Authors – M Vamsi Krishna Reddy, B Manasa, Navin Pawaskar
Reprinted with permission from the Indian Journal of Applied Homoeopathy where it first appeared. https://www.jimshomeocollege.com/ijah-publications/
Introduction: “We are always hearing that we homoeopaths are symptom hunters. We do nothing of that kind”. Successful homoeopathic prescribing depends on how much one pays attention to clinical work. The only successful homoeopathic prescribers are most observant clinicians”– Dr. Douglas Borland.
Pneumonia (Homeopathy Treatment for Pneumonia) was regarded by William Osler in the 19th century as “the captain of the men of death”. In spite of antibiotics in developing countries, and among the very old, the very young, and the chronically ill, pneumonia remains a leading cause of death. Pneumonia often shortens suffering among those already close to death and has thus been called “the old man’s friend”.
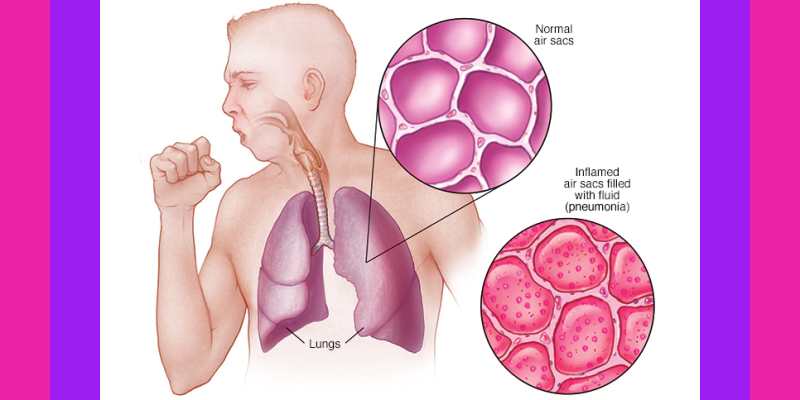
Definition: By definition pneumonia is inflammation of the distal lung parenchyma involving terminal airways, alveolar spaces, and interstitial lung tissue. Pneumonia causes accumulation of inflammatory cells and secretions in the alveolar spaces of lung, caused by an infection. Pneumonia is frequently encountered in community practice as well as in hospital based practice.
Epidemiology: Pneumonia affects approximately 450 million people globally (7% of the population) and results in about 4 million deaths per year. Incidence of community-acquired pneumonia is 5–11 per 1000 adults. Of these, 1–3 per 1000 will require hospitalization, and mortality in those hospitalized is up to 14%.
Age & comorbidity: Pneumonia caused by Chlamydia Trachomatis & RSV is seen in infants less than 6 months of age. Haemophilus Influenza pneumonias are seen in 6months – 5 yrs of age and M. Pneumoniae is seen in young adults, and those caused by M. Catarrhali seen in elderly with chronic lung disease.
Pneumonia caused by Staphylococci is seen in any age, and usually is hospital acquired in debilitated patients. Staphylococci is the commonest organism responsible for dissemination through the haematogenous route and causes rapid progress of Pneumonia.
Conventional treatment: The first thing to decide is suitability of treating a particular patient at home, at a hospital or in an intensive care unit, depending on the various risk factors for pneumonia. In conventional treatment identification of the organism and the determination of its antibiotic sensitivity are the keystones to appropriate therapy.Conventional treatment for pneumonia depends on the causative agent and the condition of the patient. For bacterial pneumonia, the physician will likely prescribe antibiotics unlike viral pneumonia which typically calls for treatment with plenty of fluids and rest, to prevent the pneumonia from progressing. Severe pneumonia treatment is with intravenous medications such as antibiotics, and with supplemental oxygen and placement on a mechanical ventilator to maintain lung function.
Classification of Pneumonia: It is important to understand various ways in which pneumonia is classified. Understanding of each component contributes towards complete diagnosis of pneumonia in a given patient. For example,community acquired lobar pneumonia caused to due streptococcus or Right lower lobe pneumonia caused due to aspiration. Each of these factors tells us about the characteristic of the pneumonia which helps in treatment and prognostication.
| Anatomical. | Etiological. |
| Nature Of Host Reaction. | Source Of Organism. |
Anatomical:
- Lobar: Parenchyma involved confined to lobe.
- Bronchopneumonia: Parenchyma + Bronchi involved.
- Interstitial: Confined to Interstitial Space.
