Reprinted with permission from the Indian Journal of Applied Homoeopathy where it first appeared. https://www.jimshomeocollege.com/ijah-publications/
INTRODUCTION
Dengue is an acute mosquito transmitted viral disease characterized by fever, headache, muscle and joint pains, rash, nausea and vomiting. Dengue fever (Homeopathy Treatment for Dengue Fever) is usually self-limited, biphasic febrile illness, its presentation may range from asymptomatic to Dengue Hemorrhagic Fever (DHF) and fatal shock (Dengue Shock Syndrome-DSS). The illness is more severe and begins more suddenly in adults, infection is asymptomatic in 80% of infants and children. In 2013 dengue was estimated to be responsible for approximately 3.2 million severe cases and 9000 deaths worldwide. In India the case fatality rate is about 3-5%.
Causative organism
It is an arbovirus from Genus –Flavivirus. It is the most common among all arbovirus infections. There are four 4 serotypes (DENV-1, 2, 3 & 4) of infections identified. Infection with one serotype does not include solid immunity to the other. Hence, individual may suffer from dengue fever more than once.
Epidemiology
Large number of cases regularly occurs in urban, suburban and rural areas, with increasing proportion of Dengue Hemorrhagic Fever and Dengue Shock Syndrome. In India during 2013, about 74168 cases were reported with 168 deaths. Case fatality rate was 0.22%. The highest numbers of cases were reported from Punjab followed by Tamilnadu, Gujarat, Kerala and Andhra Pradesh.
Transmission
Dengue is transmitted via Aedes aegypti mosquitoes. It is transmitted by female mosquitos’, bites during day time only.
Incubation period2 – 7 days
CLINICAL PRESENTATION:
– Classical Dengue
- Dengue Hemorrhagic fever
- Dengue Shock Syndrome
CLASSICAL DENGUE
- Sudden onset of chills and high fever with intense headache
- Retro-orbital pain with photophobia
- Muscle and joints pain which prevent all movements
- Intense myalgia ; BREAK BONE FEVER
- Constitutional symptoms like extreme weakness, anorexia, constipation, altered taste sensation, colicky abdominal pain, sore throat and general depression.
- Typical morbilliform rash spreading centripetally to face; trunk & limbs, spares palms & soles with first 24-48hrs. Lasting for 1-5 days, resolves with desquamation.
DENGUE HEMORRHAGIC FEVER (DHF)
- Occurs especially in children and young females
- Pre-circulating anti-dengue antibody is predominant risk factor. It may be acquired from previous infection with different serotype or in the form of trans-placental transfer.
- Leakage in plasma takes place in DHF & extravasations occur in the endothelial gaps due to increased capillary permeability.
Onset– 3rd to 7th days of illness
Criteria for diagnosis of DHF
- Fever or H/O fever lasting 2-7 days
- Hemorrhagic tendencies indicated by any of the following: Positive tourniquet test, Petechie, ecchymosis or purpura, bleeding from mucosa, gastrointestinal tract, injection sites or other locations
- Enlargement of liver
- Thrombocytopenia : platelet count < 1,00,000/mm3
- Hemo-concentration : hematocrit increased by > 20%
Plasma leakage evidenced
Rise in haematocrit> 20%
- Fall in haematocrit> 20% after IV fluids
- Positive tourniquet test i.e. appearance of more than 20 petechiae per 2.5 cm2 on inflating sphygmomanometer cuff for 5 minutes.
DENGUE SHOCK SYNDROME
All the criteria of DHF plus, Shock – manifested by rapid and weak pulse with narrowing of the pulse pressure 20 mmHg or less) or hypotension, tachycardia, with the presence of cold, clammy skin & restlessness.
Grades of Dengue…
Grade I – fever + non-specific constitutional symptoms. The only hemorrhagic manifestation is a positive tourniquet test.
Grade II – manifestations in grade I plus patient with spontaneous bleeding, usually in form of skin hemorrhage.
Grade III – circulatory failure by rapid and weak pulse, narrowing of pulse pressure or hypotension with the presence of cold clammy skin and restlessness.
Grade IV – profound shock with undetectable blood pressure and pulse.
Warning signs for shock…
- Intense, sustained abdominal pain
- Persistent vomiting
- Restless or lethargy
- Sudden change from fever to hypothermia with sweating and prostration.
INVESTIGATIONS.
