
Authors:
Zainab Thanon Hasan1
Dr. Mohammed Qasim Yahya Mal Allah AlAtrakji2
Dr. Ahmed KayesMehuaiden3
1 Clinical pharmacist, Al-Salam Teaching Hospital, Mosul, Iraq
2 MBChB, M.Sc., Ph.D. Pharmacology, Department of Pharmacology, College of Medicine, Baghdad University, Iraq
3 MBChB., F.I.C.M.S.(clinical hematology), Clinical hematologist, Ibn-Sina Teaching Hospital, Mosul, Iraq
Available online 12 October 2021.
https://doi.org/10.1016/j.ijid.2021.10.012Get rights and content
Under a Creative Commons license
open access
Highlights
- Melatonin may be beneficial in preventing complications in patients with COVID-19.
- Melatonin can be used to reduce the mortality rate in patients with COVID-19.
- Melatonin may be beneficial as an adjuvant therapy in patients with COVID-19.
Abstract
The purpose of this study is to determine the effect of melatonin on thrombosis, sepsis, and mortality rate in adult patients with severe coronavirus infection (COVID-19).
Methods: This single-center, prospective, randomized clinical trial was conducted from 1 December 2020 to 1 June 2021 at Al-Shifaa hospital in Mosul, Iraq. There were 158 patients with severe COVID-19 included in the study, 82 in the melatonin group (who received 10 mg melatonin in addition to standard therapeutic care), and 76 in the control group (given standard therapeutic care only). Patients were chosen by blocked randomization design. The physician then evaluated and recorded the incidence of thrombosis, sepsis, and mortality rate on days 5, 11, and 17 of symptoms.
Results: The intervention group consisted of 82 patients, while the control group consisted of 76 patients. In comparison to the control group, thrombosis and sepsis developed significantly less frequently (P < 0.05) in the melatonin group during the second week of infection, while mortality was significantly higher in the control group (P < 0.05).
Conclusions: Adjuvant use of Melatonin may help reduce thrombosis, sepsis, and mortality in COVID-19 patients.
Keywords
COVID-19
Melatonin
Clinical trial
Introduction
Since December 31, 2019, when the People’s Republic of China’s health authorities notified the World Health Organization of several cases of pneumonia with an unknown etiology in the city of Wuhan, which called corona virus disease 2019 (COVID-19), the infection has spread throughout the world, with 170 million confirmed cases and more than 3.5 million deaths at the time of article writing (on June, 2020). (According to Worldmeter, July 2021).
Figure 1.
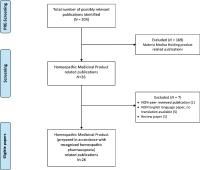
Figure 1. Flow diagram that illustrates the progress of patients through the trial.
Thrombotic complications are common in COVID-19 and are associated with a significant increase in mortality and morbidity. COVID-19 may enhance sepsis-induced hypercoagulability (Barnes BJ., et al. 2020).
While COVID-19 infection continues to spread globally and the need for urgent adjuvant treatment increases, clinical trials are underway to investigate the use of appropriate immunosuppressive and immunomodulatory agents, and also specific drugs to target individual pro-inflammatory cytokines (Soy, et al. 2020). There is a need for drugs that can potentially diminish some of the effects of the potentially deadly immune response.
Melatonin is a multifunctional molecule that has been shown to have antioxidant, anti-inflammatory, and immunomodulatory properties. Melatonin has been shown to be involved in the regulation of sleep and blood pressure, as well as in the improvement of viral respiratory disorders. As a result of these properties, recent publications have recommended melatonin for its potentially beneficial effects on clinical outcomes in patients with COVID-19. (Huang C. et al. 2020; A.T. Slominski et al. 2018). However, there is a limited number of clinical and laboratory studies on the adjunctive use of melatonin in COVID-19 infection, one used melatonin 9 mg /day (Gholamreza, et al. 2020) and two ongoing registered trials (Ali Ameri, et al. 2021; Miguel Rodriguez-Rubio, et al. 2021)
Thus, a randomized clinical trial was designed and conducted in this study to compare the efficacy of adding oral melatonin to standard treatment in hospitalized adult patients with severe COVID-19 infection.