- Aetiological:
| Bacteria. | Viral. |
| Protozoal. | Rickettsia. |
| Multiple organisms (Aspirated pneumonia.) | Non-microorganism. |
| Post-operative & hypostatic pneumonia. | Allergic pneumonia. |
- Nature of host reaction:
| Suppurative. | Fibrinous. |
- Source of organism:
| Community Acquired | Streptococcus Pneumonias. Mycoplasma Pneumonias. Haemophilus Influenza. Influenza virus. RSV. |
| Hospital Acquired | Staphylococcus Aureus.Enteric aerobic Gram –ve bacilli. |
| H I V – Infection Associated. | Pneumocystis Carini. M. Tuberculosis. |
| Aspirated Pneumonia. | Multi Organism |
| Non-Micro-organism c hemical | Lupoid. Drugs. Oil. Anticancer radiation. |
In-order to understand pneumonia and its manifestations from a homeopathic perspective, it is important to understand the anatomy (structural architecture) physiology (functions of lung tissues and ventilation as a process) and manifestations of altered anatomy and physiology in terms of signs and symptoms (form of illness in an individual).
Understanding the Structure of the Lung
The respiratory bronchioles, alveolar ducts, alveolar sacs, and the alveoli constitute the respiratory zone. The respiratory bronchioles, usually up to 3 in order, give rise to up to 9 generations of alveolar ducts. The walls of the respiratory bronchioles contain a little smooth muscle that is also present around the opening of the alveolar ducts. The alveoli are the actual gas exchange areas and are present as small outpouchings on the respiratory bronchioles and the alveolar ducts and aggregate to form alveolar sacs at the terminal ends of the alveolar ducts.
Function of Lung & its tissues
Ventilation: The respiratory drive is generated from the medullary centres and transmitted to the diaphragm and the intercostal muscles, the former being responsible for almost 80% of the ventilation.The descent of the diaphragm and expansion of the chest wall create a negative pleural pressure that lowers the alveolar pressure below the atmospheric, thus creating a pressure gradient for air to flow into the lungs. Expiration is a passive process. The upper zones receive more ventilation and the lower zones receive more perfusion. Airway resistance is the combination of mechanical factors that cause impediment to the flow of air from nose to the alveoli and back. Due to a tremendous increase in total cross-sectional area, as the bronchial tree divides distally, the resistance is greatest in the larger airways and diminishes distally. Compliance is the property of the lungs to expand in response to an applied change in pressure. Compliance is highest around the resting end expiratory position and reduces at very high and very low lung volumes. Low compliance indicates a stiff lung.
Gas Exchange: At rest, an adult person utilises 250 mL of oxygen per minute and exhales about 200 mL of carbon dioxide. The diffusion into the blood depends on the pressure gradient across the alveolo-capillary membrane and the surface available for gas exchange, as well as the chemical combination rate with haemoglobin, and inversely varies with the length of the passage and the thickness of the membrane. This ability of the lungs to transfer oxygen is called the diffusion capacity.
Gas Transport: Oxygen is transported in blood largely bound to the haem portion of haemoglobin and to a much smaller extent dissolved in the blood, 0.0031 mL per mm PaO2. The oxygen content of arterial blood (CaO2) is the sum of the bound and dissolved oxygen. Each gram of haemoglobin can carry 1.34 mL O2 when fully saturated.The actual delivery of oxygen to tissues is also dependent on the local blood flow that in turn depends on the cardiac output and the local regulation of blood flow in the particular tissue.
Pathology & Pathogenesis: Alveolar Macrophages process & present microbial antigens to the lymphocytes which secrete cytokines like TNF, IL -1. Cytokines modulate the immune process in T & B lymphocytes and facilitate the generation of an inflammatory responses and Cytokines recruit immunologic factors from plasma & further activate alveolar macrophage. Inflammatory exudate is responsible for local signs of pulmonary consolidation and systemic manifestation of pneumonia like fever, chill, myalgia’s &malaise.
Clinico-Pathological Correlations: The key element in clinic pathological correlation is the understanding of time dimension vis-à-vis evolution of illness. Clinico-pathological correlation helps understand the, pace & stage of disease, extent of infection, immunity of host and hence the susceptibility of the individual from homoeopathic perspective. Borland’s homoeopathic strategies for management of pneumonia are based on clinic pathological understanding of the patients. Different homoeopathic remedies get indicated based on individualistic features in succeeding stages of pneumonia e.g Aconite->Bryonia->Chelidonium-> Phosphorus->Kali Carb->Antimum tart etc.
- STAGE OF CONGESTION: Lasts for about 24 hrs and is characterized by vascular engorgement, Intra-alveolar fluid with Neutrophil, presence of numerous bacteria and grossly involved lobe will be heavy, boggy, red & sub-crepitant and clinically crepts are heard.
- STAGE OF RED HEPATIZATION: Increased Neutrophils & fibrin fill the alveolar spaces and massive exudation obscures pulmonary architecture. Extravasations of red cells causes the coloration seen on gross examination and White cells contain engulfed bacteria. There will be fibrinous or fibro-suppurative pleuritis. On Gross examination lobe appears – red, firm, & airless with a liver–like consistency, hence term HEPATIZATION. Clinicall, dullness, bronchial breath sound is noted.
