Dr Mirjana Zivanov, Dr Stojan Primovic, Dr Andreas Kelemen
Classical case taking and case analysis are irreplaceable tools of every homeopath, but there are some critical points in this process that could be improved. We have focused on the following three in the creation of the Matrix method:
- In the process of case taking one of the key difficulties is to get a complete and accurate picture of the patient’s mental, emotional and physical state. Because a patient forgets or avoids providing information that may prove to be crucial for the entire process, a homeopath needs to find a way to get past all of these conscious and unconscious barriers. Therefore it may take a long time for the patient to open up. The patient may sometimes get tired of waiting and move on.
- In the process of case analysis a number of symptoms are chosen by a homeopath as most significant and key to the case. This step depends very much on skill, experience and talent that is not equal in all homeopaths, meaning that we may expect that many mistakes are made at this point, in everyday homeopathic practice.
- In a case a homeopath gets, or more precisely chooses, there are a number of symptoms and themes, and she needs to associate all of them with a single homeopathic remedy – Simillimum. Since there are a great number of homeopathic remedies, finding the right remedy for a chosen set of symptoms may be quite challenging, especially because both of the previously defined critical points of case taking and case analysis may influence the choice of symptoms. There are many similarities and differences of homeopathic remedies that we may find described in great detail in a repertory. There is still a question of a point, a missing link, between a symptom and a remedy, a small number of general categories, defined by many symptoms and shared by many remedies. Also, by defining the relations between these general categories we would get an insight into the relations of symptoms and remedies.
Much of homeopathic education is focused on preparing a homeopath to recognize the key symptoms and themes in a case-taking, but we shouldn’t forget there is another person there as well – the patient, with truthful unconscious information usually hidden under the mask, sometimes quite deeply. The issues, contents of unconscious, most important for the person, are associated with intense, highly charged, emotions and behaviors. Some psychological techniques may be of great help in unlocking the contents of the patients unconscious, so we were looking for a fast and accurate technique that could provide the most intense emotions and sensations of a patient, and simple enough to be used by a homeopath with no psychological training. We have found that the best suited technique for this purpose, to our knowledge, is the Deep PEAT technique by Z. Mihalovic – Slavinski. This technique may be included in a group of psychological techniques known as Meridian therapies, because the subject taps certain points on his/her face, body or fingers that are placed along meridians (path through which the life-energy known as “qi” flows in traditional Chinese medicine), hence the name. There has been an almost three decades long discussion in psychology on the effectiveness of meridian therapies, but even the results of their most vocal critics have found that these techniques are effective only not because of use of the meridians.
Meridian therapies are based on the idea of using tapping or pressing on a sequence of acupuncture points, located on main meridians, during the psychological treatment, basically using distraction and desensitization paired with exposure[1] – a well established psychological treatment technique[2],[3]. While it was shown that “tapping (or pressing) of meridians” was not a critical mechanism, the tapping and pressing of any points, as instructed by the therapist, has shown significant reductions in fear for all 3 groups that used tapping variations[4] but not for the control group[5]. It is important to point out that two of these three groups were also control groups regarding the use of points on meridians[6]. The other key element of this treatment technique is exposure, and since it is often difficult to achieve in clinical settings[7], the imaginary exposure is commonly used. Since these findings didn’t show these techniques to be ineffective, just that there is no connection to meridians, we’ve had pursued this path.
The Deep PEAT technique, is a process that usually lasts up to half an hour and gets us the deepest pair of opposites of a person, called the Primes, and a line of content that leads to it. Originally in the technique, the prime goal was to get and integrate this deepest pair of opposites – the Primes, while the other contents are a byproduct. But for a homeopath trying to find the patient’s Simillimum, the chain of these other contents are usually just as important, and often even more so. These contents highlight the most important issues in the case-taking, and often open up a number of issues that didn’t even come up in the case taking. This gives a much more complete picture necessary for finding the Simillimum. So, while in the Deep PEAT process the aim is to get to the Primes as fast as possible, in as few steps as possible, for a homeopath using this technique the aim is to get as much content as possible.
The First Step
The first step of the Matrix method is doing the Deep PEAT process, after the classical homeopathic case-taking, but aiming to get as much content as possible before getting to the Primes, because these are the emotions, sensations and behaviors with highest emotional charge – the key symptoms and themes we need for repertorisation. This may reduce the risk for the homeopath of choosing an inadequate set of key symptoms and themes from the case taking.
By using the Deep PEAT technique after the case taking, we may significantly improve the first critical point we have listed at the beginning, because it can assist the patient in opening up. Also by modifying the aim of the technique for use in homeopathy, we may get a longer chain of contents, for the case analysis.
The Design of the Matrix Model of Behavioral States
The relations of the contents we have got in the previous step, are parts of the bigger picture of the general behavior and emotional states. For better understanding of the relations between the contents we have got from the patient, as well as their effect on the complete picture of a patient, and understanding the patient’s miasm, we have created a three-dimensional model of general behavioral states in relation to the three monoamines (serotonin, dopamine and noradrenaline) – the Matrix model, and it’s flattened two-dimensional version, the Tetractys model, named after the ancient Pythagorean symbol of tetractys, that turned out to be very similar to this flattened model. The chain of contents we get from the Deep PEAT technique basically consists of emotions, as well as sensations and thoughts that express the underlying emotion.
People are expressing many different emotions, using even more words, but are all those emotions completely different from each other, or are there significant similarities that allow us to group all emotions in just a few clusters?
Charles Darwin in The Expression of the Emotions in Man and Animals listed over thirty emotions, classified into seven clusters. Ever since this groundbreaking work scientists have argued over whether or not there is a finite number of basic emotions at all[8]. Certain emotions may be grouped in clusters because they share an underlying pattern of behavioral-neuro-endocrine control, in which monoamines play a vital role.
Monoamines are phylogenetically ancient signaling molecules and it has been found that they are involved in behavioral control in a wide range of species from humans to structurally simple organisms such as nematodes[9],[10] . The fact that many allopathic psychotropic drugs, like antidepressants and antipsychotics act by interfering with the monoamine system, may illustrate the importance of monoamine systems in human beings[11].
The three monoamines essential to behavioural-neuroendocrine response patterns are serotonin, dopamine and noradrenaline[12]. A certain relation of quantities of these three monoamines, creates a basic pattern that corresponds to a type of emotional response or behavior, such as “fight or flight”, imprinted in the limbic-amygdala hippocampus section of the mammalian brain (paleocortex), as well as in the subordinate hypothalamic and brainstem centres[13]. Since the phylogenetically ancient monoamines are crucial for behavioral control throughout evolution, these systems give a great advantage for survival because they enable an organism to modify its behavior. Monoamine systems are very dynamic, probably in relation to the need for quite rapid modifications in behaviors and emotion in order to adjust to changes of environment. We can only imagine the huge diversity of situations that monoamine systems had to deal with successfully in order to survive, therefore, a system of behavioral control cannot be specific to every possible situation. It has to activate a number of general emotional and behavioral patterns[14].
The effects of dopamine and serotonin are still not completely understood, because the brain may use a particular neurotransmitter for different purposes in different parts of the body. Some forms of dopamine are related to reward, or more precisely to reward prediction[15], and some forms of serotonin are related to aversion and punishment[16].
In order to better understand the complex relations between the three essential monoamines and the general behavioral and emotional patterns, we will focus on eleven characteristic ratios of these monoamines and try to associate them with certain characteristic emotional states.
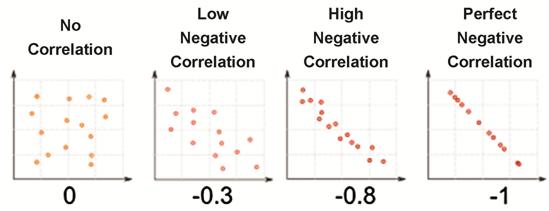
A plasma dopamine and noradrenaline variations research, in response to stress, has shown that both monoamines are not high or low at the same time, so if either one of these two is high in response to stress, the values of the other monoamine are small[17] – high negative correlation has been found.
Negative correlation is a relationship between two variables in which one variable increases as the other decreases, and vice versa[18].
A research on serotonin and dopamine system interactions in the neurobiology of impulsive aggression, has shown that serotonin hypofunction may represent a biochemical trait that predisposes individuals to impulsive aggression, with dopamine hyperfunction[19], so between these two monoamines has also been found negative correlation.
Anatomical and pharmacological data also suggest that serotonin and dopamine may act as mutual opponents[20], meaning in negative correlation.
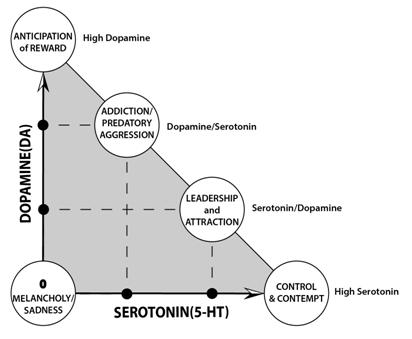
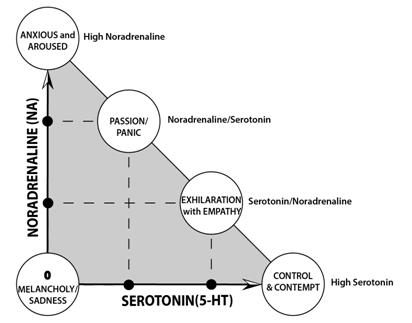
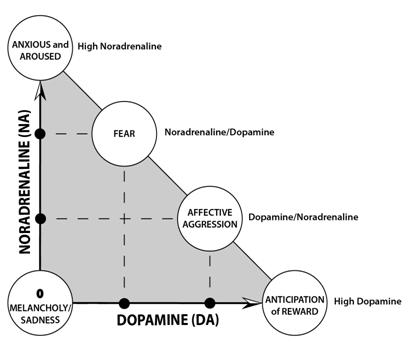
Given the negative correlation between the monoamines, to present it in the theoretical model, we will use the perfect negative correlation of dopamine (DA) and noradrenaline (NA), in an orthogonal coordinate system with two axes, with each end of the arrows represents low and high levels of signaling respectively, with five representative positions marked with circles: zero-point (NA=0; DA=0), high noradrenaline point (NA=1; DA=0), high dopamine point (NA=1; DA=0), noradrenaline/dopamine point (2/3 NA; 1/3 DA) and dopamine/noradrenaline point (1/3 NA; 2/3 DA). Because of this negative correlation the area is triangular instead of square (it would be square in positive correlation). The zero-point and the high points of both monoamines are the three points that define this coordinate system, as the points of low and high signaling. All possible ratios of the two monoamines in negative correlation are inside the gray triangular area marked on the diagram, half of which have predominance of one monoamine over the other and vice versa for the other half. Both circles placed on the negative correlation borderline, between the points of arrows on the two axes, represent the areas where both monoamines are present in a significant percent with one dominating over the other. For illustration of these two states in this theoretical model we have marked with circles the positions with 2/3 of one monoamine and 1/3 of the other – in this example the Noradrenaline/Dopamine point (2/3 NA; 1/3 DA) and the Dopamine/Noradrenaline point (1/3 NA; 2/3 DA) representing all ratios with predominance of noradrenaline over dopamine in former, and vice versa in the later. This is the diagram representing the theoretical model of two monoamines correlation with five typical ratios marked:
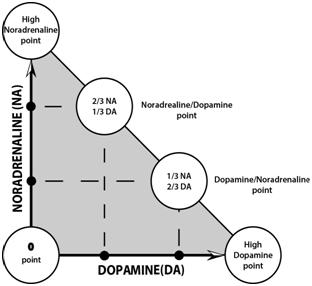
On the following pages we will try to associate each of these typical ratios to a behavioral or emotional state.