Method
The current study was a single-center, open-label, randomized clinical trial to determine the effect of melatonin on thrombosis, sepsis, and mortality in adults with COVID-19 admitted to Al-Shifaa Hospital in Mosul, Iraq from December 1, 2020 to June 1, 2021. The diagnosis of COVID-19 was confirmed using reverse transcriptase-polymerase chain reaction (RT-PCR), as well as findings consistent with COVID-19 pneumonia on computed tomography (CT) or chest radiography. Thompson’s equation was used to determine the sample size (Steven K and Thompson, 2012). Patients who met the inclusion and exclusion criteria were eligible. Hospitalized patients with confirmed severe COVID-19 infection, the age greater than 18 years or less than 80 years were included in the study. The following criteria were used to exclude individuals: the age of patients less 18 or greater than 80 years, known melatonin allergy, pregnancy, lactating female, renal impairment, liver impairment, autoimmune disease, cancer, or terminal medical illness. The ethical committee of Baghdad university/college of medicine approved the study protocol (approval number: 20201110872).
158 patients were enrolled in the current study. They were randomly assigned to intervention or control groups using a random block design. The two treatment groups were melatonin (A) and control (B), and the block size was 2 × 2=4. Within each block, the treatment allocation was as follows: (1) AABB, (2) BBAA, (3) ABAB, (4) BABA. (5) ABBA (6) BAAB.
All patients of the control group received standard therapy ((Oxygen therapy, Antiviral agents: Remdesevir (day one 200 mg intravenously infusion during 1 hour, then in day 2, 3, 4 & 5 the patients given 100 mg intravenously infusion during 1 hour), Antibacterial agents: levofloxacin 500 mg intravenously per day was used empirically for secondary bacterial infections, Corticosteroid: (dexamethasone 24 mg intravenously per day), Anticoagulant: enoxaparin 6000 unit once daily for prophylaxis and twice daily for therapeutic treatment of thrombosis). whereas All the intervention group patients received standard therapy plus 10 mg melatonin (Natrol®) once daily 20-30 minutes before bed time for 14 days following diagnosis. The physician who administered melatonin was also responsible for treatment and assessment of patientsʼ condition. Thrombosis was diagnosed clinically and laboratory as Pulmonary Embolism, Deep Venous Thrombosis (DVT), and Ischemic stroke: imaging studies (computed tomography or magnetic resonance imaging of the brain), doppler ultrasound for DVT, CT angiography, and D-dimer were ordered in accordance with the clinical presentation, and sepsis was diagnosed on days 5, 11, and 17 of symptoms by a physician. All data collected were entered into a computer database.
Statistical analysis
SPSS software was used to conduct statistical analyses (version 20.0; IBM). The categorical variables (age, gender, and comorbidities such as hypertension, ischemic heart disease, diabetes mellitus, and asthma) were expressed as counts and percentages of patients in the melatonin and control groups, respectively. The Chi-square χ2 and Fisher exact tests were used to compare these variables. The Kolmogorov-Smirnov (KS) test was used to determine the normality of the data. Non-parametric statistical methods were employed for not normally distributed continuous variables, Mann-Whitney U test was used in variable differences between the two groups. The Chi-square χ2 and Fisher exact tests are used to compare categorical variables between the two groups (thrombosis, sepsis, and death). All analyses were conducted on a two-sided basis, with a (P ≤ 0.05) considered statistically significant.
Results
In both groups, the baseline demographic and clinical characteristics of the patients are shown in (Table 1). Males made up 72.2 percent of the patients in the current study, while females made up 27.8 percent, and there was no significant difference in gender between the two groups (P > 0.05).
Table 1. Demographic and Clinical Characteristics of COVID 19 patients in melatonin group and control group
| P-value | df | Melatonin group (n=82) | Control group(n=76) | All patients(n = 158) | Patient characteristics |
| 0.393 ͣ | . | 56.8±7.5 | 55.7±8.0 | 56.3±7.7 | Age (mean ± SD) |
| 0.725° | 1 | 58(70.7%) 24(29.3%) |
56(73.7%) 20(26.3%) |
114(72.2%) 44(27.8%) |
Gender Male no.(%) Female no. (%) |
| 0.055° 0.394° 0.863° 0.113° |
1 | 50(61.0%) 15(18.3%) 25(30.5%) 5(6.1%) |
34(44.7%) 10(13.2%) 22(28.9%) 11(14.5%) |
84 (53.2%) 25(15.8%) 47(29.7%) 16(10.1%) |
Other comorbidities Hypertension Ischemic heart disease Diabetes mellitus Asthma |
df= degree of freedom, SD= standard deviation, n= number of patient, %= percentage of patients in each group, °= no significant difference (P > 0.05) using Chi-square test, ͣ = no significant difference (P > 0.05) using Mann-Whitney U test
The study population was 56.3 ±7.3 years old (mean ±SD), with a range of 32 to 78 years, and there was no significant difference in age between the two groups (P > 0.05).