- STAGE OF GRAY HEPATIZATION: Continuous accumulation of fibrin & progressive disintegration of inflammatory white cells & red cells. Fibrino-suppurative exudate give gross appearance of GRAYISH-BROWN, DRY surface. When bacterial infection extends in to the pleural cavity, the intra-pleural Fibrino-suppurative reaction is produced called EMPYEMA.
- STAGE OF RESOLUTION: Consolidated exudate within the alveolar spaces undergoes progressive enzyme digestion to produce granular, semifluid debris that is either: reabsorbed, ingested by macrophages, or coughed up.
In the above favourable condition, lung parenchyma is restored to its normal state. Pleura reaction also similarly resolves, but more often it undergoes organization, leaving fibrinous thickening or permanent adhesions. Clinically, crepts are noted.
- ATYPICAL PNEUMONIA: An acute febrile respiratory disease characterized by patchy inflammatory changes in the lung, largely confined to alveolar septa & pulmonary interstitium. The term ‘ATYPICAL’ means lack of alveolar exudate. Caused by M. Pneumoniae and common viruses are Influenza virus type A & B, RSV, Adenovirus. Clinical presentation starts as A URTI – Common cold. Gradually extension in LRTI
Pathologyofatypicalpneumonia: Patchy or whole lobes bilaterally or unilaterally lungs are involved and there is no obvious consolidation .Pleura is smooth, & Pleuritic or Pleural effusion are infrequent. In many patient there are intra-alveolar proteinaceous material, a cellular exudate, & a pink hyaline membranes lining the alveolar walls, similar to those seen in a hyaline membrane disease of infants. These change reflect similarly to that seen diffusely in the adult respiratory distress syndrome.
Risk Factors:
- Factors affecting resistance in general;
Chronic Disease, Immunologic Deficiency, being treated with immunosuppressive agents, Leukopenia, Unusually virulent infection.
- Factors affecting clearing mechanisms:
Ultimately leading to aspiration of Gastric Content e.g Loss or Suppression of Cough Reflex, Coma, Anaesthesia, Neuromuscular Disorders.Chest Pain.
- Injury to muco-ciliary apparatus:
Impairment of Ciliary function, destruction of ciliated epithelium, SCigarmoking, inhalation of hot or corrosive gases, genetic Disturbances like Immotile Cilia Syndrome.
- Interference with the Phagocytic / Bactericidal action of alveolar Macrophage:Alcohol, Tobacco Smoke, .Anoxi
- Pulmonary Congestion &Oedema.
Congestive cardiac Failure
- Accumulation Of Secretion:
Cystic Fibrosis, Bronchial Obstruction.
Clinical manifestations: The diagnosis of pneumonia is to be considered in any patient who has newly acquired respiratory symptoms (cough, sputum production, and/or dyspnoea), especially if accompanied by fever and auscultatory findings of abnormal breath sounds and crackles.
The major symptoms of community acquired acute bacterial pneumonia are abrupt onset of high fever, shaking chills, and cough producing mucopurulent sputum; occasional patients may have haemoptysis. When pleuritis is present it is accompanied by pleuritic pain and pleural friction rub. The whole lobe is radiopaque in lobar pneumonia, whereas there are focal opacities in bronchopneumonia.
Symptoms Fever, rigors, malaise, anorexia, dyspnoea, cough, purulent sputum (classically ‘rusty’ with pneumococcus), haemoptysis, and pleuritic chest pain.
Signs High grade temperature, cyanosis, herpes labialis (pneumococcus), confusion, tachypnoea, tachycardia, hypotension, signs of consolidation (diminished expansion, dull percussion note, increased tactile vocal fremitus/vocal resonance, bronchial breathing), and a pleural rub.
Types (Anatomical)
| Bronchopneumonia | Lobar Pneumonia |
| Anatomy | |
| When the process is restricted to alveoli contiguous to BronchiPatchy Consolidation of the lung tissue Extension of preexisting bronchitis or bronchiolitis | Involvement of large portion of a lobe or of an entire lobe |
| Age | |
| Common age infancy | Uncommon in infancy & in late life |
| Organisms | |
| Common agents: Staphylococci, Streptococci, Pneumococci | Common Agents: pneumococci, Streptococcus pneumoniae |
| Pathology | |
| Consolidated area of acute suppurative inflammationPatchy Consolidation of lung through one lobe more often multi lobar & frequent bilateral & Base because of tendency of secretions to gravitate in to lower lobes | Wide spread fibrino-suppurative consolidation of large area even entire lobe 4 stages of inflammatory response 1.Congestion2. Red Hepatization3. Grey Hepatization4. Resolution |
Investigations:
- Chest X Ray PA View.
