Petrol., Phosphorus, Pho. ac., Platina, Pso., PULS., Ranunculus bulbosus, Ranunculus S., Rhodo., RHUS, Sabina, SARS., SEP., SIL., Spigelia, Stannum, STAPH., Stro., Thuja, Veratrum a., Vio. t., Zincum met.
Rubric related to Migraine in Boericke’s Repertory
Chapter – Head
Migraine:
2 Marks
anac, arg.n, bell, calc, can.ind, cim, cocc, coff, gels, ign, iris, kali.c, lac.d, lach, melt, menisp, nux.v, onosm, puls, sang, scutel, sep, zinc.sul.
1 Mark
am.c, avena, bry, citr, carb.ac, indigo, kali.bich, nat.mur, plat, sil, spig, stann, sul, thea, ther, verbasc, xanth.
Periodical head pain:
2 Marks
ars, bell, ced, cinch, sang, spig.
1 Mark
acon, am.pic, arg.n, cact, gels, ign, mag.m, sep, zinc.v.
Headache associated with blindness or visual disturbances:
2 Marks
cycl, gels, iris, kali.bich, lac.d, nat.m, sang, ther.
1 Mark-
bell, ign, kali.c, lac,c, nux.v, pic.acid, pod, psor, sil, spig, zinc.s.
Headache associated with nausea:
2 Marks
ant.c, bry, cocc, ipec, iris, nux.v, puls, sang, sep, tab.
1 Mark
aloe, ars, ferr.m, gels, lac.c, naja, nat.mur, petro, sil
Headache associated with vomiting:
2 Marks
ars, bry, ipec, iris, lac.d, nux.v, sang.
1 Mark
arg.n, cham, cinch, cocc, glon, lac.c, lob, nat.m, puls, robin, sep, sil, tab,
ver,a, zinc.s
Headache aggravated by noises:
2 Marks
bell, ign, nux.v, phos.ac, sil.
1 Mark
acon, ars, coff, ferr.p, lac.d, nit.ac, phell, spig, tab.
< Bright objects: 2 Marks bell, sil 1 Mark- oreodaph, phos. ac. > Rest, Quiet:
2 Marks
bry, gels, sang, sil.
1 Mark
bell, cocc, lith.c, menyanth, nux.v, puls, spig.
Rubric related to Migraine in Murphy’s repertory:
Headache – Migraine.
Agar, Ant.c, Bry, China, Coffee, gels, Ign, Ipecac, Iris, Nux vomica, Phos, Puls, Sang, Silicea, Thuja, Zincum
Homeopathic Medicines for Migraine Headache:
1. Nat mur:
Headache comes in the morning or at 10 am lasting until 3 pm or evening. The headaches are periodical. It is preceded by partial blindness (Iris, gels, Kali bich, psorinum, silica etc.). Sensation as if there were little hammers beating in the skull similar to psorinum.
2. Belladonna:
Violent hyperemia with throbbing carotids, red face, intolerance of least noise or jar. Hemiopia, retinal blindness, slight paralysis of tongue even transitory hemiplegia.
< Afternoon or evening before or during menses > in a dark room
3. Sepia:
Migraine which had existed for years with profuse leucorrhoea has been cured with sepia. It is usually left sided and pain extends backwards. Deep stitching pain seems to be in the membranes of the brain. It is so severe that it extorts cries and frequently ends in vomiting. It is < by motion, light, noise or by thunderstorm, > sleep, rest in dark room.
It gets worse during menstrual periods.
4. Sanguinaria:
Right sided headache. Pains arise from the occiput. They increase and decrease with the course of the sun, reaching their height at midday. The paroxysms end with profuse urination (sil, gels, vera alb). They recover at every 9th day. Sanguinaria also has a menstrual headache, which attends a profuse flow in contrast to sepia, where the menses will be scanty.
5. Iris Versicolor:
When the attack begins with blurring of sight (gels, Kali bich, Nat.mur, psor, Lac.def), pains are attended with sour watery vomiting. Pains involve the infra orbital and dental nerves, with stupid stunning headache. Mostly right sided. It is a useful remedy for Sunday headache, which occurs in teachers, scholars, professors etc, in which a relief of the strain of the preceding six days; produces the headache. In sick headache with continuous nausea, it is one of our most useful remedies, and when the headaches are produced by eating sweet things, iris is probably the remedy. > from moderate motion, open air.
6. Pulsatilla:
Pulsatilla is very similar to sepia. Both are indicated by scanty menses, bursting, throbbing, boring or stitching pain on one side of the head, obscuration of sight, white tongue, nausea & vomiting. Pulsatilla has more vomiting, and thickly furred tongue with clammy mouth and relief from cold air. The pains are shifting in nature and associated with chilliness in the evening.