Probable diagnosis
Serological tests
- NS1 Ag Rapid tests
- ELISA for IgM (for recent infection) – Appear within 5 days, persists for months 3.ELISA IgG (for Chronic infection)
Confirmed diagnosis
- Culture is positive within first 5 days (sensitivity< 50%); can also obtain culture from liver at autopsy.
- Detection of virus in tissue, serum, or CSF by IHC, IFA or ELISA
- Increased specific IgG or IgM
- WBC decreased (2,000-5,000/uL) with toxic granulation of leukocytes and neutropenia; may have marked atypical lymphocytes.
- In DHF, decreased platelets (<1,00,000/uL) with impaired aggregation, prolonged prothrombin time in severe cases of DHF. DIC may occur.
- Increased transaminase (5,00-1,000 U/L) and bilirubin indicating decreased hepatic & renal functions.
- RT-PCR: Detection of genomic sequence of virus by RT-PCR (sensitivity > 90% early, <10% in 7 days). Reverse transcriptase polymerase chain reaction (RT-PCR) sensitive and specific for detection of viral RNA. But this test is still a research tool.
COMPLICATIONS
- Bleeding
- ARDS
- Renal failure
- Hepatic failure
- Encephalopathy
Homeopathic Treatment Approach in Dengue:
CASE – 1
PRELIMINARY INFORMATION
Name- Mr. S.S Age- 32 years Sex- M Marital status- Married Occupation- Machine supervisor
Date of admission- 27/9/09
C/o Generalized body pains since 5 days – severe pain as if body would break, followed by fever. Fever paroxysm- heat all over the body but the head more hot, with insipid taste 3 and dryness of mouth3. Patient took allopathic treatment without relief but, the fever pattern changed.
Since yesterday – Mild feverishness with nausea worse eating solid food3,better by drinking2 and pain in eyes, worse opening eyes3 better closing eyes3. Insipid taste3 and dryness of mouth3 still present. Thirst – small quantity and occasionally large quantity.
Investigations as on 25-9-09 were: CBC- Hb: 14.2, WBC- 2600, N 56, L 41 E02, platelet count- 67,000, Urine routine- RBC- 2-4/hpf, Pus.Cells- 1-2/hpf
ON EXAMINATION FINDINGS-
| GC: | Fair, No pallor, icterus, edema, cyanosis, No lymphadenopathy | ||
| Eyes: | Congestion ++ | ||
| Skin: | Fine macular erythematous rash on extremities, blanching on pressure ++ | ||
| Temp: | 99.4oF, Maximum temperature recorded on the day of admission was 100.8O F | ||
| Pulse: | 74/min | ||
| BP: | 110/80 mmHg | ||
| RS: | Clear | ||
| CVS: | S1S2 heard | ||
| PA: | Soft L0S0 | ||
| INVESTIGATIONS BEFORE ADMISSION | INVESTIGATIONS ON THE DAY OF ADMISSION |
| CBC- Hb: 14.2
WBC- 2600 N56 L41 E02 platelet count- 67,000 Urine routine- RBC- 2-4/hpf P.C- 1-2/hpf
|
CBC- Hb: 15.06
WBC: 4,800 N52 L43 E02 platelet count- 1,02,000 Widal test- O-1:60 H-1:60 AH and BH- nil PS for MP- negative Malaria antigen- negative |
PROBABLE DIAGNOSIS with DIFFERNTIAL DIAGNOSES-
- Dengue fever
- Viral fever
- Malaria
Reasons for consideration of Dengue fever as the diagnosis-
- Prominence of Myalgia in the symptomatology
- Fever low grade and more or less continuous type
- Presence of a macular blanching rash
- Leucopenia, a normal or increasing hematocrit
- A continuous low platelet count
INVESTIGATION: on 28/9/09 Dengue IgM and IgG POSITIVE.
FINAL DIAGNOSIS- Dengue fever
Full homoeopathic history was taken on the day of admission and fever totality as well as the chronic Constitutional totality were erected.