- Oxygen saturation and arterial blood gases if SaO2 <92% or severe pneumonia.
- CBC, U&E, LFT, CRP, atypical serology.
- Urine pneumococcal (and legionella) antigen.
- Viral throat swabs if appropriate.
- Blood cultures if pyrexial.
- Pleural fluid may be aspirated for culture.
- Bronchoscopy and broncho-alveolar lavage if the patient is immunocompromised or on ICU.
Diagnosis:
- CXR:
- i) Presence & Location of pulmonary infiltrate. ii) Assess extent of the pulmonary infection. iii) Detect pleural involvement, pulmonary cavitations or hilar lymphadenopathy. iv) Gauge response to Rx.
- Sputum examination.
- CBC & ESR.
Complication of Pneumonia:
1.Lung abscesses
- Spread to the pleural cavities empyema.
- Spread to the pericardial cavity suppurative pericarditis.
- Development of bacteraemia with metastasis abscess formation in other organs.
- Pleural effusion, respiratory failure, septicaemia, myocarditis, cholestasis jaundice, acute kidney injury.
START HERE
HOMOEOPATHIC MANAGEMENT
“Don’t get : panicky, give too low a potency, repeat too often, paralyze your patient’s heart with digitalis or ease his pains with morphine or try to replace simillimum with a tank of oxygen –they won’t work” – Dr A & D T Pulford quotes in his book Homoeopathic Leaders in Pneumonia,highlighting the power of simillimum in management of pneumonia.
Management of Pneumonia depends upon individualization based on; assessment of clinical stage of disease, symptomatology, level of Susceptibility &Miasm of an individual patient. In a nut shell, selecting a simillimum after constructing the totality of symptoms, based on symptoms of a disease and symptoms of an individual as whole.
Borland in his book describes stages of pneumonia and classifies probable indicated remedies according to phases and stage of disease. Group I incipient pneumonia, Group II frank pneumonia, Group III complicated pneumonia (mixed infection, aspiration), Group III complicated pneumonia (Bronchopneumonia). Group IV late pneumonia. Each of these groupings is based on the stage of disease and state of susceptibility.
Assessment of susceptibility depends upon state of pathology, clinical pace of development of disease, characteristic symptoms of patient and the underlying Miasm. Thus, symptoms related to Structure, Function & Form point us to select a suitable drug for the patient. Understanding of susceptibility andmiasm guides in the therapeutic approach; an acute or a deep acting chronic remedy, way of repetition of dose and level of potency.
“The whole of your success in homoeopathic prescribing in pneumonia depends on your power of recognizing which symptoms are common to every case of infection by a specific organism and which are dependent on the individual reaction of the patient who is infected.”- Borland
Five pneumonia experiences are presented as sample cases to demonstrate the homoeopathic approach and the different strategies used in management of pneumonias.
CASE 1
Mr TR 16yrs/M Occupation: Student
Presenting complaint :Cold with nose block & sneezing from 3 days. Presented with history of exposure to cold draft of air in evening 3 days ago. From the 4th day developed sudden high-grade fever with chilliness and cough < drinking cold water. C/o associated with increased thirst for large quantity of cold water.
Physical examination: T-104F. P-140/Min. RR-48/Min. RS- Air Entry decreased in Left Lower Lobe, crept – Left Lower Lobe.
X-ray : inhomogeneous opacity left lower zone.
Diagnosis :Acute Community acquired Pneumonia
Case analysis :Structural changes in this case are in early acute stage of congestion in lung tissue before the exudative stage. Functional changes are ↑ Temp 104 F, PR 140/min, ↑ cough reflex, no altered gaseous exchange, RR 48/min, RS AE ↓.
Form of presentation: symptoms are rapid in onset with A/F getting cold when heated, increased thirst for large quantity of water, cough < drinking cold water which indicates good number of characteristics.
Rapid onset with robust symptomatology in first stage of pneumonic congestion & inflammation indicate minimal deviation from original state indicating good susceptibility with dominant MiasmbeingPsora. Overall the prognosis of the case is a good one and we should expect swift resolution with a few doses of indicated medicine.
Totality of symptoms:
- A/F exposure to colddraft of air.
- Increased thirst for large quantity of cold water.
- Sudden onset
- High grade fever with chilliness Cough < drinking cold water.
Related remedies: Remedies indicated in first stage of inflammation should be differentiated in this case. Bell can be differentiated from Aconite by its extreme sensitiveness to external impressions like sound, light, least touch, movement. Cold stage is more predominant in Aconite unlike heat stage in Bell. FerrPhosis another drug to be differentiated from Aconite by less marked anxiety & fear. Aconite has bright flushing face appearance whereas Ferr-Phos has localized flush or alternate pallor and flushing face. Aconite has evening aggravation unlike FerrPhos, which has early morning aggravation.