In a study of rats that have been conditioned to fight at a specific time each day over a 10-day period, with serotonin levels decreased in the nucleus accumbens, heart rate and dopamine release were concurrently measured and both were raised in anticipation of the fight[21]. This study shows us that lowering of serotonin, raises the other two monoamines, but not in what ratio. Another study of aggressive behaviour shows that when noradrenaline is in excess (i.e., release is stimulated or reuptake is blocked by pharmacologic manipulations) it influences aggression biphasically: a slight activation increases aggression, while a strong activation decreases it[22]. Putting these two studies together may lead us to conclusion that aggressive behavior is connected to low serotonin, high dopamine and moderately elevated noradrenaline, meaning that all three monoamine systems are negatively correlated to each other. Only in a theoretical situations that one monoamine is at minimum, a 2D diagram, such as the previous one presenting a correlation between only two monoamines, has sense.
Much closer to reality, would be to use a 3D model of the all three monoamines in negative correlation. Because of this negative correlation of all three monoamines, the area of the diagram is limited to the tetrahedron presented in the image below, instead of a cubic area of positive correlation.
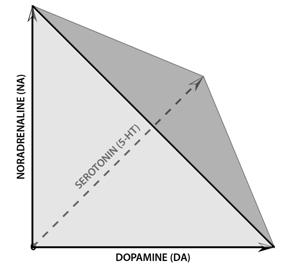
If we mark the five points of typical ratios of each monoamine pair on the three triangular faces which meet at the zero-point corner, of the tetrahedron like 3D model of the all three monoamines in negative correlation, we will get ten marked points of typical ratios on it, since five points are overlapped on the 3D model. We will add to these 10 points one more, the point of highest equal parts of all three monoamines, placed in the center of the fourth triangle tetrahedron – the darker gray one on the previous image, and the following one. This is the Theoretical 3D model of three monoamines correlation with eleven typical ratios of monoamines marked with circles and labeled based on their predominance:
The three monoamines are placed on the three orthogonal axes creating a tetrahedral space, since monoamines are supposed to be mutually orthogonal in a 3D model of monoamines as this maximizes the amount of information that can be transmitted, making it evolutionarily rational[23].
Associating these eleven typical ratios of the three monoamines, is may lead to better understanding of relations between a number of emotional and behavioral states.
Humans, unlike other species, have the sophisticated neocortex, that allows us to learn, at least to certain extent, to voluntarily suppress or modify the somatomotor-behavioural responses, while the autonomic and hormonal expressions cannot be suppressed voluntarily in the same manner. Voluntary suppression or modification of somatomotor-behavioural responses, if often repeated, may even permanently change them if often repeated, disturbing the balance in our physiological systems – “homeostasis”, consequently making changes in organic systems and tissues, including the immune system[24].
The sophisticated psychosocial challenges of today’s modern life may evoke a modified pattern of emotional response, and to understand these partially suppressed emotions and behaviors, we sometimes have to observe the autonomic and hormonal expressions that cannot be suppressed voluntarily.
To truly understand these modifications and suppressions it is necessary learn more about the general, unmodified and unsuppressed, emotional and behavioral states and to connect them to specific ratios of the three monoamines. Thanks to a huge number of studies on monoamine systems conducted through decades, there is an abundance of data available on these issues, and we will use some of these studies to propose the associations between the 11 typical ratios of the three monoamines with emotional and behavioral states.
We will start with the zero-point, as the point of origin.
The zero-point (Low 5-HT; Low NA; Low DA)
The zero-point of orthogonal coordinate system, should be understood as a point where all three monoamines are at the their lowest values, lower then normal basal level, a depressed state in the range from dysthymia to major depression disorder.
Dysthymia form of subthreshold depressive pathology, that may last for decades, neither getting better nor developing a full blown psychological disorder, such as major depression disorder, bipolar disorder etc. Therefore, this state wasn’t conidered to be a pathologycal condition, but a constitutional personality type. In dysthimia(old diagnose was melancholy) a person is in a long-lasting state of gloominess, anhedonia, low drive and energy, low self-esteem and pessimistic outlook[25].
The association between low values of all three monoamines and depression[26], was the leading concept in 1960s, that regains its importance in recent years, with new research on triple monoaminergic reuptake inhibitors (TRIs), as next generation antidepressants[27]. When patients talk about this state, they often associate it with the sensations of darkness, cold and heaviness, feeling sadness, some of the patients start to cry etc. In the homeopathic Repertory, the big Mind rubric we could associate to this state is SADNESS or MELANCHOLY, so we will use this therm for the zero-point.
High Dopamine point (High DA; Low 5-HT; Low NA)
Dopamine is considered to have rewarding, motivating and reinforcing effects, and it is associated with impulsive and addictive behavior.[28] Dopamine system also signals a large class of stimuli that are intrinsically appetitive (e.g., pleasure or sweet)[29], and react to them with the anticipation of appetitive stimuli – reward. The key theme for dopamine could be ANTICIPATION OF REWARD, that may be motivating, cause of addiction and/or impulsive behavior.
Dopamine/ Serotonin point (High DA; Moderate 5-HT; Low NA)
Noradrenergic neurotoxin DSP-4, preceded by zimelidine to prevent serotonin depletion, was administered IP to rats behaving in a defensive-submissive manner in a resident-intruder paradigm, resulting in decrease of frequency and duration of defensive episodes and marked increase of offensive aggression. This might suggest an increase of aggressiveness and therefore support the notion of an inhibitory role of the noradrenergic system in aggressive behavior[30].
As a result of selective lesions of dorsal (DB) noradrenergic (NA) system it was observed that it doesn’t simply decrease noradrenergic metabolism, but also violates its balance with the serotonergic (5-HT) system, because of the lack of noradrenergic tonic excitatory effect on serotoninergic system it decreases[31]. Since both noradernergic and serotonergic systems are lowered in this research the increase in affective aggression may be associated with the dopaminergic system. The increase in aggression is caused by changes in dopamine and serotonin levels, after noradrenaline depletion[32]. OFFENSIVE or predatory AGGRESSION is characterized by planned, goal-directed, emotionless, hidden and not preceded by autonomic arousal[33]. We could also say it is cold in nature, since one of is characteristics is low NA.
Individuals seek out the opportunity to engage in certain aggressive acts, since the performance of aggressive behavior can serve as a potent positive reinforcing event, therefore high dopaminergic.
Study shows that primates with lowered serotonin levels show behaviors similar to type II alcohol abuse: poor impulse control, risky behavior, and consumption of alcohol in huge amounts[34], while another study finds that high dopamine levels have been observed in some populations of substance users such as type II alcoholics[35] – leading to conclussion that type II alcoholic addiction could be associated with this dopamine/serotonin point. Cocaine, unlike MDMA, shows consistent rewarding effects, due to the high dopamine level – significantly contributing to cocaine addiction. The other two monoamines are moderately elevated, so the cocaine abuse may be placed close to this point. It may be placed here also because a study of repeated low-dose cocaine treatment (0.5 mg/kg/day) during adolescence facilitates offensive aggression in male Syrian hamsters, while treatment with fluoxetine (SSRI), resulting in elevated serotonin, inhibited the cocaine-facilitated aggressive response[36].
Therefore, we may associate this point with ADDICTION and OFFENSIVE AGGRESSION.
Serotonin/Dopamine point (High 5-HT; Moderate DA; Low NA)
The dopaminergic system together with oxytocin and vasopressin are crucial in the formation of pair-bonds[37], and dopamine reward system makes love a rewarding experience[38]. Infusions of moderate doses of dopamine into the nucleus accumbens facilitate pair-bonding, whereas infusion of high doses does not generate this effect. Love can feel like an addiction, and the dopaminergic pathways that are involved in love and pair-bond formation are largely similar to those that are involved in addictive behavior[39]. Since it is suggested that serotonin and dopamine act as mutual opponents[40], we may assume that lower dopamine levels result in higher serotonin levels.
Parkinson’s disease (PD) is a degenerative disorder of the central nervous system related to loss of dopamine-generating cells, and consequent low dopamine levels, and again we may assume that in turn serotonin levels may be elevated[41]. Study has shown that young Parkinson’s disease (PD) patients, with early disease onset, have significantly higher incidence of hypomania and mania related to dopamine replacement therapy (DRT)[42], so in these cases to assumingly already elevated serotonin levels, dopamine levels are also increased. Therefore, we are going to associate hypomanic behavior with this point.
A hypomanic person is described as cheerful, optimistic, extroverted, self-confident, energetic and needing habitually less sleep than other people. They can also be irritable, rude, reckless and irresponsible[43]. Hypomanic people are also focused, productive and generally successful at work, Hypomania may be an evolutionary advantage, since hypomanic behavior is generally perceived as being energetic, euphoric, visionary, overflowing with new ideas, and sometimes overconfident and very charismatic, but coherent enough in thought and action to participate in everyday activities[44]. Therefore, a hypomanic person will rarely think of changing this state – going to treatment of this condition. Low dopamine levels have been found to contribute drug- and alcohol-seeking behavior[45], so basically attracted to addictive behavior, while the next point whit inverse serotonin/ dopamin ratio, is associated with addictions.
Since moderate doses of dopamine facilitate pair-bonding, so we may call this one the point of LEADERSHIP AND ATTRACTION.
Serotonin/Noradrenaline point (High 5-HT; Moderate NA; Low DA)
Very close to serotonin/noradrenaline point may be placed abused psychostimulant MDMA (Ectasy), has affinity for serotonin (5-HT), noradrenaline (NE) and dopamine (DA) transporters ( SERT, NET and DAT respectively)[46], but predominantly for SERT with 10-fold higher affinity at SERT compared to DAT, leading to lower rewarding strength, and consequently addictive, effect compared to cocaine, for example.