FEVER TOTALITY-
- Change-in fever paroxysms of fever due to allopathic medicines
- Thirst increased fever during
- Nausea < eating after3
- Head pain < stooping3
- Dryness of mouth fever during3
- Insipid taste3
DIFFERENTIAL REMEDIES-
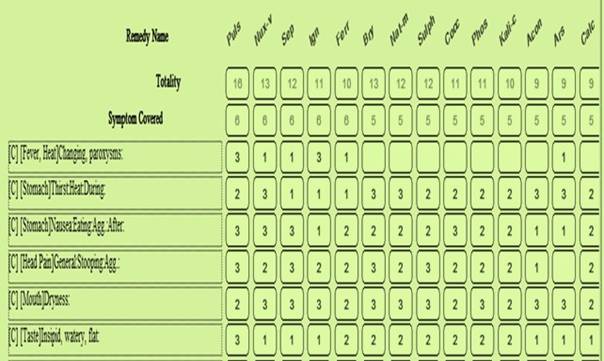
Nux Vomica, Pulsatilla and Sepia come close on Repertorization.
In Nux Vomica, chilliness is marked along with body ache, cannot bear to uncover. Patient is thirsty during chills and thirstless during fever. Low back pain is hall mark along with aching limbs during fever. NuxVom has loud, painful retching and water brash along with nausea. Gastric bilious symptoms are present during apyrexia.
Pulsatilla has slow insidious onset with subdued mild symptomatology. Thirstlessness is a hallmark of Pulsatilla along with loathing for food which is worse on eating. Taste is bad especially in the morning with white coated tongue.
Sepia is the remedy for irregular fever with changing paroxysm especially caused by medicinal intervention allopathic or homoeopathic. Sepia feels extremely chilly. Nausea not better by eating is hallmark concomitant during fevers. Sepia has thirst during chill and though thirsty during heat, less thirst compared to chilliness stage.
Sepia 200 1 dose was given on morning of 28/9/09 as the indicated remedy for the fever.
FOLLOW UPS: –
| Date | Follow up | Platelet Count | Action |
| 28/9/09 evening | No fever, Chilliness – better. Body ache, headache, nausea, eye pain – improved, Appetite and thirst improved. Sleep better. Maximum temp- 99.2F | 1,05,000 | Placebo |
| 29/9/09 | Asymptomatic ,Temp- Afebrile | 98,000 | Placebo |
| 30/9/09 | Asymptomatic, Maximum Temp- 99 F | 1,15,000 | Placebo |
| 1/10/09 | Asymptomatic, Temp- Afebrile | 1,40,000 | Placebo |
| 2/10/09 | Fine rash on abdomen and extremities, Afebrile Patient was discharged from the hospital. | 1,40,000 | Placebo |
| 5/10/09 | Rash absent, Pt was Afebrile & asymptomatic | 2,50,000 | Placebo |
DISCUSSION:-
Patient came for 5-6 days after onset of illness. He had been to a general practitioners for conventional medicine which did not completely relive him, but simply changed the pattern of fever, fortunately the concomitants persisted in spite of intervention, which, helped in forming totality.
It is important to trace the journey of patient and evolution of symptoms while treating fevers. Eliciting onset, duration and progress of each symptom is key to erecting homoeopathic totality.
Post Repertorization seemingly indicated remedies emerge like in this case,Pulsatilla, Nux Vomica, Sepia and Arsenic. Materia Medica references help understand the finer nuances of remedy differentiation.
Susceptibility assessment based on severity of illness, pace of disease and characteristic that emerge during acute episode help determine the dosage and potency. In this case patient presented with moderate intensity of illness and preserved individualistic characteristics in form of concomitants in spite of allopathic treatment received by him before switching to homoeopathy. This indicated only moderate deviation from state of health which could be restored back with single stimulation of indicated remedy.
Close follow up of the patients is essential, even though patient might report betterment in subjective symptoms.Close observation of objective criteria’s like leucopenia and platelet count is essential. In this case though patient reported no fever since second day of introduction of Sepia, patient’s platelet count was observed closely till it reached the normal range.