Final Prescription: Aconite
Remedy response: With ACONITE 1000 C repeated every 4th hourly, fever came down next day morning, and cough was better 50 % in 2 days. Aconite was stopped on 3rd day and dose of Cal Carb 200 as constitutional remedy on 4th day ameliorated the patient completely and hastened the convalescence.
Discussion: Patient had come in first stage of congestion of lungs, sudden onset with good characteristics which indicated robust susceptibility with psoricMiasm in background which allowed Aconite the indicated remedy to abort the episode midway, thus preventing the disease to go into consolidation phase of red and grey hepatization.
Borland’s advice on managing pneumonia by creating crisis
By the administration of higher potencies, – you will find that you abort the disease. It does not run its normal course; the duration of the illness is very much shortened and you have an anticipated crisis.
Case 2
Mrs. AR. 25 yrs / F Occupation: Housewife. Patient was brought with support of relatives to the hospital.
Presenting Complaint :Complaints started from 12 days after drinking cold water. First 4 days had watery nasal coryza that gradually became thick yellowish with occasional cough. On 5th day patient got wet & within 2 hrs developed high grade fever with chilliness, weakness &headache. Headache was aggravated looking down, during fever & standing from sitting position. Patient had become irritable and wanted to be left alone.
On 7th day Illness increased with scanty expectoration, chest pain aggravated coughing, deep breathing. Vertigo with fever. Thirst increased for every 10 min. Bitter taste with appetite decreased. On 10th day developed loose watery stools 2-3 times a day, yellowish offensive in small quantity.
Physicalexamination: GC Unsatisfactory, dehydrated look, had to be carried.
Temp 104 F, P/R 124/MIN, R/R 48/min, Tongue dry thick white coated,
Respiratory System: Bronchial breathing in Right Upper Zone.
Investigation :Hb: 11.2. WBC: 11,800 N: 78 L: 20 E: 1 M: 1 ESR: 98. SGPT: 40, MP –veWidal: O: 60, H: 1:60 CUE : Alb: ++++, RBC: Occ, PC: 18–20/hpf, PC casts: 6-7/hpf.
X-Ray Chest: Rt. Upper Lobar Pneumonia with Loculated effusion.
Diagnosis :Acute community acquired bacterial lobar Broncho Pneumonia.
Case analysis: Structural changes include inflammation of mucosa, serosa & Rt. lung upper lobe parenchyma. Stage of congestion lands into stage of red hepatization with fibrino suppurative exudation.
Functional changes seen as Nasal &Mucociliary Clearance, Cough reflex, Compliance of Lung – Hyperventilation, altered gaseous exchange, RR 48/m.
Form of presentation of symptoms are slow and gradual, watery coryza becoming thick with occasional cough. High grade fever with chilliness, - cough with scanty sputum & chest pain indicates moderate to ↑ susceptibility & dominant MiasmSycotic.
Totality of symptoms:
- A/F Exposure to heat, Suppression.
- Concomitants thirst for large quantity often, Irritability & Headache.
- Slow gradual onset with early pleural involvement.
- Dryness of all mucous membranes.
- Dry hard cough with sharp stitches in the chest Chest Pain < motion, hot weather, > pressure, rest.
Related remedies :Remedies in second stage of Inflammation like Bryonia, Chelidonium, Sangunaria need to be considered for differentiation here.
Chelidonium appearance is slightly yellowish tinge unlike bluish dusky in Bryonia. Both have irritability but Chelidonium is snappish unlike Bryonia who wants be left alone undisturbed.
Bryonia pains > lying on painful parts while in Chelidonium> sitting up or leaning forward.
Chelidonium desires warm food & drinks unlike Bryonia has < from warmth in general.
Sanguinaria can be differentiated by circumscribed redness of cheeks of face, unlike Bryoniathat has dusky hue. Sanguinaria has < cold weather, lying down while in Bryonia> cold in general, lying on painful side.
Final Choice: Bryonia
Remedy response: BRYONIA 200 4th hourly gradually improved patient of dehydration and fever in 2 days and of chest pain in 4 days.
Discussion: As compared to the first case this case had slow gradual onset.Symptoms evolved slowly yet the characteristics were present indicating moderate deviation from state of health. Thus the susceptibility was in moderate zone. The dominant SycoticMiasm in the case was indicated through its slow onset, stage of consolidation – Red Hepatization, Scanty yellow discharge, stitching pains.
Thus, a case which has already reached stage of Hepatization, with moderate susceptibility and dominant MiasmSycotic, should be allowed to resolve through lysis and run the course from Hepatization to resolution. One should not attempt to abort the course as in earlier case which was in first stage of inflammation with Psoric back ground.
Borland’s advice for Repetition of doses
- “When you are using low potencies, you have to keep up your drug administration right throughout the course of the disease”.