7. Nux Vom:
Nux vom is more suited to men than women. The attack commences early in the morning and generally increases to a frantic degree. Headache can be caused by tobacco, coffee, alcohol intake, digestive troubles, constipation and hepatic insufficiency. It suits the gouty and haemorrhoidal subjects. Headache is usually left sided, and is associated with sour taste or perhaps nausea and violent retching. The dull, wooden, busting of head following a debauch is most characteristic of Nux vomica Headache of high livers, business men. < stooping & coughing. Moving the eyes & motion in general <. A headache all over the head is also characteristic of Nux vomica 8. Arsenic alb: Causes a throbbing, stupefying headache over the left eye. The arsenicum headache is temporarily relieved by the application of cold water. 9. Theridion : Flickering before eyes, then blurring. The nausea is made worse by closing the eyes and also by noise. 10. Silica: Headache after any unwanted exertion. The pains excite nausea and fainting. The peculiarity is that there will be obscuration of vision after headache. Headache is decreased by urination. 11. Argentum nitricum: It is suited to deep seated neurotic disease and by some it is supposed to be of epileptic in nature. It is useful for periodical complaints. There is frequently boring pain in the head, which is worse in the left frontal eminence. The boring is relieved by tight bandaging. It is excited by any mental emotion or by anything that depreciates the nervous system, as loss of fluids, loss of sleep or mental strain. Sometimes the pain becomes so severe that the patient loses his consciousness. The paroxysms frequently end in vomiting of bile or sour fluid. 12. Gelsemium: Headache commencing with blindness and it is also a remedy for headache due to eyestrain (onos). Pain commences in the occiput and comes up over head and settles over eyes. (Cocculus is another remedy for occipital pain). Headache gets worse with sun – begins at 2 or 3 am and reaches its height at afternoon. It is associated with stiff neck. The patient cannot think effectively or fix his attention. Copious urination relieves the headache and the headache is accompanies with visual troubles such as double vision, squinting and dim sight. Gelsemium headaches are relieved by sleep. A characteristic of gels is a sensation of a band around the head just above the ears. It also suits “tobacco headache” > Urination ( Silica, Ign)
13. Kali bich:
The patient is affected with blindness, objects become obscured, the headache then begins. It is violent and is associated with aversion to light and noise and the sight returns as the headache grows worse. It can be compared with psorinum. In psorinum there is blindness before headache and the sight returns before the pain begins.
14. Oleum animale:
Migraine with polyuria, the urine being perfectly clear. Eyes heavy and blood shot, can hardly lift the eyelids. Speech is thick unwieldy.
15. Cocculus:
Migraine with vertigo and nausea, occipital pain is characteristic. Sick headache from riding in a carriage, boat, train or cars. Headache at each menstrual period with nausea and inclination to vomit. Headache from loss of sleep.
Juglans cinerea is one of the important remedies for occipital headache with hepatic complaints.
16. Spigelia:
Left sided sun headache. Noise and jarring of bed will aggravate the headache. Stooping and change of weather also make the pain worse.
17. Lac defloratum:
Frontal migraine in anemic women with nausea, vomiting and obstinate constipation. Hyperesthesia of sight and hearing. Icy coldness of body even near the stove. Deathly sickness of stomach. Sometimes vomiting < during menses.
18. Lac caninum:
Pain over left eye < noise and talking, > rest and cold water
Neuralgic pain in left side of head followed by a film over right eye. Intense darting. pain around left eye.
19. Melilotus:
Intense frontal headache preceded by hot flushed face, epitaxis & menstrual flow.
20. Glonoine:
Hemicrania from excessive use of wine. Nausea, dimness before eyes like a cloud followed by most violent headache > by vomiting.
21. Epiphegus:
Headaches are neurasthenic in type, brought on by strenuous exertion such as going on a visit, doing a day’s shopping etc. Vision gets a little blurred. It is worse on rising from supine position and in the open air. There is a decided relief after a sound sleep. Pressive pain in the temples traveling inwards < from working in open air. Headache is caused by mental and physical exertion and they are preceded by hunger.
22. Scutellaria:
In nervous sick headache which is caused by excitement and over exertion with frequent scanty urination. Associated with restless sleep and night terrors. Worse over right eye, aching in eye balls. Explosive headache of school teachers.
< Noise, odor, light > Night, rest
23. Tongo:
Used in migraine with neurological affections. Tearing pain in supra orbital nerve with beating and throbbing pain in head. Trembling in right upper lid. The symptoms are < by rest, when seated , > by movement & pressure.
24. Cyclamen:
Migraine is accompanied by sparkling before eyes. One sided headache. Vertigo – things turn in a circle, > in a room, < open air. Frequent sneezing and itching of ears.