CASE – 2
PRELIMINARY INFORMATION
Name- Mr. D.S Age- 24 years Sex- Male Education- 4th standard
Occupation- welding machine worker, Marital status- married since 5 months
History:Patient came with complaints of fever with rigors on the 25/9/09. Along with fever complained of pain in limbs, backache and headache. There was an afebrile period for a day followed by fever with rigors again. Later on 6th day developed nausea and vomiting. Please refer to table below for details. Throughout patient showed irregular fever patterns.
| LOCATION | SENSATION | MODALITY | CONCOMITANT |
| General – Since 5 days
On first day Intermittent |
Started from pain in limbs3, later started having fever with mild chilliness. Backache 2 headache3
Fever with rigors3 Took Allopathic treatment with general practitioners. |
< movement3
> pressure2 < night3
> covering3
|
Weakness3– could not get up and go to work |
| On 2nd and 3rd day | Asymptomatic | ||
| On 4th and 5th day | Fever with rigors again Bodyache3& headache3 | < Jarring3
> pressure2
|
Thirstlessness3 during
fever Bitter taste3 |
| No fixed pattern of fever | |||
| On 6th day i.e. on the
day of reporting
Stomach
Abdomen |
Fever increased, chilliness3
Bodyache3, headache3 Nausea3 with retching & vomiting of ingesta not better after eating. Mild pain |
< Jarring3
> pressure2
|
Bitter taste3
|
ON EXAMINATION FINDINGS-
| G.C: | Fair, No pallor, icterus, edema, cyanosis, no lymphadenopathy | |||
| Tongue: | Clean, moist | |||
| Temp: | 101.4OF | |||
| Pulse: | 88/min | |||
| BP: | 120/80mmHg | |||
| RS: | Clear | |||
| CVS: | S1S2 heard | |||
| PA: | Soft, recti tender +, Liver 1 finger palpable, Spleen 1Finger Palpable | |||
| Back: | lumbar para-spinal tenderness+ ROM full | |||
| INVESTIGATIONS DONE ON 25/9/09 | INVESTIGATIONS DONE ON 26/9/09 | |||
| CBC- Hb- 13.2, TLC- 4,000, N:50 L:40 E:08 M:02
ESR- 20 Platelet count- 1,65,000 PS for MP- negative
|
CBC- Hb- 13.8, WBC- 4,000, N:55 L:38 E:05
M:02 Platelet count- 1,52,000 S. Total Bilirubin- 1.6 S. Direct Bilirubin- 1 SGOT- 77 SGPT-42.7 Widal test- negative PS for MP- negative MP antigen- Negative Urine routine- NAD DENGUE IgM- Positive DENGUE IgG- Positive
|
|||
FINAL DIAGNOSIS: Dengue fever
TOTALITY OF SYMPTOMS-
- Thirst less fever during
- < Jar3
- > pressure2
- Extremity pain fever during3
- Weakness fever during3
- Backache fever during3
- Headache fever during
- Taste bitter
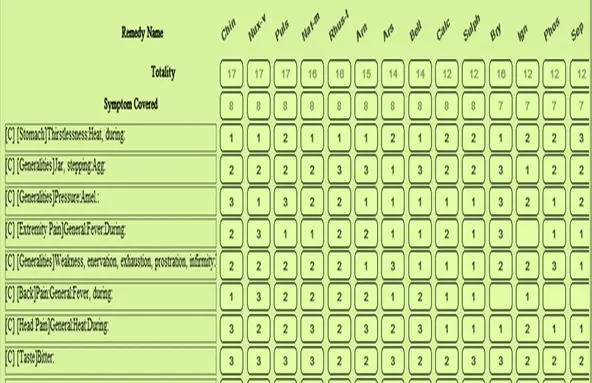
DIFFERENTIAL REMEDIES:-
| Drug | Materia Medica | ||
| China | | Prodromal : nervous excitement, anxiety, headache, nausea, irritability | |
| | Chill: Chill followed by thirst, wants to wrap himself warmly, chill begins in the breast. | ||
| | Heat: without thirst, fiery red face with congestion of head, other parts chilly | ||
| | Sweat: with thirst, drenching profuse, debilitating | ||
| | Apyrexia: debility, restlessness, anemia, edema | ||
| | Headache and weakness as concomitants. | ||
|
|
Fever patterns are clear and well defined | ||
| Nux.Vomica | | Fever with prominent gastro-bilious symptoms | |
| | Chill: preceded or accompanied by blueness of fingernails | ||
| | Chill with yawning & aching in limbs and back | ||
| | Chill not relieved by covering or external heat | ||
| | Thirst less during fever | ||
| | Low backache during heat | ||
| | Worse Pressure | ||
|
|
Weakness is not a prominent concomitant. | ||
| Nat Mur | | Useful in inveterate and badly treated cases of fever | |
| | Chill: 10 – 11 am, begins in small of back or feet | ||
| | Chill with thirst and generalized aches and pains | ||
| | Heat: high fever with throbbing headache, increased thirst, | ||
| | Fever blisters around lips | ||
| | Sweat: debilitating , relieves headache | ||
| | Marked periodicity | ||
| Sepia | | Irregular Fevers | |
| | Marked Chilliness | ||
| |
Worse Jarring |
||
| | Better Pressure | ||
| | Profound Prostration | ||
| | Nausea at smell and sight of food | ||
| | Nausea not better by eating | ||
| | Thirst less during fever | ||
Treatment:
SEPIA 200 1 DOSE WAS GIVEN ON 26/9/09
If one refers to reportorial sheet all remedies seem closely indicated. Except for natrum all other remedies considered are thirstless during heat. Nux has worse jarring but has worse pressure too, which is opposite of what patient presents. Natrum mur and China have well defined patterns of fever with regular paroxysms. Nux , China and Natrum have significant headaches but, with differing modalities.