MDMA abuse is associated with euphoria, exhilaration, an increased perception and feeling of closeness to others – emapthy, mood-enhancement, increased energy and heightened senses, but also hyperthermia that, esspecially in warm environments may develop acute complications with potential fatal consequences, as well as tachycardia, hypertension, seizures etc.[47],[48] Most frequent acute somatic complaints of MDMA were jaw clenching, lack of appetite, impaired gait, and restless legs[49]. It affects mnemonic processes including spatial, working and episodic memory domains, but without affecting simpler aspects such as vigilance, reaction time, selective attention, and response inhibition. MDMA affecting response inhibition may be connected to serotoninergic inhibitory effect, while high dopaminergic effect of impulsiveness is found in cocaine impaired performance on response inhibition[50].
Single low dose of MDMA produces cognitive impairments lasting up to 72 h post-administration, whereas acute low doses of cocaine produced cognitive enhancement[51].
Although it was expected that drugs of abuse that increase sleepiness and sedation (e.g., cannabis) are more likely to induce dissociative symptoms than stimulant drugs (e.g., MDMA, cocaine), a study has demonstrated that MDMA and cannabis can induce dissociative symptoms, unlike cocaine. While cannabis significantly increased subjective ratings of depersonalization, derealization, and amnesia during intoxication, and MDMA primarily increased feelings of derealization, their magnitude of total dissociation was comparable[52].
Exhilaration with EMPATHY could be the most adequate terms to describe this behavioral state.
Noradrenaline/Serotonin point (High NA; Moderate 5-HT; Low DA)
In early stages of romantic love, there is a depletion of serotonin levels[53],[54].
In the classical experiment by Dutton and Aron the influence of an elevated noradrenergic state on the sexual attraction was shown, when the sexual attraction to an attractive interviewer was increased by locating the interview on a anxiety-arousing, high suspension bridge, as compared to a low bridge[55].
Depletion of central serotonin is also found in obsessive-compulsive disorder (OCD)[56]. Early stages of romantic love show similarities to OCD, like a mild serotonin-depletion-related form of obsessive behavior, including symptoms of anxiety, stress, and obtrusive thinking. Of course love is not a mental disorder, so 12–18 months after the start of the relationship, subjects do not have any obsessive ideation regarding the partner anymore[57]. The high levels of anxiety and stress indicates high noradrenaline content, so the obsessive component maybe related to serotonin.
Another study has shown significant correlation between increased anxiety severity and decreased DAT availability in newly diagnosed, untreated PD patients[58], that may also indicate negative correlation between the three monoamines, by finding behavior associated with elevation of noradrenaline and serotonin as a result of lowering dopamine levels.
Serotonin agonists (5-MeODMT) raise pain thresholds dramatically, as well as very markedly facilitate male rat sexual behavior (male rats require fewer intromissions to reach ejaculatory threshold), but degeneration of central noradrenergic (NA) neurons by DSP4 abolished entirely the analgesic effect and most of the effects on male rats sexual behavior, of 5-MeODMT or serotonin (5-HT) itself [59],[60]. So, high serotonin levels loses both of these effects, without a moderate action of noradrenaline.
Since there is evidence to support association between low dopamine activity and social phobia, and increased dopamine transporter binding in generalized social anxiety disorder, making these conditions low dopaminergic, while high doses of caffeine with elevating noradrenergic effect might provoke panic attacks in patients with panic disorder or social phobia, and noradrenergic β-blockers are sometimes used to treat uncomplicated performance anxiety, so this might support that social anxiety/panic state is high-noradrenergic[61]. There is an increased serotonin transponder binding in generalized social anxiety disorder, therefor a lowered serotonine level[62], but since there are low dopamine levels in these conditions if we take into consideration the previosly mentioned negative correlation between serotonin and dopamine, the level of serotonin will be higher then dopamine levels, so we could say that we will have moderate serotonin level.
We could say this is the point of PASSIONATE, but also social anxiety/PANIC behavior.
High Serotonin point (High 5-HT; Low NA; Low DA)
In the previous study the serotonin component was linked to obsessive behavior, and also serotonin 5-HT2A receptor polymorphism has recently been linked to an obsessive romantic attachment behavior[63]. If there is a purpose to the obsessive behavior in OCD it is to avoid some potential or imaginary danger. Serotonin system signals a large class of stimuli that are intrinsically aversive (e.g., stress or pain)[64], and reacts to these stimuli with repulsion and withdrawal. Serotonin leads to behavior inhibition and aversion to punishment[65]. We may say that the key theme of serotonin could be avoiding danger, regulating the other two monoamines by inhibitory mechnisms, in other words CONTROL the system. Also, another study showed that systemic administration of the selective dopamine D2 receptor antagonist sulpiride caused proaversive effects in rats in the elevated plus maze[66], and since lowering dopamine may lead to elevated serotonin, this study also leads us to assumption of association between elevated serotonin and (pro)aversive behavior . Serotonin also has a well established anti-depressive effect, illustrated by the fact that serotonin synthesis in normal male was found to be 52% higher than in normal female, which might explain the lower incidence of major unipolar depression in males[67].It is also associated with nausea, and feeling disgust and CONTEMPT.
Dopamine/Noradrenaline point (High DA; Moderate NA; Low 5-HT)
The study described before, when we were giving an explanation on the 2D diagram of dopamine/noradrenaline relation, this point was associated with the emotional aggression as emotional response.
Another study of the aggressive biting response effects, on stress-induced noradrenaline (NA) release in the rat amygdala and gastric ulcer formation, one group of rats were exposed to a 60-min period of cold restraint stress with or without being allowed to bite a wooden stick[68]. The results have shown that the group allowed to bite a wooden stick had approximately doubled the noradrenaline (NA) release, and it returned to basal levels immediately after release from stress, while in the other group the noradrenaline level has approximately tripled, and it was maintained until 80 min after release from stress. This suggests the possibility that expression of aggression during stress exposure might attenuate stress-induced fear and/or anxiety – a rewarding effect probably connected to high dopamine levels. In this example we can once again find that the medium elevated noradrenaline (NA), with low serotonin and high dopamine is present in expressed AFFECTIVE AGGRESSION. Affective aggression is impulsive, overt and unplanned in nature, equivalent to defensive rage[69]. Impulsive alcoholic offenders show lower CSF 5-HIAA than non-impulsive alcoholic offenders and healthy controls[70] (Virkkunen et al., 1994), indicating that the impulsive type of aggression is associated with serotonin hypofunction[71]. High dopamine levels have also been observed in some populations of substance users such as type II alcoholics, a group associated with impulsive and aggressive behavior[72].
Noradrenaline/Dopamine point (High NA; Moderate DA; Low 5-HT)
The non-bitting group in the previous study had approximately tripled the basal noradrenaline (NA) release – a clearly high NA level[73]. Stress-induced increases in NA turnover in the amygdala are closely related to the provocation of negative emotion such as anxiety and/or fear observed in animals during stress exposure[74],[75], so we may connect this point to FEAR, since fear also has a rewarding dopamine component – its one of the reasons why people enjoy horror movies. Fear can be characterized by arousal, noradrenergic effect, and fight-or-flight responses to imminent threats[76]. Analysis of the gastric ulcer data indicated that the biting rats had significantly fewer and smaller lesions, up to five times, as compared to the non-biting rats. These results strongly support the hypothesis that suppression of aggression during stress exposure may lead to psychosomatic diseases such as peptic ulcer and/or neuroses in humans. FEAR is also a big rubric in the Mind section of the Repertory.
High Noradrenaline point (High NA; Low DA; Low 5-HT)
In the same study, the above mentioned stress-induced increases in NA turnover in the amygdala is closely related to negative emotion of anxiety, an unrewarding, hence low dopaminergic and low self-esteem, hence low serotonegic emotion. Central serotonin depletion is found in anxiety disorder[77]. Thus we may connect this point to ANXIOUS and AROUSED. The high noradrenaline levels are also connected to active, aroused, high pulse and blood pressure, attentive[78]. Anxiety is characterized more by apprehension, tension, and worry, where the potential threat might occur in the distant future[79]. ANXIETY is also a big rubric in the mind section of the Repertory – another reason to use this therm high noradrenaline point.
The point of equilibrium (Moderate 5-HT, DA and NA)
There is anther point in the middle between the high points of all three monoamines, the point of equilibrium, a more or less neutral state, but heightened, as opposed to lowered neutral state of dysthymia, until about a century ago diagnosed as melancholy and the lowest neutral zero-point, basically of a depressed state – sadness. This high point of equilibrium is quite often described by our patients with the sensation of light, warmth and lightness, image of a beautiful sunny day, feeling of peace and tranquility. This is the point of balance and inner PEACE & JOY.
Each point represents a behavioral state of a person, depending on the underlying relational pattern of the three monoamine, while their positions in the 3D model reveals the relations between them. This model shows the pattern – the MATRIX of behavioral stated, in order to help us understand why do the behavioral changes of a certain type of person occur in a particular sequence:
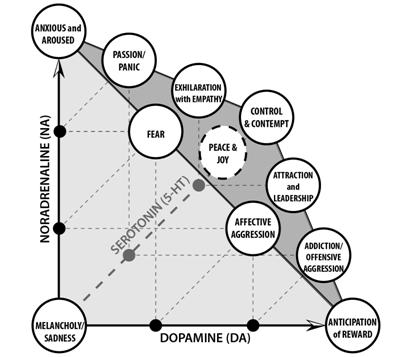
Since all the points except the zero-point, are placed in the same triangular plane with the point of each axis arrow, at the corners of the triangle. To flatten the 3D MATRIX of behavioral states, into this one triangular plane we will superimpose the two points of equal parts of all three monoamines – the zero point of low equilibrium (depression), and the point of equilibrium (peace & joy), in to one point, represented with black and white half.
This flattened MATRIX model of behavioral states has a triangular shape with 10 points marked with behavioral states looks very much like the ancient Pythagorean symbol tetractys, so we have named this 2D model of behavioral states the TETRACTYS model. This TETRACTYS model might be easier to follow then the 3D model, for everyday use in homeopathic practice together with the Chain of emotions:
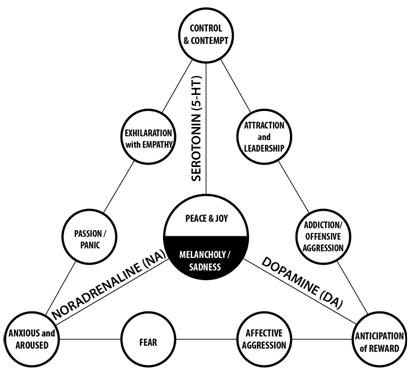
These states represent typical behavioral states, while a person in real life will usually somewhere in-between, but gravitating to one of them at any given time. We have chosen one therm for each of these states, but, for example, elevated Dopamine is not just about anticipation – it is also about rewarding feeling, motivation, addiction, impulsiveness etc. We have asked ourself, what is in common for all these themes, and why?