- “When you are using the higher potencies, it is advisable to continue the administration of the selected drug until the temperature has reached normal and has remained normal for at least 6 hours”.
- “In the average case where you are using a low potency (30 and below) it is quite sufficient to give the drug about once in four hours”.
Case 3
MRS SA 28 Yrs/F Occupation : Teacher
Presenting complaint :Patient had a frightful experience 24 hours before from which she recovered but developed cough and high grade fever with chills from 2.30 am. Cough with blood-streaked sputum. Associated with chattering teeth during chills, extremity pain, and pain in Rt dorsal back aggravation inspiration, night in general. App low & taste insipid. Thirst for large quantity cold water. Heat sensation in mouth & eyes. Weakness. Hoarseness worse talking.
Physical examination: T: 103 F. P-120/min. Throat – congestion. Dry Tongue. Respiratory System: Dull note on Percussion, reduced air entry in Rt Lower zone, occasional crepts Rt. Side.
Investigations :Hb: 13 gms WBC – 19400 L- 19 N – 77 E – 03 M – 01 Plat- 32 000
Chest X Ray: Small patch of consolidation Rt. basal & Para cardiac region
Diagnosis : Broncho pneumonia.
Case analysis. :In this case structural changesin lungsshows congestion with early hepatisation. Functional changes show rapid onset of respiratory distress with high grade fever & chills, weakness with app decreased, cough with bloody sputum. Form of presentation, complaints are a/f fright, rapid onset with progress, fever< night with extremity pain, Heat sensation with burning eyes & mouth, Hoarseness < talking.
A good number of characteristics with cause and effect relationship is indicative of moderate deviation from state of health indicating moderate susceptibility. Rapid onset of symptoms, bloody sputum, and exhaustion early in the course of illness are indicative of lurking Tubercular Miasm in background.
Totality of symptoms: Insidious onset ending in severe or rapid disease.
- A/F
- Thirst for large quantity cold water Fever with weakness, Burning pains < night.
- Thirsty with dry tongue
- Bloody Discharge
- Small patch of consolidation Rt. Lung basal region.
Related remedies: Remedies like Merc Sol , Phosphorus & Kali Carb need to be differentiated. Merc sol can be differentiated from Phosphorus by discharges which are offensive, in this case the sputum is bloody. Merc sol has increased thirst for cold water with moist tongue while phosphorus increased thirst for ice cold water with dry tongue. Kali Carb has early pleural involvement with stitching pains. Kali is thirstless, is worse during early hours of the morning, is better sitting erect and has profuse perspiration. Phosphorus covers the causation of fright, has rapid pace of disease, characteristic burning pains, thirst for cold water profound weakness since the beginning of illness, bloody sputum most important the tubercular Miasmis in the background.
Final Selection: Phosphorus.
Remedy response: After starting Phosphorous 200 with cautious repetition, maximum up to three times day gradual improvement was seen. By third day there was no rise of temperature. Appetite & sleep improved in 5 days and cough subsided in 10 days. Patient received constitutional medicine to complete the recovery process.
Discussion: Patient was brought to op in 2nd stage of Red Hepatization pathology. Sudden onset & progression of symptoms, with good characteristics indicated good susceptibility of patient with predominant Tubercular Miasm. Hence patient was treated with a remedy which has tubercular base with cautious repetition. In this case physician followed 3 points by Dr. Pulford in his book Homoeopathic Leaders in Pneumonia – “Don’t get panicky, Don’t give too low a potency, Don’t repeat too often.”
Case 4
Mast. A. 11 months. / M. known case ofVHD with MR & Delayed Milestones.
Presenting complaint: Child was brought withcold & coryza with mucoid nasal discharge & Mild Fever since 4 days. Associated with Thirst decreased & Mucous Stools 2-3 times. Based on which Pulsatilla 200 was prescribed but without relief.
From 5th day Cough increased with high grade fever. Rattling in chest, with difficult to expectorate sputum, 1-2 sticky vomiting with drowsiness & weakness. Cough < Lying down > Carrying on shoulder. Associated with Decreased appetite & thirst with white coated tongue.
Physical examination T: 102.4F RR: 50/min. P: 140/ min. RS: AE in Right Lower Lobe, Crepts Right Lower Lobe +
Investigation: Chest X Ray: Right Lower Lobe homogenous opacity- Consolidation
Diagnosis: Aspiration pneumonia
Case analysis: This case presented with structural changes as overstimulation of pneumogastric nerve, causing increased mucous secretions. Congestion in lungs with exudative inflammation. Functional changes with hypersecretion of mucous, capillary congestion, spasm of respiratory muscles with altered gas exchange ↑ Respiratory Rate 50/ min.