Sepia covers generals of irregular pattern of fever, general modalities, and general sensation of weakness, thirstlessness and modalities of nausea. Hence, qualitatively sepia has better coverage of the case.
FOLLOW UPS:-
| Date | Follow up | Platelet Count&
Ix |
Action |
| 26/9/09
|
Fever & chilliness-better, Appetite SQ, thirst -improving, General sense of wellbeing present Max Temp- 102.8OF | 1,52,000 | Placebo |
| 27/9/09 | Most of the complaints SQ in the morning but better by the evening. Max Temp- 98.6OF | Not done | Placebo |
| 28/9/09 | Itching of the palms+, no eruptions. Diarrhea 4 times/ day. Max Temp- 99OF | 1,48,000
|
Placebo |
| 29/9/09 | Sleepless, app and thirst reduced, weakness and tiredness3, taste bitter, Afebrile all throughout | 1,75,000 | Placebo |
| 30/9/09 | Generals – much better,Particulars – better by 60-70% Afebrile | — | Placebo |
| 1/10/09 | Patient comfortable, moving around in the ward, all symptoms better Afebrile | — | Placebo |
| 2/10/09 | Completely better. Patient Discharged | — | Placebo |
The patient was discharged on 2/10/09 and was called for a follow up after 4 days.
After 4 days patient was well and had no fever, but had some weakness which was better than before and he had started attending work. Patient was started on constitutional medicine after fever settled down.
DISCUSSION:
Repertory is a tool of great help but, has its limitation. Quantitative aggregation presented by repertory software needs qualitative analysis. In this case Sepia does not come up in first five remedies, yet on qualitative studies in Materia Medica stands up prominently. Meticulous differentiation of remedies based on Materia Medica is brings down errors in prescribing.
CASE – 3
PRELIMINARY INFORMATION
Mrs. V.P.J AGE: 35 years SEX: Female Married since 14 years Housewife
DATE OF CASE TAKING: 15/9/09
Patient presented with low grade fever partially treated with allopathic medicines. Patient was not better hence came for homoeopathic treatment. Entire course of the illness was mild, insidious and slow. Patient did not complain of chills right from day one. She had headache, dullness with no desire to work, thirstlessness and bitter taste in mouth. Headache was severe led to weeping spells.
DAY – 1
| LOCATION | SENSATION | MODALITY | CONCOMITANT |
| General
Since 3 days Sudden onset
Head-forehead and generalmuscles and soft tissues,legs
Stomach Since the last 2 days 2-3 / day Skin since 1 day Ext mainly upper |
Fever initially low grade, later high grade with heat S. No chiils or rigors
No sweating
Partial betterment with medicines prescribed by general practitioners. But, fever persists
Pain3- aching
Nausea 3 Vomiting of ingested food and water Appetite reduced Reddish rash, occasional itching, no burning |
< noise2 > Binding head3
< eating3 < drinking2
|
DULLNESS3 – No desire to work
WEEPING3 PAIN WITH Thirstlessness3 Taste bitter3
|
Past History – Fever 9-10 years back,? Koch’s
Family History – Hypertension in both parents
OBSERVATIONS MADE OF PATIENT’S BEHAVIOUR-
- Patient was a quiet lady who spoke little and appeared to be mild
- Patient was always accompanied by someone for the follow up.
- She was afraid when spoken to about admission and the diagnosis
- She timidly followed everything told to her by the team of physicians and her husband.