These are all behavioral patterns shaped through the evolution. Every human being has conscious and unconscious goals, at least the survival as the deepest instinctive goal. When a goal is pursued every moment is charged with ANTICIPATION of REWARD, making you motivated, but also reckless and impulsive. It seems to us that by creating a feeling of ANTICIPATION about a goal dopamine affects our behavior, so we have chosen these terms.
In order to survive, apart from goal pursuit, you need to avoid danger, and to be vigilant most of the time. In order to avoid danger one has to anticipate risks, stop risky behavior and plan ahead, in other words to CONTROL, accompanied by feelings of CONTEMPT, strength and high self esteem. Similarly, staying vigilante most of the time may lead to the state of ANXIETY.
Feeling of inner weakness, with feeling threatened or under pressure, is shared by all four low serotonin states and the zero-point of depression. Feeling of inner strength and self-confidence gets higher with elevated serotonin content, with its high at high serotonin point (the superior feeling of contempt and disgust to others, an extreme state connected to satiety [80] – in the food related disgust, if a person keeps eating after there is no more hunger, it will lead to the point of food aversion. Connection of this feeling to serotonin is well established since in allopathy the nausea and vomiting are often treated with antagonists of the serotonin receptor type 3[81]). States of fear and affective aggression are considered both low serotonergic, but on the other hand, as all the other states with elevated dopamine share the feeling of reinforcement and reward. States of elevated noradrenaline are supposedly active and aroused, attentive, with a high pulse, feeling heat, may be even with reddish face[82], but not focused to either avoid or achieve something, therefore with an element of uncertainty that may lead to anxiety .
Most people go through some form of all of these behavioral states, but every person is more prone to get in a few of these states over and over again throughout life – a disposition to a certain kind of behavior. Aggression is one of the most researched behaviors because of its impact on society. It is a behavioral pattern with a crucial evolutionary role, so finding a genotype associated with it was a logical step. Low functioning MAOA genotypes have been reliably linked to increased reactive aggression, with increased impulsivity, specific to conditions of negative affect, as a key element of this behavioral pattern. Study suggests that disrupted serotonergic systems, thus limited in its inhibitory actions, in MAOA genotype predispose individuals towards aggressive behavior by increasing impulsive reactivity to negative affect[83]. Impulsivity in the MAOA genotype, is a trait of a high dopaminergic activity, and in our model both states near the high dopaminergic corner, are associated with aggression (one with offensive and the other with affective aggression).
Just as MAOA genotype may be associated with predominance of dopamine, due to disrupted serotonergic system, other genotypes may be associated with high activity of the other two monoamines (noradrenaline and serotonin), resulting in three general types of disposition.
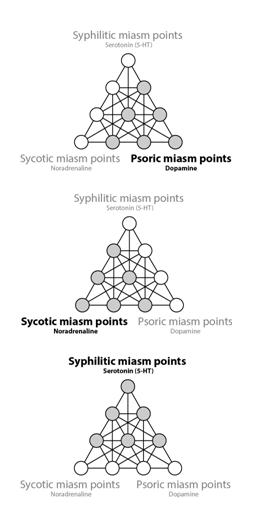
In homeopathy, Hahnemann has defined the three genaral dispositions, the three miasms – Psora, Sycosis and Syphilis. Genotypes with predominance of serotonin could be associated to the Syphilistic miasm, due to incredibly similarity with the hypomanic type of behavior that is placed in the Serotonin/Dopamine point near the High serotonin point of our flattened MATRIX of behavioral states. Dopaminergic anticipation and motivation could be associated with Psora as a driving force behind the never ending psoric struggle, while anxiety and fears of the on and near the high noradrenergic point may be associated with fears and hiding of Sycosis.
This leads to the conclusion that the three Hahnemann’s miasms are the three general miasms, three general patterns of behavior, well founded in the effects bio-dynamcs of the three monoamines on behavior.
In the study of the aggressive biting response effects, on stress-induced noradrenaline (NA) release in the rat amygdala and gastric ulcer formation[84], mentioned above, a significant correlation has been found between the monoamines state and higher incidence of gastric lesions (up to 5 times higher).
Since the homeopathic miasms affects the mental emotional and physical level, this example of mental/emotional and physical correlation of monoamines action speaks in favor of the three monoamine – three miasm correlation.
When each content from Chain of contents is associated with one of the behavioral and emotional states in our TETRACTYS model of behavioral states, depending on area of the model where most contents are positioned we may define the patients miasm. We will demonstrate this later in the examples of case analysis using the MATRIX method.
Every patient will have one predominant miasm, but usually with elements of one or both of the other two miasms. If we observe the dominant miasm with elements of one of the other two as a separete subtype of miasm, we may find six more subtypes and one more theoretical subtype that has elements of all three myasms, so the model of three miasms doesn’t exclude additional six/seven subtypes, or even defining each behavioral state on our flattened MATRIX of behavioral states model as a separate miasm. On the other hand by defining each variation as a separate miasm would cloud the similarities between these subtypes, and the real-life dynamism between these states.
By associating the states on our TETRACTYS model, with the emotional and behavioral states behind the contents a homeopathic patient is going through during the case taking and in the Chain of contents, we may follow the dynamic, sequence and paths of his/hers changes in behavioral states. Usually a patient will go through just a few behavioral states, while talking of all kinds of things in case taking and in the Chain of contents. These few behavioral states a patient is going through, create together his/her personal pattern similar to a pattern of that patients constitutional homeopathic remedy – Simillimum. This pattern on the TETRACTYS model is the TETRACTYS of a patient.
Based on the positions of the points of general behavioral states on the Tetractys of a case, we may recognize the miasm of that patient, as it is presented on the diagrams below:
After this lengthy, but necessary explanation we will give an example, of an Arg-n case mentioned in an earlier article on Tetractys of Simillimum by Dr M. Zivanov, but this time in detail through all steps of the Matrix method.
Example of the first step of the Matrix method – the Deep PEAT techique
Arg-n Case, Woman, 34 years old, Teacher
The procedure of Deep PEAT is quite simple to learn. It begins with discussion with the patient in order to define the starting point of a process. For a homeopath this step is unnecessary since the patients main complaint is usually pointed out by a patient at the beginning of the classical homeopathic case taking. Deep PEAT is a psychological technique, so the starting point has to be the way a patient feels about his/her main complaint.
In the next step this staring point – “problem” has to be defined briefly in the words of the patient, because only a persons own words are powerful and meaningful enough to provoke a reaction of the subconscious.
The technique starts at the “I-point”, on sternum, where the patient holds the index finger and the middle finger, and embracing the feeling of acceptance and love for yourself and your “problem” as a part of you, while making the FAM statement with regard to the starting “problem”:
“Even though I feel _________(“problem” – the statement of complaint), I accept and love myself, my body, my personality and _________ (“problem”)”
After that the patient should take a deep breath, exhale, and move the two fingers to the point in the inner corner of the eye – the “first-point”, “insight point”. Here the patient should imagine himself/herself in situation that results in the “problem” as intensely and deeply as he/she can – the imaginal exposure, then take a deep breath, exhale and report his/her experience. If the content does not change the patient moves the next, second, point around the eye, takes a deep breath, exhales and again imagines the “problem” situation and intensifies it as much as possible. If the content doesn’t change again, the patient moves to the next, third, point around the eye, and if it still doesn’t change, back to the first “insight-point”, and so on until it does.
When a new material arises the patient moves back to the chest “I-point” and repeats the Formula of Antagonistic Motivation (FAM)with the acceptance of that content, followed by taking a deep breath and exhaling.
Whenever there is a change, the patient goes the “I-Point” and “dives deeper”. It is important to carefully listen to each new content that arises, and when the patient states to opposite contents, he/she is directed to the “I-Point” to make the FAM statement, regarding each opposite separately, then taking deep breath and exhaling, and move the two fingers to the First point, “Insight-point”.
At the “Insight-point” the patient first has to imagine and intensify the feeling of one opposite, take a deep breath and exhale, then he/she is told: “now forget about ______(the first opposite)”. Then the patient is instructed to imagine and intensify the feeling of the other opposite, take a deep breath and exhale, and after that to imagine both simultaneously, followed by taking a deep breath and exhaling,
Than the patient is told: “Now tell me, without using logic and reasoning, do you fell that you can feel this opposites separately”, If the answer is “no” this pair of opposites are the Primes, and they have been neutralized. It is the end of the process, for the needs of a homeopath[85].
For example, here is an Argentum nitricum case, with fear of being alone as the main complaint:
Dr: We should start with some issue that bothers you the most.
P: Well, its that fear. I want to feel independent. To get rid of that fear.
Dr: So, the starting complaint is “fear”. Now close your eyes, lightly touch the “I-Point”, with first two fingers of your right hand and repeat after me:
Even though I feel fear, I accept and love myself, my body, my personality and that I feel fear. (the patient is repeating FAM after the homeopath)
Take a deep breath and exhale.
Now lightly touch the “First-point” and imagine feeling that fear, a situation were you’ve felt that kind of fear and dramatize it.
Say the first thing that comes to your mind.
P: [content: “fear”; “First-point”]
I feel enclosed, like someone is walling me in from all sides (she is gesturing with her hands like showing sides of a box )
Dr: Take a deep breath and exhale.
Lightly touch the “I-Point” and repeat after me:
Even though I feel enclosed, I accept and love myself, my body, my personality and that I feel enclosed. (the patient is repeating FAM after the homeopath)
Take a deep breath and exhale.
Now lightly touch the “First-point” and imagine feeling enclosed, and dramatize it.
P: [content: “enclosed”; “First-point”]
I feel something here (showing the back of her neck, more to the left), like a tingling, like I’m not in control of my muscles.
Since this tingling is a localized sensation, just like the next one, the stomach pain, we are moving on to the next point around the eye – waiting for a content that is a feeling or a general sensation, and only then starts the new cycle at the “I-point”.
Dr: Take a deep breath and exhale.
Lightly touch the “Second-point” outside the eye, and imagine feeling enclosed, and dramatize it.
P: [content: “enclosed”; “Second-point”]
Is it possible that I’ve just felt pain in my stomach, like slight burning.
