Most of us will remember our college years where teachers gently and less-gently (as in my case!) reminded us to stop picking remedies for cases with the justification that those remedies were “for migraines” or “for anxiety”.
“Three legged stool!” “Strange, rare, peculiar!”
I only too vividly remember my teacher turning purple as he yelled these commands to us on clinic days. Bless him, he was just trying to erase our allopathic disease-way of thinking and training us to be true homeopaths who individualize their case taking and prescriptions. Today, I am so glad my teacher was so violently invested in us! After all, his teaching taught me to take a fertility case well.
Although we all know that we should be prescribing on the specifics, I all too often hear homeopaths prescribing remedies like Sepia, Pulsatilla or Folliculinum almost routinely in fertility cases because they are classed as “hormonal” remedies. Newsflash my friends, all homeopathic remedies are “hormonal”. After all, if a patient’s symptoms show the picture of Veratrum Album and they happen to be estrogen dominant, Sepia is not going to fix that hormone imbalance while Veratrum Album will!
Finding the most indicated individualized remedy for our patients is still at the core of homeopathy! Nothing has changed since Hahnemann taught us in paragraph 153 of his Organon:
“..the more striking, exceptional, unusual, and odd (characteristic) signs and symptoms… are to be especially…kept in view. These, above all, must correspond to very similar ones in the symptom set of the medicine sought if it is to be the most fitting one for cure.” (Brewster O’Reilly, 1996)
I think that the reason that it is so easy to fall into the trap of selecting common fertility remedies – even when we know better – is because those are the pictures we are presented with in our consultation rooms. We see tired women with heavy long periods and short cycles, and so we prescribe Sepia. We get hypothyroid patients that suppress their emotions and give them Natrum Muriaticum. We get patients with a high sex drive and hot flushes and send them off with Lachesis.
To make things worse, we are often encouraged in this lazy way of prescribing by the outcomes as 6 out of 10 cases are cured or at least helped with those remedies. But what about the other 40%? The answer is that we need to look beyond the common symptoms. Common symptoms? We need to discard those! (That’s my creative translation of part 2 of paragraph 153) (Brewster O’Reilly, 1996).
Taking a fertility case well, is really no different than taking any other case: find the strange, rare and peculiar symptoms (SRP’s)! However, discovering those SRP’s and finding the most indicated remedy, only works if you understand at least partially what is keeping the couple from conceiving and if you know which symptoms are common for those blocks.
Then when you have found “the remedy”, you can always confirm it for yourself by identifying whether you know it as a typical ovulation, estrogen dominance, metal toxicity, fill-in-the-blanks _______ remedy.
Finding the SRP’s in female hormone imbalance
When it comes to the hormonal aspect of a fertility case, a homeopath needs to understand and study at least the following to learn to find the SRP’s; charting, hormone imbalance(s) and their glands.
Charting in my opinion, is the most underused tool by both homeopaths and fertility specialists. Through the fertility charts of our patients, we can not only identify patterns of their hormone (im)balance over the course of years and months, but we can also identify what is going on for them currently.Short term charts can tell us where our patients are in their cycles. Are they (about to be) fertile? Then they need to know so they can make the most of their fertile window! Are they ovulating later than normal? Is that because their adrenals are particularly stressed or are their FSH levels high and is menopause approaching? All this information helps us to help our patients make the most of every cycle, so they can time baby-making well, but it also helps us to tweak their treatment appropriately, even before problems actually become problems.
From the longer term patterns we can identify whether hormone levels are generally good enough to conceive and hold onto a pregnancy or whether there is a chronic disturbance of the main hormonal glands. Through charting we can sometimes pick up (and therefore treat) problems before they are reflected in blood work. Charting can even help us identify why hormone balance is off when this does come up in blood tests. Because charting give us so much insight into the hormonal and glandular condition of a patient, it can often give answers where couples before have been told they suffer with unexplained infertility.
Since charting shows us the condition of the hormone balance and glandular health of a woman, it can also help us as homeopaths to sift through her symptoms and find the SRP’s.For example, your patient comes in with heavy bleeding. Do you use that as a symptom in repertorization or not? If her charts show you that she is estrogen dominant, then my argument would be not to, as heavy bleeding is typical of estrogen dominance. In fact, I would probably never use that symptom except perhaps as a confirmatory symptom after selecting a remedy.The symptom “heavy menses” may be quite an obvious one and you may not use it anyway because the rubric is so large. “Female MENSES, general, profuse” brings up 271 remedies in my repertory (Murphy, 2005). Those numbers alone are a dead give-away that this symptom is not specific enough for us to use.