GENERAL EXAMINATION-
- GC: Fair, Mild pallor +
- Weight: 49 Kg
- TEMP: 20F
- Pulse: 98/min
- BP: 120/80 mmHg
- Tongue: Moist white coated
- Skin: Macular erythematous rash on the upper and lower extremities, 1-2 petechiae, not palpable, non-tender, blanching + on pressure
SYSTEMIC EXAMINATION-
- S- Clear C.V.S- S1S2 heard
- A- soft, non-tender, L 1F, S 2F
- ENT- NAD
- Oral Cavity – Fordyce’s spots +
INVESTIGATIONS –
Hb- 13, WBC- 4,200 N:68 L:26E:4M:2, ESR- 18
Platelet count- 78,000
Ps for MP- Absent
Actions on Day 1.
- Patient advised admission for observation and investigations.
- Patient refused admission.
- Patient asked to follow up daily and sos.
- Prescription- placebo
DAY – 2
Bleeding PV started, Profuse, dark red, LMP- 15 days ago ? Menses early, ?hemorrhage Rash- same
Mild feverishness in evening, temperature not measured by patient.
No improvement in app and thirst
No other complaints
PROBABLE CLINICAL DIAGNOSIS- Dengue fever
REASONS–
- Sudden onset of fever with severe intense headache and myalgia.
- The appearance of rash at the de-effervescence of fever with its characteristic pattern of initial macular to later purpuric type are characteristic of dengue fever.
- A low leucocyte count.
- Falling platelets with appearance of bleeding is also more suggestive of a dengue infection.
ON EXAMINATION FINDINGS-
Mild icterus +, No pallor
T- 98
RS, CVS- Nad
PA- L2fp, S3fp
Skin- petechial spots + over the arms, blanching on pressure, non-palpable, erythematous macules developing over the abdomen and back
PLATELET COUNT- 50,000 DENGUE IgM-positive, IgG- positive FINAL DIAGNOSIS- Dengue fever with thrombocytopenia.
DAY – 3
PV bleeding persisted
Mild fever
Mild nausea, no other complaints
ON EXAMINATION-
Rash same, Purpuric spots on the lower extremities and very few over the abdomen.
Case taking of the chronic totality done to know the deep acting CONSTITUTIONAL REMEDY as well as the probable ACUTE REMEDY in relationship with the constitutional remedy.
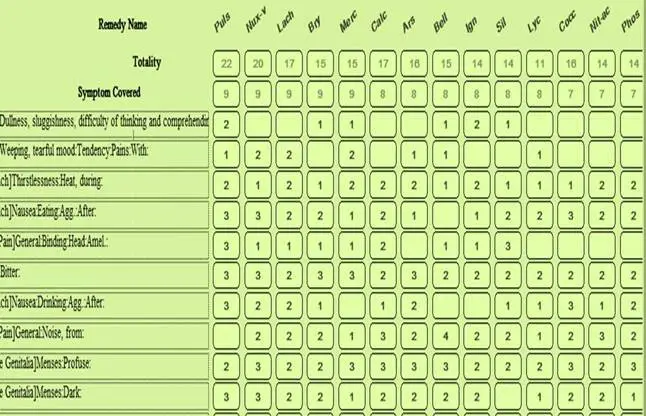
Acute Totality:
| 1. Dullness fever during
2. Weeping pain due to 3. Thirstlessness 4. Nausea < eating3 5. Head pain > binding the head3
|
6. Bitter taste3
7. Nausea < drinking2 8. Head pain < noise2 9. Menses profuse 10. Menses dark red |
CHRONIC TOTALITY
| 1. Sensitive3 reprimands to
2. Weeping tendency3 3. Mildness3 4. Timidity3 5. Aversion milk3 6. Aversion sour3 |
7. Aversion sweet2
8. Hunger agg3 9. Thermals- HOT 10. Menses dark3 11. Menses offensive3 12. Menses staining3 13. Head pain2 exposure to sun due to
|
REMEDY:
PULSATILLA was indicated in the acute phase and also as the constitutional remedy.