Form of presentation of symptoms is rapid travel from Upper Respiratory Tract to Lower Respiratory Tract. Rattling cough, can’t be raised, >Expectoration, Vomiting. Lacks reaction, weakness. Tongue white coated. This indicates ↓ significant deviation from original state of health, indicating susceptibility is debilitated. Lack of ability to react, exhaustion, better by expectoration with Mental Retardation, &VSD , syphilitic Miasm was lurking in background.
Totality of symptoms:
- Drowsiness & exhaustion
- ↓ Thirst with coated tongue
- Cough with rattling chest
- Cough with difficult Sticky expectoration Cough ending in Vomiting < lying down.
Related remedies: Remedies like Carbo Veg, Antim Tart and Ipecac need differentiation. Carbo veg comes close due to exhaustion and lack of reaction, but can be differentiated due to its more bluish hue, coldness of skin and marked thirst, unlike Ant tart which, is pale &thirstless. Ipecac also has rattling cough with nausea and vomiting with clean tongue. Ipecac discharges are blood stained and accompanied by severe bronchospasm. Alertness of ipecac is preserved, child screams, howls cries, unlike drowsiness in Ant tart. Ipecac has blood streaked sputum unlike scanty mucoid sputum in Ant tart. Ipecac < lying down unlike > lying down on right side in Ant tart.
Remedy response: Ant -tart 200 4th hourly was prescribed. Fever went down first, drowsiness improved next day followed by appetite and thirst. Cough improved and respiratory distress improved over 5 days On 9th day CXR showing total Resolution.
Discussion: This case relies on Dr. Borland’s writings on healing by lysis where a case is managed cautiously, only controlling the symptoms and preventing the complications. The debilitated susceptibility is supported till it tides over the crisis safely. The aim here is to preserve life and not to abort the disease aggressively.
CASE 5
Mast: Y.P Age: 2 ½ yrs/Male
Presenting complaint
Child had come with watery nasal coryza and cough from 4 days with low ↓Appetite & dullness. From 5th day developed high grade fever with chilliness < evening. Had 1 episode of vomiting associated with irritability, carried desire to be & teeth grinding.
Past history 2 episode of Lower Respiratory Tract Infection, 2 episodes of Acute Gastroenteritis.
Physical examination T– 1010 F, P/R – 110/min, R.R. – 23/min Respiratory System – Bilateral Crepts + CVS- S1S2 normal P/A- Soft
Investigation Hb 9.4%, WBC 12,400 N 74, E 2, M 2, L 22 Chest X ray left Lower Lobe Homogenous opacity consolidation+
Diagnosis Pneumonia (Late stage)
Mental generals Active and playful child. Dominating – While playing expects that others should obey his rules, keeps finding mistakes with others. Irritable – on slightest provocation. Egoistic – Does not readily mix with people and judges their suitability before befriending them. Does not like to be scolded and becomes angry. Sharp memory – Good memory of events, names etc.
Physical general Craving – Egg , Garlic , Chana. Hot patient.
Case analysis
In this chronic case structures affected are lungs with Left Lower Lobe consolidation & GIT. Functional changes are ↑ Mucous secretion→coryza, GE; ↑ Cough reflex; ↑ Temparature& PR. Form of presentation of symptoms are as Gradual pace onset, Evening ↑ Temp., Weakness & desire to be carried, Availability certain characteristic mental generals. This all indicates moderate deviation from state of health & ↑robust susceptibility
Totality of symptoms
| S.NO | Chronic Totality | Acute Totality | |
| 1 | Dominating/Egoistic | Irritability heat during | |
| 2 | Irritable | Carried desire to | |
| 3 | Sharp memory | Thirst increased for | sips freq. |
| 4 | Desire Egg, Garlic, Chana | Fever < evening | |
| 5 | Hot |
Related remedies
Sulphur
- Lt sided affinity
- Irritable, full of anxiety & fear.
- Fever with more violent Heat.
- Thirst for stimulants.
- < 11am
- Irritability
- Aversion to business due to laziness.
- Sleep- wakes up happily singing in morning.
Lycopodium
- Sided affinity.
- Fever with icy coldness as if lying on ice.
- Thirst for Warm drinks.
- < 4-8 pm
- Irritability & aversion to undertake new things
- lack of confidence.
- Sleep- sadness on waking up.
- < warm weather, 4-8pm Chest pain > sitting up.
Kali carb.
- < cold weather , 3am
- Chest pain > sitting with leaning forward.
Final Selection: Lycopodium
Of the three remedies Lycopodium covered the acute & chronic totality of the patient. Hence it was the choice of remedy over Sulphur and kali carb.