Other comorbidities were present in 70.3 percent of patients, and there was no significant difference between the two groups in relations of hypertension, ischemic heart disease, asthma, and diabetes mellitus (P > 0.05). (See Table 1)
Effect of melatonin on developing thrombosis in COVID-19 patients:
Fisher exact test revealed no significant difference between the two groups at the baseline (day 5 of symptoms) (P = 1.000). Additionally, no significant difference in developing thrombosis was observed between the two groups on day 11 (P = 1.000). While developing thrombosis was significantly greater in the control group than in the melatonin group on day 17 (P < 0.05), (See Table 2) .
Table 2. Effect of melatonin on thrombosis in COVID 19 patients
| P-value | df | Control group (n=76) | Melatonin group (n=82) | All patients (n = 158) | |
| 1.000 | 1 | 0(0.0%) | 1(1.2%) | 1(0.6%) | Day 5 |
| 1.000 | 1 | 3(3.9%) | 3(3.7%) | 6(3.8%) | Day11 |
| 0.037* | 18(23.7%) | 9(11.0%) | 27(17.1%) | Day17 |
n=number of patients, df= degree of freedom, *Significant using Fisher exact test
A binary logistic regression model was used in which a melatonin used, age, gender, hypertension, ischemic heart disease, diabetes mellitus and asthma were considered as explanatory variable and thrombosis as dependent variable. Considering the Exp (β), an odds ratio equal to 1 shows no effect; an odds ratio greater than 1 shows the variable increase the odds of outcome target level; and an odds ratio less than 1 indicates the variable in question decrease the odds of the outcome target level .(Garson, D.G. 2013)
From the odds ratio evaluation, the probability of developing thrombosis in patients used melatonin (in melatonin group) was 0.309 times less likely compared to patients not used melatonin (in control group) as in (see Table 3).
Table 3. Logistic regression analysis to determine melatonin use associated with thrombosis in COVID-19 patients.
| B | S.E. | Wald | df | Sig. | Exp.(B) | 95% C.I. for Exp(B) | ||
| Lower | Upper | |||||||
| Melatonin | -1.174 | .504 | 5.428 | 1 | .020* | .309 | .115 | .830 |
| Age | .099 | .039 | 6.419 | 1 | .011* | 1.105 | 1.023 | 1.193 |
| Gender | -.635 | .579 | 1.201 | 1 | .273 | .530 | .170 | 1.650 |
| Hypertension | -.577 | .511 | 1.274 | 1 | .259 | .561 | .206 | 1.530 |
| Ischemic heart disease | 1.335 | .564 | 5.599 | 1 | .018* | 3.800 | 1.258 | 11.481 |
| Diabetes mellitus | .735 | .508 | 2.093 | 1 | .148 | 2.086 | .770 | 5.648 |
| Asthma | .649 | .688 | .891 | 1 | .345 | 1.914 | .497 | 7.367 |
| Constant | -7.048 | 2.217 | 10.103 | 1 | .001* | .001 | ||
B = coefficient, SE= standard error of B, df= degree of freedom, Exp(B)= Estimated odds ratio, C.I= Confidence interval for exp(B), *Significant using binary logistic regression
Effect of melatonin on developing sepsis in COVID-19 patients:
No patients developed sepsis during the baseline period (day 5 of symptoms) (no difference between the two groups). On day 11, two patients (2.4 percent) in the melatonin group developed sepsis, compared to eight patients (10.5 percent) in the control group. Chi square analysis revealed a significant difference between the two groups (P = 0.050). On day 17, sepsis developed significantly more frequently in patients in the control group (35.5 percent) than in patients in the melatonin group (8.5 percent) (P = 0.000) (See table 4).