25. Picric acid:
Headache from over study or over work; occipital pain. Relieved by bandaging tightly worse from slightest mental exertion.
26. Damiana:
It is an excellent remedy for migraine.
27. Chionanthus:
Migraine due to acidity and sluggishness of liver.
28. Carbolic acid:
For migraine in children – Tight feeling in head as if compressed by a rubber band headache better by green tea, while smoking.
29. Cannabis Indica:
Migraine attack preceded by unusual excitement with loquacity.
Headache with flatulence. Feels as if top of head were opening and shutting and as if calvarium were being lifted.
30. Lobelia inflata:
Periodical headache that comes on in the afternoon and continues to increase till midnight every third attack being more violent than the two previous attacks. Gastric headache with nausea, vomiting and prostration.
31. Lithium carb:
Headache of females, brought on by sudden cessation of menses, and it is always better when the patient eat something.
32. Prunus spinosa:
Right sided migraine, shooting pain from right frontal bone through brain to occiput. Pain in right eye ball as if it would burst.
33. Verbascum thapsus:
Sensation as if the temples were crushed together. Neuralgic pain in the zygoma, temporo-maxillary joint and ear, particularly left sided, with lachrymation, coryza and sensation as if parts were crushed with tongs. Talking, sneezing and change of temperature aggravate the pain also pressing teeth together. Pain seems to come in flashes, excited by least movement, occurring periodically at same hour in the morning and afternoon each day.




Thank you for the indepth study you have made. You have gone through all the School of medicine except Ayurvedic one. I think it is worth to study.
I am a migraine patient and my school life and college life has disturbed for the same. I have been treated at first by Allopathy school (Safderjung Hospital & AIIMS in Delhi) and thereafter in Homeopathy in the 60s. Now I am 52 yrs. Out of all these treatment only Dr. B C Guha, MD, LRCP&S (Homeopathy doctor of President ,S.Radhakrishnan) has cured upto 80% but unfortunately I could not continue the treatment. Thereafter i took ‘Vasogratn’if necessary.
I my self has some study and my own personal experience regarding migraine are:
1.It is psychomatic disease. So mental aspect is very important. So expression of mental tension/pressiure should be addressed. I think, control of mind in our Indian Yogic process is very much important.
2.In my case change of weather is the other important triggering factor. Change of temperature and barometric pressure.
3.Migraine patients are perfectionist – sometime that built up tension which trigger headache which turns to migraine. So I changed my life to be very casual and this helps me. You may also suggest your patients.
4.”Migraine Personality” – I think it is there. I have made studies survey in this regard. They are generally advanced thinkers and so a bit different from others. Such child should be handled cautiously and separately.
5. Migraine severely affect the carrier of a student so it should be treated urgently.
For any further please feel free to contact me.
all of your observations are correct & apply to my case.
Hi Pradeep,
I have been experiencing visual disturbance for several years not frequently (roughly about once in a few months) and today I experienced this after almost 2 years. Usually this disturbance lasts for 30 to 45 minutes. Many times I do not experience any headache at all. But sometimes I experience headache after the vision has become normal. Many years ago I consulted an ophthalmologist and he rule out any problem with vision. Is there any way I can prevent this kind of visual disturbance in future? What about homeopathy? I am looking forward to your suggestions. My email: [email protected]
Regards,
Srikanth
Very useful article.
Amazing information…..Very Nice….Keep it up…..
Good explanation. keep it up.
Good going Pranesh !!!!!
Keep it up……
dear sir,
i feel the article could have been written in beautifull way, if practical aspects, any case studies of patients ,any illustrations were given.merely writing from medical books is not difficult .further i would like to point out that these classifications are given as per allopathic school as they are having set of treatments prefixed but in homeopathy individuality needs emphasis so as to cure patient.these aspects listed above were lacking.
thanks
Very very useful article, because this is a common disease now a days.
Very useful and nice article all Migraine patent and doctors
good article
is there any treatment in homeopathy for “VISUAL SNOW”…
p.s. i do not have any headache, pain etc.. only visual snow(flickering dots, tv like static).
please help…
Hello Dr. Pranesh,
Thank you for the informative article.
I have been experiencing visual disturbance for several years not frequently (roughly about once in a few months) and today I experienced this after almost 2 years. Usually this disturbance lasts for 30 to 45 minutes. Many times I do not experience any headache at all. But sometimes I experience headache after the vision has become normal. Many years ago I consulted an ophthalmologist and he ruled out any problem with vision. Is there any way I can prevent this kind of visual disturbance in future? What about homeopathy? My email: [email protected]
Regards,
Srikanth