Remedy response
| First Day | Temp – 1010F, Cough ++ | Lycopodium 10m single dose |
| Second Day | Fever > but relapse cough > but relapse | Lycopodium 10m single dose |
| Third Day onwards | No complaints, X ray chest with complete resolutionof lung parenchyma | Placebo |
Discussion
Patient had two episodes of lower respiratory tract infections before this episode. Hence a drug which suits both acute & chronic symptom was best selected. There were characteristic generals in totality including mental generals in both acute and chronic totality, indicating highly robust susceptibility hence high potency in single dose was used. Lycopodium was used in high potency with the hope of cutting down or aborting the course of disease. Since the susceptibility was robust and correspondence of remedy complete, the physician took the risk of aggressive strategy through creating a crisis as suggested by Borland.
Borland’s advice on role of potencies
- With too low potencies you avoid the complications of the disease, make patients more comfortable and reduce mortality rate. But by this method you do not reduce the duration of disease.
- By the administration of higher potencies, – you will find that you abort the disease. It does not run its normal course; the duration of the illness is very much shortened and you have an anticipated crisis.
- As far as the high potencies are concerned, I think it is wiser to give the drug every 2 hours, the reason being that you want a number of stimuli in a comparatively short period of time in order to obtain the crisis within 12-24 hours.
Debate of Strategies Lysis V/S Crisis.
Answer to the debate lies in assessment of susceptibility and Miasm.
- If the indicators of susceptibility are robust; like characteristics are robust, pathology is just setting in, early stage of disease, general condition is good, no compromise in vitality and essentially psoric response from patient and if the correspondence of indicated remedy is complete, it is safe to aggressively barge in by creating crisis and cut short or abort the course of illness.
- If the indicators of susceptibility are weak; Not much characteristics, well established inflammation or its complication, general debility, vitality compromised, underlying co morbidity essentially, tubercular or syphilitic miasm expressions, it is better to follow slow yet safe method of using low potency. Support the susceptibility to withstand the disease force and allow it to tide over. Choose steady lysis of disease. Patient is comforted by relief in symptoms and prevention of complication while disease runs its full course.
Conclusion
- Homoeopathy has the potential and the capability to counter and diffuse infections based on the principle of individualisation. Homoeopathic approach in pneumonia is no different.
- Totality of symptoms; i.e. the pathognomonic common symptoms of the disease caused due to infection and Characteristic symptoms exhibited by the individual as a reaction to the infection are our guiding post to establish diagnosis and select homoeopathic remedies, respectively.
- Diagnostic knowledge and skills are critical for suspecting, identifying and confirming the diagnosis of pneumonia. Clinico- pathological correlations are essential for understanding inflammatory stages of pneumonia and hence the group of remedies based on stage & type of pneumonia as suggested by Borland.
- Groups suggested by Borland in 1939 based on the tissue affinity, still hold true and are seen by contemporary physicians in practice. Group I (incipient) Aconite, Belladonna, ferumPhos. Group II (Frank) Bryonia, Chelidonuim , Phosphorus, Group III( Bronchopneumonia) Nat Sulph, Puls, lobelia Senega, Group III (Complicated) Lach, Rhus Tox, Merc, HeparSulph , Pyrogen Group IV (Late) Carbo Veg, Ant. Tart, Kali Carb, Lycopodium, Ars Alb, Sulph.
- In homoeopathic prescribing for pneumonia, the endeavour is to find a drug that will cover not only the actual pathological picture but also reaction of the individual patient to the infection. Individual reactions are exhibited through peculiar symptoms like; Causations, Generals, Concomitants, Modalities, and Sensations.
- Case taking should focus on evolutionary picture of the disease on day to day basis. Patiently, each symptom and sign should be elicited and recorded on time line to understand onset duration and progress.
- The trio of pace of disease, stage of pathology and evolution of characteristic symptoms are the basis of susceptibility assessment. Identifying pace and stage of the disease in pneumonic inflammation goes a long way in providing assessment of susceptibility of the patient.
- Miasm plays a significant role in deciding how a pneumonia is going to progress and how an individual will react in the course of the illness. Identifying phases of pneumonia from Posra to Syphilis helps in formulating strategy.
- Strategy of management of pneumonia e.g Crisis or Lysis, use of acute or constitutional remedy, choice of potency and repetition is based on understanding of susceptibility and miasm of a given case.
- Homoeopathic management of pneumonia is an art formulated on scientific principles of Homoeopathy which can be learnt and perfected by practice alone.
References:
- API Text Book Of Medicine 9th Edition (2012 )
- Current Medical Diagnosis and Treatment 2015
- Homoeopathic Leaders in Pneumonia By Dr. A Pulford, Dr.D.T Pulford, B Jain Publishers, Reprint Edition 2004.
- Organon Of Medicine By Samuel Hahnemann, 6thEdition, Reprint Edition 2003, Ibpp Publishers
- Oxford Hand Book Of Clinical Medicine 2014
- Pneumonias By Dr. Douglas M.Borland, B Jain Publishers, Reprint Edition 2003, 2008.
- Robbins Cotran Pathologic Basis Of Disease 9th Edition