Table 4. Effect of melatonin on sepsis in COVID 19 patients
| P-value | Df | Control group (n=76) | Melatonin group (n=82) | All patients (n = 158) | |
| 1.000 | 1 | (0%) | 0(0%) | 0(0%) | Day 5 |
| 0.050* | 1 | 8(10.5%) | 2(2.4%) | 10(6.3%) | Day11 |
| 0.000* | 1 | 27(35.5%) | 7(8.5%) | 34(21.5%) | Day17 |
n=number of patients, df= degree of freedom, *Significant using Fisher exact test
From the odds ratio evaluation in the binary logistic regression analysis, the probability of developing sepsis in patients used melatonin (in melatonin group) was 0.071 times less likely compared to patients not used melatonin (in control group) as in (Table 5).
Table 5. Logistic regression analysis to determine melatonin use associated with sepsis in COVID-19 patients.
| B | S.E. | Wald | df | Sig. | Exp.(B) | 95% C.I. for Exp(B) | ||
| Lower | Upper | |||||||
| Melatonin | -2.642 | .624 | 17.949 | 1 | .000* | .071 | .021 | .242 |
| Age | .157 | .046 | 11.766 | 1 | .001* | 1.170 | 1.070 | 1.279 |
| Gender | -.563 | .620 | .825 | 1 | .364 | .569 | .169 | 1.920 |
| Hypertension | -.520 | .556 | .876 | 1 | .349 | .594 | .200 | 1.766 |
| Ischemic heart disease | .622 | .661 | .885 | 1 | .347 | 1.862 | .510 | 6.803 |
| Diabetes mellitus | 2.243 | .597 | 14.131 | 1 | .000* | 9.418 | 2.925 | 30.322 |
| Asthma | 1.829 | .798 | 5.250 | 1 | .022* | 6.225 | 1.303 | 29.744 |
| Constant | -12.918 | 2.910 | 19.704 | 1 | .000* | .000 | ||
B = coefficient, SE= standard error of B, df= degree of freedom, Exp(B)= Estimated odds ratio, C.I= Confidence interval for exp(B), *Significant using binary logistic regression
Effect of melatonin on mortality rate in COVID-19 patients
According to the Chi square test (χ2), the mortality rate was significantly higher in the control group (17.1%) than in the melatonin group (1.2%), df = 1, (P = 0.001). (See table 6).
Table 6. Effect of melatonin on mortality in COVID 19 patients
| P-value | df | Control group (n=76) | Melatonin group (n=82) | All patients (n = 158) | |
| 0.000* | 1 | 13(17.1%) | 1(1.2%) | 14(8.9%) | Death |
n=number of patients, df= degree of freedom, *Significant using Fisher exact test
Discussion:
Worldwide, the COVID-19 pandemic has infected and killed millions of people. These large numbers necessitate a rapid development of clinical trials evaluating therapies capable of lowering the alarmingly high death rate. As a result, a large number of drugs have been studied in COVID-19 patients. Melatonin’s efficacy as an adjunctive therapy has been demonstrated in a variety of diseases (Biancatelli RMLC, et al. 2020; Zhang R, et al. 2020). There are, however, few trials evaluating the use of melatonin in patients with COVID-19 (Gholamreza, et al. 2020; Ali Ameri, et al. 2021; Miguel Rodriguez-Rubio, et al. 2021), while our study is randomized trial evaluating the efficacy and safety of 10 mg oral melatonin as an adjunctive therapy in patients hospitalized with severe COVID-19. It has been well found that melatonin administration could alleviate viral infection-induced oxidative stress as well as increasing the antioxidant activity (Habtemariam S, et al. 2017). In the current study three clinical complications (Thrombosis, sepsis & mortality rate) were evaluated.