Dr: Take a deep breath and exhale.
Lightly touch the “Third-point”, under the eye, and imagine feeling enclosed, and dramatize it.
P: [content: “enclosed”; “Third-point”]
I can’t concentrate on that feeling anymore. Now I don’t feel anything and I feel calmer.
Dr: If you can’t feel that anymore it’s good, because one of the purposes of the process is to relief the charges on the issues.
Take a deep breath and exhale.
Now lightly touch the “First-point” and imagine feeling enclosed, and dramatize it.
P: [content: “enclosed”; “First-point”]
I feel sad (starts crying).
Dr: Take a deep breath and exhale.
Lightly touch the “I-Point” and repeat after me:
Even though I feel sad, I accept and love myself, my body, my personality and that I feel sad. (the patient is repeating FAM after the homeopath)
Take a deep breath and exhale.
Now lightly touch the “First-point” and imagine feeling sad, and dramatize it.
P: [content: “sad”; “First-point”]
That’s it. I can’t dramatize it anymore than that. I am thinking how I feel ashamed now.
From this point on, we are going to skip the guidance by a homeopath, because these are the same sentences repeated in each cycle, with a few words changed, namely the content that surfaced at the end of the previous cycle. It will make following the chain of contents easier.
P: [content: “ashamed”; “First-point”]
I feel hot. I am sweating. I can feel anything else at the moment.
P: [content: “hot”; “First-point”]
I don’t know. I can’t. It is like I am blocked and I can’t cooperate. At first I have opened up, but since I’ve started to cry, I closed myself in and it is very hard for me to continue. I guess it is because I don’t feel anything right now, so I have nothing to say.
P: [content: “closed myself in”; “First-point”]
I am tensed.
P: [content: “tensed”; “First-point”]
I feel much more peaceful now.
Dr: What is the opposite of feeling peaceful, for you?
P: Fear is opposite.
Dr: How do you feel when you are afraid?
P: Powerless.
P: [content: “powerless”; “First-point”]
At the moment I can’t imagine feeling powerless, or a situation where I would feel powerless. Right now I feel bright and capable.
P: [content: “bright”; “First-point”]
Me in the countryside, walking and feeling cheerful.
P: [content: “bright”; “Second-point”]
I imagine myself going for a walk, traveling, shopping, how I can do everything on my own and to be able to spend a day all by myself. I can’t do it in real life because of that fear.
P: [content: “bright”; “Third-point”]
I still imagine the same image, me walking through the city, but now I start criticizing myself because that is how I imagine feeling bright. I started thinking of studying and work. At the previous point I’ve felt free, and now I blame myself.
P: [content: “blaming myself”; “First-point”]
Now I could start crying again, but I wont. I am starting to feel sad again, but it is more like I pity (smiling) myself.
P: [content: “self-pity”; “First-point”]
Well, I don’t know. It’s a miserable thing to say that I feel self-pity.
P: [content: “self-pity”; “Second-point”]
It’s like, everything is bright and clear to me now. Like I’ve unwrapped some stuff. I feel much lighter, as if a burden’s been lifted.
P: [content: “self-pity”; “Third-point”]
I feel better now. Much clearer, like I can organize my thoughts well and I clearly see myself. I feel much stronger.
P: [content: “strong”; “First-point”]
I am thinking now: “i feel so strong i could explode”
P: [content: “strong”; “Second-point”]
Again, some fear started to appear because I feel too strong. I used to have that feeling before, like when I’m feeling good I start to be afraid because I feel good – as if it’s too much for me.
P: [content: “fear of too much”; “First-point”]
Now that I’m think about the words “too much”, I remember the last period I was going out with my friends, the drinking, sex. It felt good.
P: [content: “fear of too much”; “Second-point”]
Now I remember the guilt I felt the morning after, because back then, it was very hard for me to convince myself that was OK to drink too much, and find my peace again.
P: [content: “peace”; “First-point”]
I feel peaceful now.
Dr: What is the opposite of peace for you?
P: Anxiety.
Dr: Take a deep breath and exhale.
Lightly touch the “I-Point” and repeat after me:
Even though I feel peace on one side and anxiety on the other, I accept and love myself, my body, my personality and that I feel peace on one side and anxiety on the other. (the patient is repeating after the homeopath)
Take a deep breath and exhale.
Now lightly touch the “First-point” and imagine feeling peace.
Now forget about feeling peace.
Now imagine anxiety.
Imagine peace and anxiety at the same time.
Take a deep breath and exhale. You may open your eyes when you are ready.
There are two ways we may understand the precesses in the Deep PEAT technique – one is classical psychological explanation and the other is from the holistic perspective, based on energy paradigm – energy therapies.
The first classical explanation of the technique, fundamentally based on the mechanistic concept of a human being, is that after defining a “problem”, follows the phase of the imaginal exposure with light pressure on a point, not necessarily on a meridian, followed by distraction in a form of FAM with light pressure on sternum, and back again to the previous step of imaginal exposure. These steps are repeated until desensitization of a “problem”, the third part and the goal of this treatment, is achieved.
The other explanation is based on the application of energy paradigm to removal of psychological and emotional aberrations, believed to be caused by disturbances in the energy field of a human being. These disturbances manifest themselves neurologically, biochemically, cognitive and behaviorally, while their energy foundation exists and acts on the deepest level of energy structures and fields.
The second step of the Matrix method – the Tetractys of a patient
The patient has chosen the following issue for the starting point in Deep PEAT:
“Well, its that fear. I want to feel independent. To get rid of that fear.”
Therefor, we will use the word “fear” for the starting point.
This is the same case we have used to illustrate the Deep PEAT technique, but here we will analyze it in the context of the Matrix method, and Tetractys of Simillimum. We will simplify the layout of this case, and the cases we are going to present in the following chapters, so every content that goes to the I-point is going to be marked by a number, while the points around the eye are marked with dashes.
Based on the data presented in the chapter “The Matrix of Miasms Model” we will try to associate each content we get in the Deep PEAT process, to a general behavioral of emotional state in the Tetractys of Simillimum – points of Tetracys and we will mark them by using bold condensed typeface. We will also explain our decisions about associating a content to a point of behavioral or emotional state, and our explanations will be marked by using italic typeface.
- Fear (Fear point)
– I feel enclosed, like someone is walling me in from all sides (she is gesturing with her hands like showing sides of a box )
- Enclosed feeling (Passion/Panic point) The contents that follow the
starting point, the enclosed feeling, pain in the stomach and tingling
may associated to the panic, because the enclosed feeling, feeling
trapped, is often accompanied by fear and overwhelming panic
followed by sensation heat, that we may recognize in the burning
pain in the stomach. Until the moment when a patient says
that she starts feeling calmer we may assume that she is in the same
general behavioral or emotional state, so all the contents before the
change of state will be listed under the previous state, in this case
the of Passion/Panic point Tetractys model.
– I feel something here (showing the back of her neck, more to
the left), like a tingling, like I’m not in control of my muscles.
– Is it possible that I’ve just felt pain in my stomach, like slight
burning.
– I can’t concentrate on that feeling anymore. Now I don’t feel
anything and I feel calmer.
A person may get calmer either because has reached the
state of high energy equilibrium, Peace & Joy point, or
because the energy has decreased towards the zero-point,
Melancholy / sadness point – both states in a way stabilize an
acute stressful situation. In this case we can see that the
patient has calmed down towards the zero-point, because
the following content is “sadness”.
– I feel sad (starts crying). (Melancholy / sadness point)
- Sad
– That’s it. I can’t dramatize it anymore than that. I am
thinking how I feel ashamed now.
- Ashamed (Passion/Panic point) We can see a change back to this state
again, because the patient says that there are no more contents left
at the Melancholy / sadness point and the new state is described by
feeling ashamed, hot and sweating. Sensations of heat and sweating
onset of panic attack with the elevated NA and 5-HT Passion/Panic
point and feeling ashamed is also connected to blushing, heat and
sweating, a passive reaction low dopamine reaction.
– I feel hot. I am sweating. I can feel anything else at the moment.
- Hot
– I don’t know. I can’t. It is like I am blocked and I can’t
cooperate. At first I have opened up, but since I’ve started to
cry, I closed myself in and it is very hard for me to continue.
I guess it is because I don’t feel anything right now, so I have
nothing to say.
- I closed myself in
– I am tensed. (Fear point) Feeling tensed is connected to
DA anticipation, speaking in favor of the state of fear.
- Tensed
– I feel much more peaceful now. (Peace & Joy point)
The patient has reached the state of high energy
equilibrium, and even our following two questions couldn’t
change this state, so she can’t even describe an imaginary
powerless feeling while in this state. She further describes
this state as feeling bright and capable.
What is the opposite of feeling peaceful, for you?
Fear is opposite.
How do you feel when you are afraid?
Powerless
- Powerless
– At the moment I can’t imagine feeling powerless, or a
situation where I would feel powerless. Right now I feel
bright and capable.
- Bright
– Me in the countryside, walking and feeling cheerful.
– I imagine myself going for a walk, traveling, shopping, how
I can do everything on my own and to be able to spend a day
all by myself. I can’t do it in real life because of that fear.
– I still imagine the same image, me walking through the city,
but now I start criticizing myself because that is how I
imagine feeling bright. I started thinking of studying and
work. At the previous point I’ve felt free, and now I blame
myself. (Melancholy / sadness point) The patient start to get into
a gloomy, low energy mood, blaming and pitting herself,
almost starting to cry again – the zero-point.
- Blaming myself
– Now I could start crying again, but I wont. I am starting to
feel sad again, but it is more like I pity (smiling) myself.
- Self-pity
– Well, I don’t know. It’s a miserable thing to say that I feel
self-pity.
– It’s like, everything is bright and clear to me now. Like I’ve
unwrapped some stuff. I feel much lighter, as if a burden’s
been lifted. (Peace & Joy point) Apart from the previously used
word “bright”, this state is now also described with words
“clear”, “light”, in contrast to the previous state of
melancholy-sadness that has been a burden – heavy, hard.
– I feel better now. Much clearer, like I can organize my
thoughts well and I clearly see myself. I feel much stronger.
- Strong
– I am thinking now: “i feel so strong i could explode”
(Exhilaration with Empathy point) High serotonergic and
noradrenergic point, a very high energy point, with feeling
there is too much of something that may be associated to
serotonin (nausea, disgust). This point is also associated to
friendship and empathy, but this state lasted just for a
moment because it is more like remembering a state she used
to have in the past.
– Again, some fear started to appear because I feel too strong.