SUSCEPTIBILITY
| Criteria | Assessment | Reasons |
| Tissue
Susceptibility |
Moderate | Pace- slow, presenting in declining phase of fever
Pathology- acute fever with thrombocytopenia Characteristics- many, mental characteristic symptom +, physical gen +, particular++ |
| Sensitivity and Reactivity | High | Presence of characteristic mental as well as physical general symptoms in the fever episode as well as, at dispositional level |
| Pathology | Moderate | Functional reversible |
| Miasm | Dominant– Sycotic
Fundamental– sycotic |
Slow insidious onset, mild intensity yet prolong symptoms. Affection of the blood and RES with reduction of the platelet count and bleeding. |
| Vitality | Good | Vitals stable, |
Susceptibility of the patient indicated only moderate deviation from state of health, hence single dose of constitutional remedy should suffice. Pulsatilla was the deep acting constitutional force in the case. Patient had a sensitive and reactive system hence, PULSATILLA 200 single dose was given on 17/9/09.
FOLLOW UPS:-
| DATE | GENERALS | PLATELET COUNT | ACTION |
| 18/9/09 | App and thirst improved,No fever, body ache Rash reduced, Headache mild,PV bleeding reduced | 58,000 | Placebo |
| 19/9/09 | App and thirst further improved, energy levels better Rash improved, purpuric spots SQ, erythema reducing, bleeding reduced | 62,000 | Placebo |
| 20/9/09 | Better Purpuric spots also fading, no erythema, bleeding stopped | 1,68,000 | Placebo |
| 22/9/09 | Improved Only mild headache Rash- only 1-2 purpurae seen | 1,68,000 | Placebo |
| 29/9/09 | No symptoms | 2,35,000 | Placebo |
DISCUSSION:-
Case presented during de effervescence of the episode. Onset duration and progress clearly showed a slow mild, and insidious pace of illness. Thou patient did not have high grade fever lady was weeping due to headaches and also had other concomitants like drowsiness. Complete history was sought to obtain constitutional data. Constitutional data helps plan the treatment based on remedy relationships.
In this case constitutional remedy Pulsatilla itself covered the fever totality. Susceptibility assessment did not show any gross deviations from state of health as illness was in declining phase. Hence single stimulation was adequate for the case to sail through.
Key decision making points were stage of disease, pace and progress of symptoms, state of susceptibility and confirmation of acute and chronic totality coverage by Pulsatilla.
CASE – 4
PRELIMINARY INFORMATION
Name: R.C.N. Age: 25 yrs, Sex: Male, Religion: Hindu Education: student D.O.A: 8-09-2004
Patient presented with high grade fever sever chilliness and body pains since 2 days. He had travelled to an endemic area a few days ago, also had ice cream in the journey. Since the fever he had low appetite, bitter taste,thirstlessness and headache. Body ache was extremely severe associated with restlessness. Whole body was sore, patient was unable to lie down in one position for more than a minute.
| LOCATION | SENSATION | MODALITY | CONCOMITANT |
| Since 2 days
BLOOD & RES
SUDDEN |
Chilliness with fever
Fever in range of 104° F 105° F Severe Chilliness Severe Body Pains
Intense restless3 due to intense soreness of body Unable to lie in one position even for a minute but finds it difficult to move due to intense weakness |
A/F- Had lot of
Ice-cream 2 days back
|
Taste bitter
App low Thirst- reduced Headache
|
H/O- Having traveled to endemic area 2 days ago.
On Examination-key findings
Toxic look
T- 105 0F
Tonsils – Enlarged ++, Congested ++, Pus pocket ++
Abdomen- Liver not palpable, Spleen 2 cm
Differential diagnosis.
| Tonsillitis | Malaria | Dengue | |||
|
|
Ailments from ice cream.
Fever Tonsils enlarged, congested and with pus pockets |
|
High grade fever with chilliness.
Malaise and headache. Spleen 2 cm. |
|
H/o visit to Dengue endemic area
Abrupt onset of fever. Malaise, headache, backache. |
| | Spleen 2 cm. | ||||
| | Toxic look. |
INVESTIGATIONS:
8-9-04
Hb- 15 , TLC- 4,800/cmm. N-66, L-27, E-04, M-03, Platelet- adequate. SGOT- 16.6 SGPT- 44.7S.Bil. – 0.58Direct- 0.39
Malarial Parasite – Not Detected
Widal : O- 1:30 H – 1: 30
Totality of symptoms:- 1.Ailment from ice cream.
- Restlessness due to intense soreness and aching of body parts lied upon
- Feel too weak to move in bed.
- Fever with rapid prostration.
- Thirst decreased during fever.
- High-grade fever with toxic state.
- Painless inflammation of tonsils.