Effect of Melatonin on Thrombosis in COVID-19 Patients:
Coronaviruses have been shown to enter cells via angiotensin-converting enzyme 2 (ACE-2) receptors, which are predominantly found on the alveolar epithelium and endothelium. Endothelial cell activation is thought to be the primary cause of thrombosis. Inclusion bodies from viruses have been identified in endothelial cells from a variety of organs, including the lung and gastrointestinal tract (Varga Z, et al. 2020). Rapid viral replication results in the release of large amounts of inflammatory mediators. One theory proposed that neutrophil extracellular traps (NETs) could be the source of hypercoagulation in severe COVID-19 patients. High NET levels in the blood are associated with elevated thrombin levels, which are predictive of adverse cardiac events that can result in major organ damage (Barnes BJ. Et al. 2020). In severe cases of COVID-19, a retrospective analysis of 452 patients revealed a significant increase in neutrophil counts (Qin C, et al. 2020). NETs have the ability to alter endothelial barrier structures, resulting in an increase in vascular endothelial permeability and a decrease in anti-thrombotic and anti-inflammatory properties (Ma Y, et al. 2019; Hernández-Reséndiz S, et al. 2018). Local injection of melatonin (140 pg) into endothelial cells effectively reduced endothelial cell vascular permeability induced by leukotriene B4-activated neutrophils, as demonstrated in an in vivo rodent experiment. Melatonin’s inhibition of endothelial cell hyper-adhesiveness likely mediated the decrease in vascular permeability (Lotufo CM, et al. 2006). In 46 healthy young men, oral melatonin (3 mg) administration resulted in an inverse relationship between procoagulant measures, with increased plasma melatonin predicting lower FVIII:C (P = 0.037) and fibrinogen (P = 0.022) levels (Wirtz PH, et al. 2008).
The increased D-dimer level is one of the most consistent findings. Although numerous inflammatory processes can affect D-dimer levels, they almost certainly reflect intravascular thrombosis to some extent in patients with COVID-19 (Leonard-Lorant I, et al. 2020; Cui S, et al. 2020). An elevated D-dimer level (>1000 ng/mL) at admission was associated with an increased risk of in-hospital death in the early studies emerging from China (Zhou F, et al. 2020). The true prevalence of COVID-19-associated thrombosis is unknown, as the majority of studies to date have lacked systematic and comprehensive investigation protocols. As a result, individuals infected with COVID-19 faced a risk of venous thromboembolism (VTE) of up to 25%. (Bikdeli B, et al. 2020; Chen G, et al 2020).
At day 17 of symptoms, 23.7 % of patients in the control group developed thrombosis, compared to 11% in the melatonin group (P < 0.05). The aforementioned data are consistent with this study, which established a significant effect of melatonin use on thrombosis.
Effect of Melatonin on Sepsis in COVID-19 Patients:
Sepsis is defined as organ dysfunction that is potentially fatal as a result of an abnormal host response to infection (Singer M, et al. 2016). Sepsis may be caused by a number of different pathogens. Sepsis is primarily caused by bacterial infection. However, up to 42% of sepsis patients had negative cultures, implying a nonbacterial cause (Phua J, et . 2013). Although almost any virus can cause sepsis in susceptible patients, viral sepsis is a very rare clinical diagnosis. Increased awareness, early detection of viral sepsis, rapid administration of appropriate antiviral medications, and prompt treatment can significantly reduce viral sepsis-related deaths (Reinhart Konrad, et al. 2017). With time, a significant difference in the development of sepsis was observed between the melatonin and control groups (at day 17 of symptoms, 35.5 percent of patients in the control group develop sepsis versus 8.5 percent in the melatonin group) (P < 0.001). Although no study has been conducted on the effects of melatonin on sepsis in COVID-19 patients, a recent clinical trial found that intravenous administration of 60 mg/d of a melatonin formulation improved septic patients, decreased their mortality to zero, and decreased their hospital stay by 40%. (Dario A. et al. 2020). Another trial used 9 mg of melatonin per day in COVID-19 patients showed significant reduction of hospital stay duration (p < 0.05) and improved clinical symptoms as well as the level of CRP and the pulmonary involvement in the melatonin group (P < 0.05) (Gholamreza, et al. 2020). This trial tested the effect of melatonin tablet 10 mg as it is the available dosage form in our country and to assure good compliance.
Effect of Melatonin on Mortality rate in COVID 19 Patients:
As previously demonstrated, thrombosis and sepsis associated with higher mortality rate & were improve by melatonin administration. As a result, it is entirely reasonable that melatonin resulted in a lower mortality rate in COVID-19 patients. This implied effect of melatonin was quantified directly in this study, which found that 17.1% of in-hospital patients in the control group died compared to 1.2 percent of patients in the melatonin group (P< 0.001).