I used to have that feeling before, like when I’m feeling good
I start to be afraid because I feel good – as if it’s too much for
- (Fear point)
- Fear of too much
– Now that I’m think about the words “too much”, I
remember the last period I was going out with my friends,
the drinking, sex. It felt good. (Exhilaration with Empathy point)
Once again this is a reminiscence of a state she used to have.
– Now I remember the guilt I felt the morning after, because
back then, it was very hard for me to convince myself that
was OK to drink too much, and find my peace again.
- Peace
– I feel peaceful now. (Peace & Joy point)
The “peaceful” feeling was repeated a number of times during
the process, and once again in the previous content, so we have
assumed that this is the key theme for the patient, so we ask
the patient about the opposite of this content.
What is the opposite of peace for you?
Anxiety
Since the patient has stayed in the point of high energy
equilibrium – the point of peace & joy, after uniting these
two opposites, we may assume that the deepest pair of
opposites, the Primes, for this patient are:
PEACE – ANXIETY
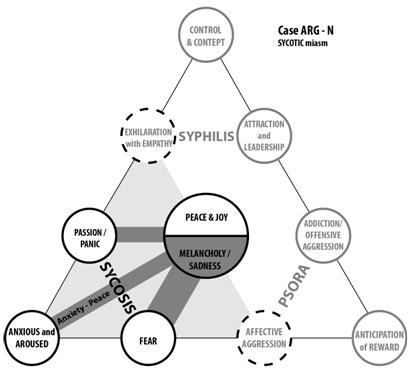
The Simillimum for this patient was Argentum nitricum, so we may also assume that the patient’s contents in the: Fear point, Passion/Panic point, Anxious – aroused point, Melancholy – Sadness point, and Peace & Joy point together with the Primes – Peace-Anxiety, are the key elements of this remedy’s Tetractys of Simillimum. Exhilaration with Empathy point is a state the patient remembers, while now she may get into that state just for a moment at best, so we will mark this state with a dashed line as a potential state that she presently doesn’t have.
The following contents were associated with the six points of Tetractys in this case:
Fear point: – Fear
– Tensed
– Too much
Passion/Panic point: – Enclosed feeling
– Tingling
– Pain in the stomach, slightly burning
Passion/Panic point(continued): – Powerless
– Ashamed
– Hot
– Sweating
Anxious – aroused point: – Anxiety
Melancholy – Sadness point: – Sad (crying)
– Self-Blame
– Self-Pitty
– Guilt
– Miserable
Peace & Joy point: – Bright
– Capable
– Cheerful
– Clear
– Light
– Peaceful
(Exhilaration/Empathy point): – Feeling so strong I could explode
– Able to organize my thoughts
– Going out with friends (drinking, sex)
– Feeling good
The case started with the theme of fear, Fear point, followed by Passion/Panic point and after a short lowering of the patient’s energy to the Melancholy – sadness point she gets back to the Passion/Panic point and followed by the Peace & Joy point of high energy equilibrium. After that the energy level has decreased to the Melancholy – sadness point, but just for the next few contents, and then back to the Peace & Joy point followed by the energy rise to the Exhilaration/Empathy point. This was immediately replaced by a state of fear, Fear point, of the previous exhilarated state, so we may assume that the patient used to have this state in the past, and it may appear again in the future but right now it is not one of her general behavioral states. After the Fear point the patient once again reminiscences of her exhilarated state in the past, followed by the peaceful feeling of Peace & Joy point, that continued after uniting the Primes. The opposite of content to “peace” was “anxiety” so this adds the Anxious – aroused point as well.
When we look at the positions of these five points on our Tetractys model, two of them are in the middle – the zero point (Melancholy – sadness point) and the point of high energy equilibrium (Peace & Joy point), while the other three (Fear point, Passion/Panic point and Anxious – aroused point) are in the Sycotic miasm corner, and since the Exhilaration/Empathy point belongs to the patient’s past, we will mark it with dashed line as a potential state she may get into.
For finding the patient’s miasm we need to put aside the zero-point and the point of high energy equilibrium, because both are present in all three miasms. In this case, after removing these two, we are left with the three points in the sycotic corner – the Fear point, Passion/Panic point and Anxious – aroused point, therefor patient’s miasm is Sycotic, while in the past she also had a syphilitic component when she was getting into the state of Exhilaration/Empathy point .
The points and the miasm present in this case are presented in black on the diagram, while the points that may be associated with this miasm but were not present in this case with dashed line around that point:
This case was managed as a classical homeopathic case, and only later in the course of the treatment we have used the Matrix method. There was a number of issues that didn’t come up in the classical case taking, but since the Matrix method uses a psychological Deep PEAT technique it is much easier for the patient to open up. These additional issues gave us a much clearer insight into the essence of the patient, as well as the connections between the patient’s issues. Many of these other issues would probably come up later in the course of the treatment, but this way, instead of waiting for months for that to happen, we can get them in a matter of minutes.
An Outline of the Patient’s Classical Homeopathic Case-taking
A 32 year old women who came to us because of fears and anxiety, or as she said “I have fear of fear”.
We can see that two of the three key reoccurring behavioral states – Fear point and Anxious – aroused point have been pointed out in at the very begining of the case taking, soon to be followed by the third, Passion/Panic point, connected to enclosed feeling and followed by nausea, the indication of elevated serotonin levels, and the Passion/Panic point does have elevated serotonin level, as well as NA.
The patient said that she is afraid of traveling by car because she fears that is she gets stuck in a traffic jam, she will get overwhelmed by enclosed feeling followed by nausea, she will feel disoriented, feeling as if she had butterflies in her stomach and that she would start to feel completely powerless.
When we asked her what helps her in such a situation she said that she just needs to run away and find a place to calm down in peace and quiet.
She also feels chest pain near her heart, by the doctors said she is fine after examination. She also often has stomach pain. She has painful menses, and polycystic ovaries. She starts feeling pain in ovaries as soon as she would step barefoot on a cold surface and it lasts for days. During the allopathic treatment of her polycystic ovaries, after unsuccessful treatments with antibiotics she was even prescribed to take insulin for the ovaries, but that didn’t do any good either.
She often gets sore throat with raised temperature and difficulties swallowing. She likes to eat pastry, fish, salads, salty and sweet food. Likes chocolate.
Her mother had cancer of cervix, 18 years ago. Her father didn’t have any serious illnesses. Her parents are divorced for 28 years.
She graduated from Faculty of Philosophy. She is unemployed. Her hobby is painting.
She said that she misses how she used to feel as a child.
On the first follow up after the remedy – Argentum nitricum 1M, she had chills, slightly elevated temperature, soreness of the entire body and mild headache. She dreamed her ex boyfriend his friends and in the dream she felt like she doesn’t belong there, any more. She felt pain in the pelvic region like she is going to have a period, accompanied by increased perspiration. She remembered that she used to have that kind of pain many years ago. On the other hand, she said that mentally she was feeling perfect, no more interrupted thoughts.
The next day after the second follow up, when the remedy was repeated, she has got her period and it was painless, with light menstrual flow, like it used to be 15 years ago. After 15 years it was her first period without painkillers. She went to Adriatic sea, through Bosnia, and before the remedy the high Bosnian mountains used to cause her panic attacks, but this time there was no panic, she just felt a bit strange because of the high altitude. She also said that she started to wake up early in the morning, and that her sense of smell is heightened. She had a sore throat and some stitching pain in the upper left part of the chest. The remedy was repeated in the higher potency – Argentum nitricum 10M.
On the next follow up she said that she went to a club and she was relaxed with no nausea and vomiting. For the first time in years she could sleep alone in her flat, and just for a moment she felt uncomfortable like the panic will start, but it didn’t.
After a year since she came to the homeopathic treatment, she was getting married and she moved to her husband’s country. In this period she had to travel by plane many times, in the company and alone, and she manage to get through all that without a single panic attack. Just once she felt a little uncomfortable, but she was able remain calm and soon this feeling was gone. She said that her appetite is very good.
Mirjana is co- author of a new book which is now available. It will be available on kindle in two weeks for the promotional price of $1.00.
Title: The Matrix Method with Tetractys Model
Authors: Dr Mirjana Zivanov, Dr Stojan Primovic, Dr Andreas Kelemen
Number of pages: 179
Price: 25 USD
Available on Amazon in paperback & kindle edition
[1] Waite, W.L. & Holder, M.D. (2003). Assessment of the Emotional Freedom Technique: An Alternative Treatment for Fear. Scientific Review of Mental Health Practice, 2 (2), 20-26.
[2] Haw, J., & Dickerson, M. (1998). The effects of distraction on desensitization and reprocessing. Behaviour Research and Therapy, 36, 765-769.
[3] Walley, E. J., Beebe, D. K., & Clark, J. L. (1994). Practical therapeutics: Management of common anxiety disorders. American Family Physician, 50, 1745-1753.
[4] Waite, W.L. & Holder, M.D. (2003). Assessment of the Emotional Freedom Technique: An Alternative Treatment for Fear. Scientific Review of Mental Health Practice, 2 (2), 20-26.
[5] Feinstein, David (December 2012). “Acupoint stimulation in treating psychological disorders: Evidence of efficacy”. Review of General Psychology 16 (4): 364–380. doi:10.1037/a0028602. p.7.
[6] Bakker, Gary M. (November 2013). “The current status of energy psychology: Extraordinary claims with less than ordinary evidence”. Clinical Psychologist 17 (3): 91–99. doi:10.1111/cp.12020
[7] Rothbaum, B. O., Hodges, L. F., Kooper, R., Opdyke, D., Williford, J., & North, M. M. (1995a). Effectiveness of virtual reality graded exposure in the treatment of acrophobia. American Journal of Psychiatry, 152, 626-628.
[8] Hugo Lövheim, A new three-dimensional model for emotions and monoamine neurotransmitters, Medical Hypotheses, Volume 78, Issue 2, February 2012, Pages 341-348, ISSN 0306-9877, http://dx.doi.org/10.1016/j.mehy.2011.11.016.
)
[9] A. Hay-Schmidt. The evolution of the serotonergic system. Proc. Biol. Sci., 267 (2000), pp. 1071–1079.
[10] Hugo Lövheim, A new three-dimensional model for emotions and monoamine neurotransmitters, Medical Hypotheses, Volume 78, Issue 2, February 2012, Pages 341-348, ISSN 0306-9877, http://dx.doi.org/10.1016/j.mehy.2011.11.016.
)
[11] Ibid.
[12] Ibid.