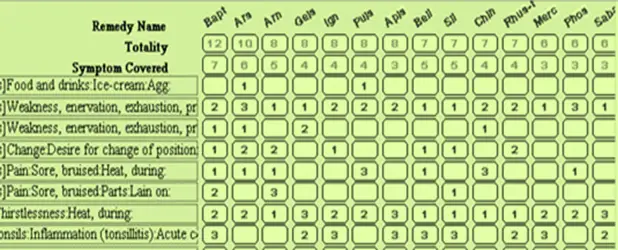
Remedy differentiation:
| BAPTISIA | ARS ALB | ARNICA | GELSEMIUM |
| Restlessness due to intense soreness and aching of body parts lied upon
Toxicity Thirstlessness Painless throat |
Mentally restless Physically exhausted. Thirsty – Drinks little and often | Intense soreness and aching of body parts lied.
Thirsty during chill
|
Drowsiness is more
marked Bodyache thirstlessness |
POSOLOGY:
| Susceptibility | High | Sudden, abrupt onset
Rapid pace Functional changes Characteristic symptoms |
Potency – 200 Repetition – 3 doses |
| Sensitivity | High | Characteristic symptoms |
REMEDY SELECTION: Baptisia 200 three doses 08.09.04.
FOLLOW UPS:-
| 8-09-04 | After first dose Soreness decreased+ ,feeling better. Fever range104 F – 103 F After second dose Body ache decreased+fever range same.
After third dose Weakness++Body ache++ Restlessness++ ,Fever102 F – 99 F |
| 9-09-04 | Asymptomatic |
| 10-09-04 | Asymptomatic |
| 11-09-04 | Purpuric rash, Sub-Conjunctival Hemorrhage, TLC 4200, Platelet count 90,000/cmm |
| 12-09-04 | Patient Asymptomatic ,TLC – 4600, Platelet count – 62,000/cmm |
| 13-09-04 | Asymptomatic, DENGUE IgM- 95.7 PANBIO units Platelet count 64,000/cmm |
| 15-09-04 | Patient Asymptomatic, Platelet count – 94,000/cmm |
| 16-09-04 | Patient Asymptomatic, Platelet count – 1,52,000/cmm |
DISCUSSION
Diagnosis in this case was inconclusive for first 3 days, though had suspicion of Dengue and Malaria, but because prescribing characteristics were present in the case homoeopathic treatment could be started even before conclusive diagnosis was arrived at. This is one advantage of using homoeopathy in early stage of diseases, even before classical pathological symptoms develops, because homoeopathic treatment is patient specific and not disease specific. However this doesn’t undermine importance of diagnosis for the homoeopathic physician. Diagnosis helpedto do follow up investigations, to anticipate complications, to understand natural course of disease visa vis course of disease in this specific case after homoeopathic treatment.
IMPACT OF TREAMENT:
| NATURAL COURSE | CASE | ||
| •••
• • |
Abrupt onset
3-4 days duration of first phase Biphasic-saddleback pattern –2 to several weeks Sequel with distress Complications- shock, death |
••••
• |
Abrupt onset
First phase –duration of 1 day. Biphasic –saddleback pattern – aborted No Sequel. No complications. |
CONCLUSIONS:
- Homoeopathic treatment helps in cutting short the clinical course of disease, reduction of distress of patient, prevention of complications & cutting short the convalescence in Dengue.
- Meticulous homoeopathic case taking during Dengue fever focusing on; onset, duration and progress of each symptom, fever pattern & concomitants during different stages is essential.
- Carefully elicited symptoms and systematic recording in LSMC format as suggested by Boenninghausen helps in analysis, of common symptoms from individualizing characteristics.
- Assessment of individuals susceptibility based on pace of disease, stage of illness, presence of homeopathic characteristics help in deciding the potency and repetition schedule. In Dengue, rarely is multiple dose repetition essential unless clearly indicated by severely deviated state of susceptibility like in DHF or DHS.
- Close follow up of dengue patient is essential. Mere sense of wellbeing, absence or reduction of fever should not be relied upon. Dengue is known for relapses and kickback fevers.Objective signs like platelet count, purpuric rash and active bleeding should be observed closely.
- After patient is afebrile for 48 hours or during convalescence, the deep acting constitutional remedy should be prescribed to prevent relapse.


Excellent clinical teaching article!
Excellent teaching article!
Excellent