The limitations of this trial were the open labeled and single-centered which could restrict the generalizability of the results.
Conclusion
The results of this study demonstrated that oral melatonin, when added to standard of care, was more effective than standard of care alone in patients hospitalized with severe COVID-19. Improved thrombosis, sepsis, and mortality rates support the adjuvant melatonin’s efficacy in mitigating this infectious disease. Given melatonin’s superior performance as a cheap, highly safe, and readily available medication, it is strongly recommended to be addressed in future studies.
Acknowledgement
I would like to express my deep thanks to assistant professor Dr. Mohammed Qasim Yahya for his great and unlimited support and a special thanks to Dr. Ahmed Kayes Mehuaiden for his contribution.
Conflict of interest
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Ethical approval
The patients provided informed consent to provide specimen and clinical data, and the study received approval by the ethical committee of Baghdad University /college of medicine.
References
Ali Ameri, Masoomeh Frouz, Manoochehr, et al. Evaluation of the effect of melatonin in patients with COVID-19-induced pneumonia admitted to the Intensive Care Unit: A structured summary of a study protocol for a randomized controlled trial. Iranian registry of clinical trial . (2021) the registration number (IRCT20200506047323N7). available at https://doi. org/10.1186/s13063-021-05162-3.
Barnes BJ, Adrover JM, Baxter-Stoltzfus A, et al. Targeting potential drivers of COVID-19: Neutrophil extracellular traps. J. Exp. Med. (2020) 217 (6).
Biancatelli RMLC, Berrill M, Mohammed YH and Marik PE. Melatonin for the treatment of sepsis: The scientific rationale. J Thorac Dis. (2020) 12(Suppl 1): 54–S65.
Bikdeli B, Madhavan MV, Jimenez D, et al. COVID-19 and thrombotic or thromboembolic disease: implications for prevention, antithrombotic therapy, and follow-up. J Am Coll Cardiol . (2020) 75: 2950–2973.
Chen G, Wu D, Guo W, et al. Clinical and immunological features of severe and moderate coronavirus disease 2019. J Clin Invest (2020); 130: 2620–2629
Cui S, Chen S, Li X, et al. Prevalence of venous thromboembolism in patients with severe novel coronavirus pneumonia. J Thromb Haemost (2020) 18: 1421–1424.
Dario A. Germaine E., Juan C. et al. Clinical trial to test the efficacy of melatonin in COVID-19. J Pineal Res. (2020) 20: 83.
Garson, D.G. Logistic Regression: Binary &Multinominal; Statistical Associates Publishers: Asheboro, NC, USA, (2013)1–52.
Gholamreza, Mostafa, Taleb, et al. Efficacy of a Low Dose of Melatonin as an Adjunctive Therapy in Hospitalized Patients with COVID-19: A Randomized, Double-blind Clinical Trial. (2020) Clinical Trials.gov Identifier: NCT0440952
Habtemariam S, Daglia M, Sureda A, Selamoglu Z, Fuat Gulhan M, Mohammad Nabavi S. Melatonin and respiratory diseases: a review. Curr Top Med Chem. (2017) 17:467-488.
Hernández-Reséndiz S, Muñoz-Vega M, Contreras WE, et al. Responses of endothelial cells towards ischemic conditioning following acute myocardial infarction. Cond Med. (2018) 1(5):247–258.
Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet (2020) 95, 497–506.
Leonard-Lorant I, Delabranche X, Severac F, et al. Acute pulmonary embolism in COVID-19 patients on CT angiography and relationship to D-dimer levels. Radiology (2020) 296 (3).
Lotufo CM, Yamashita CE, Farsky SH, et al. Melatonin effect on endothelial cells reduces vascular permeability increase induced by leukotriene B4. Eur. J. Pharmacol. (2006) 534 534 (1-3): 258–263.
Ma Y, Yang X, Chatterjee V, et al. Role of neutrophil extracellular traps and vesicles in regulating vascular endothelial permeability. Front Immunol. (2019) 10: 1037.