[13] Ingibjörg H. Jonsdottir and Björn Folkow, 11 – Defence and Defeat Reaction: Central Control and Peripheral Effects, In New Insights to Neuroimmune Biology, edited by Istvan Berczi, Elsevier, London, 2010, Pages 221-233, ISBN 9780123846914, http://dx.doi.org/10.1016/B978-0-12-384691-4.00011-0. )
[14] Hugo Lövheim, A new three-dimensional model for emotions and monoamine neurotransmitters, Medical Hypotheses, Volume 78, Issue 2, February 2012, Pages 341-348, ISSN 0306-9877, http://dx.doi.org/10.1016/j.mehy.2011.11.016.
)
[15] S. Kakade, P. Dayan. Dopamine: generalization and bonuses. Neural Networks, 15 (2002), pp. 549–559
[16] Juyang Weng, Stephen Paslaski, James Daly, Courtland VanDam, Jacob Brown, Modulation for emergent networks: Serotonin and dopamine, Neural Networks, Volume 41, May 2013, Pages 225-239, ISSN 0893-6080, http://dx.doi.org/10.1016/j.neunet.2012.11.008. )
[17] J. LeBlanc, M.B. Ducharme, Plasma dopamine and noradrenaline variations in response to stress, Physiology & Behavior, Volume 91, Issues 2–3, 8 June 2007, Pages 208-211, ISSN 0031-9384,
[18] Negative Correlation Definition | Investopedia. (2010, September 28). Retrieved May 30, 2015, from http://www.investopedia.com/terms/n/negative-correlation.asp
[19] Dongju Seo, Christopher J. Patrick, Patrick J. Kennealy, Role of serotonin and dopamine system interactions in the neurobiology of impulsive aggression and its comorbidity with other clinical disorders, Aggression and Violent Behavior, Volume 13, Issue 5, October 2008, Pages 383-395, ISSN 1359-1789, http://dx.doi.org/10.1016/j.avb.2008.06.003.
)
[20] N.D. Daw, S. Kakade, P. Dayan. Opponent interactions between serotonin and dopamine. Neural Networks, 15 (4–6) (2002), pp. 603–616
[21] Ferrari,F.P.,vanErp,A.M.M.,Tornatzky,W.,Miczek,K.A.,2003.Accumbaldopamine and serotonin in anticipation of then extaggressive episodeinrats.Eur.J.Neurosci.17,371–378.
[22] J Haller, G.B Makara, M.R Kruk, Catecholaminergic involvement in the control of aggression: hormones, the peripheral sympathetic, and central noradrenergic systems, Neuroscience & Biobehavioral Reviews, Volume 22, Issue 1, 27 December 1997, Pages 85-97, ISSN 0149-7634, http://dx.doi.org/10.1016/S0149-7634(97)00023-7.
)
[23] Hugo Lövheim, A new three-dimensional model for emotions and monoamine neurotransmitters, Medical Hypotheses, Volume 78, Issue 2, February 2012, Pages 341-348, ISSN 0306-9877, http://dx.doi.org/10.1016/j.mehy.2011.11.016.
)
[24] Ingibjörg H. Jonsdottir and Björn Folkow, 11 – Defence and Defeat Reaction: Central Control and Peripheral Effects, In New Insights to Neuroimmune Biology, edited by Istvan Berczi, Elsevier, London, 2010, Pages 221-233, ISBN 9780123846914, http://dx.doi.org/10.1016/B978-0-12-384691-4.00011-0. )
[25] N. Brunello, H. Akiskal, P. Boyer, G.L. Gessa, R.H. Howland, S.Z. Langer, J. Mendlewicz, M. Paes de Souza, G.F. Placidi, G. Racagni, S. Wessely, Dysthymia: clinical picture, extent of overlap with chronic fatigue syndrome, neuropharmacological considerations, and new therapeutic vistas, Journal of Affective Disorders, Volume 52, Issues 1–3, January–March 1999, Pages 275-290, ISSN 0165-0327, http://dx.doi.org/10.1016/S0165-0327(98)00163-3. )
[26] Bunney Jr.,W.E.,Davis,J.M.,1965.Norepinephrine in depressive reactions: a review. Arch. Gen.Psychiatry13,483–494.
[27] Berend Olivier, Serotonin: A never-ending story, European Journal of Pharmacology, Volume 753, 15 April 2015, Pages 2-18, ISSN 0014-2999, http://dx.doi.org/10.1016/j.ejphar.2014.10.031. )
[28] Hugo Lövheim, A new three-dimensional model for emotions and monoamine neurotransmitters, Medical Hypotheses, Volume 78, Issue 2, February 2012, Pages 341-348, ISSN 0306-9877, http://dx.doi.org/10.1016/j.mehy.2011.11.016.
)
[29] Juyang Weng, Stephen Paslaski, James Daly, Courtland VanDam, Jacob Brown, Modulation for emergent networks: Serotonin and dopamine, Neural Networks, Volume 41, May 2013, Pages 225-239, ISSN 0893-6080, http://dx.doi.org/10.1016/j.neunet.2012.11.008. )
[30] J. Zagrodzka, M. Wieczorek, A. Romaniuk, Social interactions in rats: Behavioral and neurochemical alterations in DSP-4-treated rats, Pharmacology Biochemistry and Behavior, Volume 49, Issue 3, November 1994, Pages 541-548, ISSN 0091-3057, http://dx.doi.org/10.1016/0091-3057(94)90066-3. )
[31] M. Wieczorek, A. Romaniuk. The effects of dorsal and ventral noradrenergic system lesions with DSP-4 on emotional–defensive behavior and regional brain monoamines content in the cat. Behav. Brain Res., 63 (1994), pp. 1–9
[32] J Haller, G.B Makara, M.R Kruk, Catecholaminergic involvement in the control of aggression: hormones, the peripheral sympathetic, and central noradrenergic systems, Neuroscience & Biobehavioral Reviews, Volume 22, Issue 1, 27 December 1997, Pages 85-97, ISSN 0149-7634, http://dx.doi.org/10.1016/S0149-7634(97)00023-7.
)
[33] Thomas R. Gregg, Allan Siegel, Brain structures and neurotansmitters regulating aggression in cats: implications for human aggression, Progress in Neuro-Psychopharmacology and Biological Psychiatry, Volume 25, Issue 1, January 2001, Pages 91-140, ISSN 0278-5846, http://dx.doi.org/10.1016/S0278-5846(00)00150-0. )
[34] J.D. Higley, A.J. Bennett. Central nervous system serotonin and personality as variables contributing to excessive alcohol consumption in non-human primates. Alcohol and Alcoholism, 34 (1999), pp. 402–418
[35] Dongju Seo, Christopher J. Patrick, Patrick J. Kennealy, Role of serotonin and dopamine system interactions in the neurobiology of impulsive aggression and its comorbidity with other clinical disorders, Aggression and Violent Behavior, Volume 13, Issue 5, October 2008, Pages 383-395, ISSN 1359-1789, http://dx.doi.org/10.1016/j.avb.2008.06.003. )
[36] Katrina R DeLeon, Jill M Grimes, Daniel F Connor, Richard H Melloni Jr., Adolescent cocaine exposure and offensive aggression: involvement of serotonin neural signaling and innervation in male Syrian hamsters, Behavioural Brain Research, Volume 133, Issue 2, 18 July 2002, Pages 211-220, ISSN 0166-4328, http://dx.doi.org/10.1016/S0166-4328(02)00004-9. )
[37] A. Bartels, S. Zeki. The neural correlates of maternal and romantic love. Neuroimage, 21 (3) (2004), pp. 1155–1166
[38] A. de Boer, E.M. van Buel, G.J. Ter Horst, Love is more than just a kiss: a neurobiological perspective on love and affection, Neuroscience, Volume 201, 10 January 2012, Pages 114-124, ISSN 0306-4522, http://dx.doi.org/10.1016/j.neuroscience.2011.11.017.
)
[39] S. Edwards, D.W. Self. Monogamy: dopamine ties the knot. Nat Neurosci, 9 (1) (2006), pp. 7–8
[40] N.D. Daw, S. Kakade, P. Dayan. Opponent interactions between serotonin and dopamine. Neural Networks, 15 (4–6) (2002), pp. 603–616
[41] Ibid.
[42] Franziska Maier, Josuah Merkl, Anna L. Ellereit, Catharine J. Lewis, Carsten Eggers, David J. Pedrosa, Elke Kalbe, Jens Kuhn, Thomas D. Meyer, Mateusz Zurowski, Lars Timmermann, Hypomania and mania related to dopamine replacement therapy in Parkinson’s disease, Parkinsonism & Related Disorders, Volume 20, Issue 4, April 2014, Pages 421-427, ISSN 1353-8020, http://dx.doi.org/10.1016/j.parkreldis.2014.01.001. )
[43] Thomas D Meyer, Ferdinand Keller, Is there evidence for a latent class called ‘hypomanic temperament’?, Journal of Affective Disorders, Volume 75, Issue 3, August 2003, Pages 259-267, ISSN 0165-0327, http://dx.doi.org/10.1016/S0165-0327(02)00051-4. )
[44] Fieve, Ronald R. (2006). Bipolar II: Enhance Your Highs, Boost Your Creativity, and Escape the Cycles of Recurrent Depression—The Essential Guide to Recognize and Treat the Mood Swings of This Increasingly Common Disorder. Emmaus, Pa.: Rodale Books. ISBN 978-1-59486-224-3.
[45] Dongju Seo, Christopher J. Patrick, Patrick J. Kennealy, Role of serotonin and dopamine system interactions in the neurobiology of impulsive aggression and its comorbidity with other clinical disorders, Aggression and Violent Behavior, Volume 13, Issue 5, October 2008, Pages 383-395, ISSN 1359-1789, http://dx.doi.org/10.1016/j.avb.2008.06.003. )
[46] Robert W. Gould, H. Donald Gage, Matthew L. Banks, Brandi L. Blaylock, Paul W. Czoty, Michael A. Nader, Differential effects of cocaine and MDMA self-administration on cortical serotonin transporter availability in monkeys, Neuropharmacology, Volume 61, Issues 1–2, July–August 2011, Pages 245-251, ISSN 0028-3908, http://dx.doi.org/10.1016/j.neuropharm.2011.04.007. )
[47] Wael M.Y. Mohamed, Sami Ben Hamida, Jean-Christophe Cassel, Anne Pereira de Vasconcelos, Byron C. Jones, MDMA: Interactions with other psychoactive drugs, Pharmacology Biochemistry and Behavior, Volume 99, Issue 4, October 2011, Pages 759-774, ISSN 0091-3057, http://dx.doi.org/10.1016/j.pbb.2011.06.032. )
[48] Ibid.