Let me however give you a much less obvious example. Your patient comes in with severe PMS symptoms around ovulation. The only rubric you can find is “ailments around ovulation” which gives us 3 remedies; Sepia, Folliculinumand Lapis Granites Murvey. That seems pretty good right? Small rubric, few numbers and so it looks like an SRP. However, if you can tell from other symptoms and from your patient’s chart that they are estrogen dominant, then this is actually not a good rubric. Yes, these remedies have a good chance of working, but there is an equally good chance that they won’t do the trick, because PMS around ovulation is a typical estrogen dominance issue! PMS around ovulation can often occur when women are used to high estrogen levels, because before ovulation estrogen plummets, which brutally throws these women off their high. So if you choose one of the named remedies in this case, you are basically picking another “hormonal remedy” and prescribing on a symptom that is to be expected with the condition.
Let me give you another example. A patient comes in with the diagnosis of hypothyroidism. She is overweight, tired and complains of cold hands. When you go by these symptoms – which are typical for an under functioning thyroid – you may end up with CalcareaCarbonica on repertorization or because you know it as a thyroid remedy (which by the way is because CalcareaCarbonica has low metabolism generally). When, however, you discard those obvious symptoms and you find that she also gets migraines which are relieved by licking salt off the palm of her hand, she hasn’t cried since 1996, and she gets palpitations when she lies down in bed at night, then you know that you’ve got yourself a Natrum Muriaticum case. Guess what, Natrum Muriaticum can also be obese, have cold hands and is known as a “thyroid remedy”! Now you know that you’re taking the case the right way around.
One more example. Another thyroid patient comes in. She is also overweight, has a hypothyroid diagnosis, has cold hands and is tired. Will you give her CalcareaCarbonica,or perhaps Natrum Muriaticum because your last patient taught you that’s a thyroid remedy too? No of course not! Ignore those symptoms and keep asking. When you keep asking, she may tell you that she has ringing and eczema in her left ear, that her 5year old cesarean scar is getting inflamed, she actually does cry and feels better for it, and feels like she should exercise as she feels better for it but just cannot get herself off the couch. Now you’ve got a great Graphites picture. Surprise, surprise; Graphites too has poor circulation with coldness, is known for obesity and has thyroid affinity.
Having said all of this, of course I prescribe Sepia, Pulsatilla, Natrum MuriaticumandFolliculinum (to name a few) a LOT in fertility cases. They are wonderful remedies that can sometimes even sort someone out within just one cycle. However, they do not sort all cases, sometimes work temporarily, or sort out some symptoms without curing the infertility.
That is why it is important that you understand the pictures of different types of hormone imbalance so that you do not risk taking the case too broadly and missing out on the indicated remedy or remedies. It will reduce the length of treatment due to trial and error remedies and avoids disappointment in homeopathy.
Therefore, in order to take a fertility case well, we need to thoroughly understand how the hormonal feedback system works and how the ovaries, adrenal glands, thyroid, hypothalamus, pancreas, and anterior pituitary gland communicate. When we know how they work, then we are also able to recognize when the system is out of balance in a patient.In order for us to then understand which are the common symptoms in that patient, and which are their SRP’s, we need to have good knowledge of the effects of particular hormone conditions.
Examples of (hormone) conditions we need to understand when taking fertility cases:
- Estrogen dominance
- Low progesterone
- Hypothyroidism – both auto-immune adrenal/hypothalamic induced
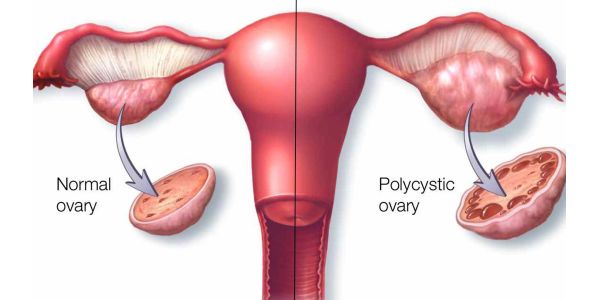
- Poly cystic ovaries syndrome
- Adrenal fatigue
Only then will we recognize the patterns of a patient’s symptoms and will we be able to discard some as common. Only then we will be able to find the SRP’s and gems will come to the surface which are otherwise overshadowed by the polychrests and “hormonal” remedies. Only then will know that we are truly taking a fertility case well.
Brewster O’Reilly, W., ed., 1996. Organon of the Medical Art. 3rd edition. Palo Alto: Birdcage Books.
Murphy, R., 2005. Homeopathic Clinical Repertory. Third ed. Blacksburg: R.R. Donnelley and Sons.

a wonderful article many thanks
Thank you Beverley, I’m glad you liked it!
An very valuable article which describes numerous variables that must be considered in such cases. Without this knowledge, accurate prescribing would be difficult.
Glad we are on the same page JZ!