Miguel Rodríguez-Rubio, Juan Carlos Figueira, et al. A phase II, single-center, double-blind, randomized placebo-controlled trial to explore the efficacy and safety of intravenous melatonin in patients with COVID-19 admitted to the intensive care unit (MelCOVID study): a structured summary of a study protocol for a randomized controlled trial. EU Clinical Trials Register. Date of trial registration: 10 July 2020. URL: https://www.clinicaltrialsregister.eu/ctr-search/trial/2020-001808-42/ES.
Phua J, Ngerng W, See K, et al. Characteristics and outcomes of culture-negative versus culture-positive severe sepsis. Crit Care. (2013) 17:202.
Qin C, Zhou L, Hu Z, et al. Dysregulation of immune response in patients with COVID-19 in Wuhan, China. Clin Infect. (2020) 10.248.
Reinhart Konrad, Daniels Ron, Kissoon Niranjan, Machado Flavia R, Schachter Raymond D, Finfer Simon. Recognizing Sepsis as a Global Health Priority – A WHO Resolution. N Engl J Med. (2017) 377:414–7.
Singer M, Deutschman CS, Seymour CW, et al. The Third International Consensus definitions for sepsis and septic shock (Sepsis-3). JAMA. (2016) 315:801–10.
Slominski, A.T.; Hardeland, R.; Zmijewski, M.A.; Slominski, R.M.; Reiter, R.J.; Paus, R. Melatonin: A cutaneous perspective on its production, metabolism, and functions. J. Invest. Dermatol. (2018) 138, 490–499.
Soy, M., Keser, G., Atagündüz, P., Tabak, F., Atagündüz, I., and Kayhan, S. Cytokine storm in COVID-19: pathogenesis and overview of anti-inflammatory agents used in treatment. Clin. Rheumatol. (2020) 39, 2085–2094. doi:10.1007/s10067-020-05190-5
Steven K . Thompson. Sampling, (2012). 3: 59-60.
Varga Z, Flammer AJ, Steiger P, et al. Endothelial cell infection and endotheliitis in COVID-19. Lancet (2020) 395: 1417–1418.
Wirtz PH, Spillmann M, Bärtschi C, et al. Oral melatonin reduces blood coagulation activity: a placebo-controlled study in healthy young men. J. Pineal Res. (2008) 44 (2): 127–133.
Worldometer. COVID-19 Coronavirus Pandemic. Available at:https://www.worldometers.info/coronavirus/. Accessed 1 June 2021.
Wu R, Wang L, Kuo H-CD, et al. An update on current therapeutic drugs treating COVID-19. Curr Pharmacol Reports. (2020) 6:56-70.
Zhang R, Wang X, Ni L, et al. COVID-19: Melatonin as a potential adjuvant treatment. Life Sci. (2020) 117583.
Zhou F, Yu T, Du R, Fan G, Liu Y, Liu Z, Xiang J, Wang Y, Song B, Gu X, et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: a retrospective cohort study. Lancet. (2020) 395(10229):1054-62.
© 2021 The Authors. Published by Elsevier Ltd on behalf of International Society for Infectious Diseases.
https://www.sciencedirect.com/science/article/pii/S1201971221007980
Copyright © 2021 Elsevier B.V. or its licensors or contributors. ScienceDirect ® is a registered trademark of Elsevier B.V.
ScienceDirect ® is a registered trademark of Elsevier B.V.

I was interested to see that there had been a trial using melatonin to treat several illness in patients diagnosed with SARS-COVID-2 and I am now more interested in finding out more about the trial for example I see no notes to suggest that these patients had received one or more or none of the SARS-COVID-2 “vaccines” which are still in trial so that is my first observation. It is interesting to note that the study only included those “infected” with the “virus” and not those who had received any “vaccines”. Is there an explanation for this which could help with the process of reviewing the study? To my knowledge there are now many reports worldwide of high numbers of adverse events (reactions) to the vaccines and a high number of deaths. Will these also be part of a clinical study using melatonin?? I am concerned that many nations (or most) have outlawed (banned) the use of effective early treatments, do the research team have any comments? Yet here is a study where melatonin study/trial commenced with the approval of the Iraqui Government one can only assume. Have there been studies using these effective early treatments like Ivermectin but also using homeopathic or nutritional supplementation that you are aware, in the effort to avoid unnecessary suffering and death? To my knowledge Australia has only outlawed and banned any such early treatments in favour of the vaccination and censors all opposing expert opinion. Regards S Turvey Australia