[49] Franz X. Vollenweider, Alex Gamma, Matthias Liechti, Theo Huber, Psychological and Cardiovascular Effects and Short-Term Sequelae of MDMA (“Ecstasy”) in MDMA-Naı̈ve Healthy Volunteers, Neuropsychopharmacology, Volume 19, Issue 4, October 1998, Pages 241-251, ISSN 0893-133X. )
[50] Robert W. Gould, H. Donald Gage, Matthew L. Banks, Brandi L. Blaylock, Paul W. Czoty, Michael A. Nader, Differential effects of cocaine and MDMA self-administration on cortical serotonin transporter availability in monkeys, Neuropharmacology, Volume 61, Issues 1–2, July–August 2011, Pages 245-251, ISSN 0028-3908, http://dx.doi.org/10.1016/j.neuropharm.2011.04.007. )
[51] Ibid.
[52] Dalena van Heugten-Van der Kloet, Timo Giesbrecht, Janelle van Wel, Wendy M Bosker, Kim PC Kuypers, Eef L Theunissen, Desirée B Spronk, Robbert Jan Verkes, Harald Merckelbach, Johannes G Ramaekers, MDMA, cannabis, and cocaine produce acute dissociative symptoms, Psychiatry Research, Available online 30 April 2015, ISSN 0165-1781, http://dx.doi.org/10.1016/j.psychres.2015.04.028. )
[53] A. de Boer, E.M. van Buel, G.J. Ter Horst, Love is more than just a kiss: a neurobiological perspective on love and affection, Neuroscience, Volume 201, 10 January 2012, Pages 114-124, ISSN 0306-4522, http://dx.doi.org/10.1016/j.neuroscience.2011.11.017.
)
[54] S. Zeki. The neurobiology of love. FEBS Lett, 581 (14) (2007), pp. 2575–2579
[55] D.G. Dutton, A.P. Aron. Some evidence for heightened sexual attraction under conditions of high anxiety. J Pers Soc Psychol, 30 (1974), pp. 510–517
[56] J. Micallef, O. Blin. Neurobiology and clinical pharmacology of obsessive-compulsive disorder. Clin Neuropharmacol, 24 (4) (2001), pp. 191–207
[57] D. Marazziti, H.S. Akiskal, A. Rossi, G.B. Cassano. Alteration of the platelet serotonin transporter in romantic love. Psychol Med, 29 (3) (1999), pp. 741–745
[58] Roberto Erro, Sabina Pappatà, Marianna Amboni, Caterina Vicidomini, Katia Longo, Gabriella Santangelo, Marina Picillo, Carmine Vitale, Marcello Moccia, Flavio Giordano, Arturo Brunetti, Maria Teresa Pellecchia, Marco Salvatore, Paolo Barone, Anxiety is associated with striatal dopamine transporter availability in newly diagnosed untreated Parkinson’s disease patients, Parkinsonism & Related Disorders, Volume 18, Issue 9, November 2012, Pages 1034-1038, ISSN 1353-8020, http://dx.doi.org/10.1016/j.parkreldis.2012.05.022. )
[59] Archer, T., Minor, B.G. and Post, C., Blockade and reversal of 5-methoxy-N,N-dimethyltryptamine-induced analgesia following noradrenaline depletion, Brain Research, 333(1985) 55-61.
[60] A. Fernandez-Guasti, S. Hansen, T. Archer, G. Jonsson, Noradrenaline-serotonin interactions in the control of sexual behavior in the male rat: DSP4-induced noradrenaline depletion antagonizes the facilitatory effect of serotonin receptor agonists, 5-MeODMT and lisuride, Brain Research, Volume 377, Issue 1, 2 July 1986, Pages 112-118, ISSN 0006-8993, http://dx.doi.org/10.1016/0006-8993(86)91196-0. )
[61] Hugo Lövheim, A new three-dimensional model for emotions and monoamine neurotransmitters, Medical Hypotheses, Volume 78, Issue 2, February 2012, Pages 341-348, ISSN 0306-9877, http://dx.doi.org/10.1016/j.mehy.2011.11.016.
)
[62] Ibid.
[63] E. Emanuele, N. Brondino, S. Pesenti, S. Re, D. Geroldi. Genetic loading on human loving styles. Neuro Endocrinol Lett, 28 (6) (2007), pp. 815–821
[64] Juyang Weng, Stephen Paslaski, James Daly, Courtland VanDam, Jacob Brown, Modulation for emergent networks: Serotonin and dopamine, Neural Networks, Volume 41, May 2013, Pages 225-239, ISSN 0893-6080, http://dx.doi.org/10.1016/j.neunet.2012.11.008. )
[65] N.D. Daw, S. Kakade, P. Dayan. Opponent interactions between serotonin and dopamine. Neural Networks, 15 (4–6) (2002), pp. 603–616
[66] Marcus Lira Brandão, Amanda Ribeiro de Oliveira, Sangu Muthuraju, Ana Caroline Colombo, Viviane Mitsuko Saito, Teddy Talbot, Dual role of dopamine D2-like receptors in the mediation of conditioned and unconditioned fear, FEBS Letters, Available online 14 March 2015, ISSN 0014-5793, . )
[67] S Nishizawa, C Benkeflat, S.N Young, M Leyton, S Mzengeza, C de Montiggny, P Blier, M Diksic. Differences between males and females in rates of serotonin synthesis in human brain. Proc. Natl. Acad. Sci., 94 (1997), pp. 5308–5313
[68] Takahiko Tanaka, Masami Yoshida, Hideyasu Yokoo, Masaru Tomita, Masatoshi Tanaka, Expression of Aggression Attenuates Both Stress-Induced Gastric Ulcer Formation and Increases in Noradrenaline Release in the Rat Amygdala Assessed by Intracerebral Microdialysis, Pharmacology Biochemistry and Behavior, Volume 59, Issue 1, January 1998, Pages 27-31, ISSN 0091-3057, http://dx.doi.org/10.1016/S0091-3057(97)00312-2. )
[69] Thomas R. Gregg, Allan Siegel, Brain structures and neurotansmitters regulating aggression in cats: implications for human aggression, Progress in Neuro-Psychopharmacology and Biological Psychiatry, Volume 25, Issue 1, January 2001, Pages 91-140, ISSN 0278-5846, http://dx.doi.org/10.1016/S0278-5846(00)00150-0. )
[70] M. Virkkunen, R. Rawlings, R. Tokola, R.E. Poland, A. Guidotti, C.B. Nemeroff, et al. CSF biochemistries, glucose metabolism, and diurnal activity rhythms in alcoholic, violent offenders, fire setters, and healthy volunteers. Archives of General Psychiatry, 51 (1994), pp. 20–27
[71] Dongju Seo, Christopher J. Patrick, Patrick J. Kennealy, Role of serotonin and dopamine system interactions in the neurobiology of impulsive aggression and its comorbidity with other clinical disorders, Aggression and Violent Behavior, Volume 13, Issue 5, October 2008, Pages 383-395, ISSN 1359-1789, http://dx.doi.org/10.1016/j.avb.2008.06.003. )
[72] Ibid.
[73] Ibid.
[74] M. Tanaka, A. Tsuda, H. Yokoo, M. Yoshida, Y. Ida, H. Nishimura. Involvement of the brain noradrenaline system in emotional changes caused by stress in ratsAnnals of the New York Academy of Sciences, Neurobiology of stress ulcers, vol. 597. New York (1990) 159–174
[75] T. Tanaka, H. Yokoo, K. Mizoguchi, M. Yoshida, A. Tsuda, M. Tanaka. Noradrenaline release in the rat amygdala is increased by stress: Studies with intracerebral microdialysis. Brain Res., 544 (1991), pp. 174–176
[76] Elizabeth P. Bauer, Serotonin in fear conditioning processes, Behavioural Brain Research, Volume 277, 15 January 2015, Pages 68-77, ISSN 0166-4328, http://dx.doi.org/10.1016/j.bbr.2014.07.028. )
[77] E.D. Leonardo, R. Hen. Genetics of affective and anxiety disorders. Annu Rev Psychol, 57 (2006), pp. 117–137
[78] Hugo Lövheim, A new three-dimensional model for emotions and monoamine neurotransmitters, Medical Hypotheses, Volume 78, Issue 2, February 2012, Pages 341-348, ISSN 0306-9877, http://dx.doi.org/10.1016/j.mehy.2011.11.016.
)
[79] M. Davis, et al. Phasic vs sustained fear in rats and humans: role of the extended amygdala in fear vs anxiety. Neuropsychopharmacology, 35 (1)(2010), pp.105–135
[80] Hugo Lövheim, A new three-dimensional model for emotions and monoamine neurotransmitters, Medical Hypotheses, Volume 78, Issue 2, February 2012, Pages 341-348, ISSN 0306-9877, http://dx.doi.org/10.1016/j.mehy.2011.11.016. )
[81] A.E. Patanwala, R. Amini, D.P. Hays, P. Rosen. Antiemetic therapy for nausea and vomiting in the emergency department. J Emerg Med, 39 (2010), pp. 330–336
[82] Hugo Lövheim, A new three-dimensional model for emotions and monoamine neurotransmitters, Medical Hypotheses, Volume 78, Issue 2, February 2012, Pages 341-348, ISSN 0306-9877, http://dx.doi.org/10.1016/j.mehy.2011.11.016. )
[83] David S. Chester, C. Nathan DeWall, Karen J. Derefinko, Steven Estus, Jessica R. Peters, Donald R. Lynam, Yang Jiang, Monoamine oxidase A (MAOA) genotype predicts greater aggression through impulsive reactivity to negative affect, Behavioural Brain Research, Volume 283, 15 April 2015, Pages 97-101, ISSN 0166-4328, http://dx.doi.org/10.1016/j.bbr.2015.01.034. )
[84] Takahiko Tanaka, Masami Yoshida, Hideyasu Yokoo, Masaru Tomita, Masatoshi Tanaka, Expression of Aggression Attenuates Both Stress-Induced Gastric Ulcer Formation and Increases in Noradrenaline Release in the Rat Amygdala Assessed by Intracerebral Microdialysis, Pharmacology Biochemistry and Behavior, Volume 59, Issue 1, January 1998, Pages 27-31, ISSN 0091-3057, http://dx.doi.org/10.1016/S0091-3057(97)00312-2. )
[85] There are a few more short steps that follow this in the Deep PEAT technique


Very Important Theory in Modern Homeopathy. It is new and excellent way to find perfect remedy.They explained it nicely. I already bought this book and reading day by day. I am learning many things from it. Great achievement by Dr Mirjana Zivanov and Her group. She is a Great Doctor.All the Best.
This is a very interesting and intriguing theory. A very original approach to get more in dept information about the patient. This theory may help to bridge the gap between homeopathy and modern science. Congratulations Dr Mirjana! Keep on the good work.