
Farhana Nakhooda,Tebogo Tsele-Tebakang
ABSTRACT
Background:Constipation is the most common gastro-intestinal complaint for which patients seek therapeutic intervention, affecting 2.5-79% of the global population. The effects of constipation compound from impacting on the person’s physical health to affecting their moods and influencing their quality of life. Most conventional treatments strive to treat only local symptoms and do not address concomitant symptoms of constipation.There exists a 50% dissatisfaction with the traditional approach of using laxatives.Homeopathic remedies are commonly used in managing patients with constipation (Homeopathy for Constipation), however research studies on the efficacy of individualised homeopathic treatment for constipation are scarce.
Objective: The study intended to determine the efficacy of individualised homeopathic treatment of chronic constipation.
Design:This was a descriptive study, using ten case studies, conducted over a six-week period.
Setting: The study was conducted at the University of Johannesburg Homeopathy Health Training Centre, Johannesburg, South Africa.
Participants: Through purposive sampling, ten males and females, aged 18-50 years who met the Rome II criteria participated in the study.
Interventions: A selection questionnaire confirming the participant’s constipation status was completed. The participants then had their full case history taken and physical examination performed.Each case was repertorised using Mercurius Repertorisation Software version 5.2.1.0. The participants were given the individualised remedy.
Results: The study indicated an improvement in stool frequency and general wellbeing for all ten participants, and an improvement in stool form and ease of evacuation for the majority of the participants.
Conclusions:These results support previous findings which suggest that, when an individualised homeopathic approach is correctly applied it is an effective approach for the management of chronic conditions.
Keywords:Homeopathy, Constipation, Repertorisation, Individualised treatment.
Introduction
Constipation is the term described as either infrequent bowel movements, difficult evacuation of stool, hard stool or a sensation of incomplete defecation.1The Rome II criteria is the current standard used to define and determine the presence of constipation. To meet this criterion a person must have experienced two of the following for at least three months: a bowel evacuation of three or less times per week, symptoms of straining, hardened stool, or incomplete bowel evacuation for at least 25% of the time.1Statistics show that constipation affects between 2.5-79% of the adult population worldwide2and is associated with large expenses of diagnostic testing, prescription and non-prescription laxatives.3Developing countries, with Africa in particular, have limited literature available on the prevalence of constipation. Available figures for South Africa show a 29.2% prevalence of constipation. However, due to the nature of the study4 from which this percentage was obtained, it cannot be generalised to the rest of the population. Statistics also show a higher incidence of constipation amongst the black ethnicity, lower income households, overweight and inactive individuals, females and those who received a lower level of formal education.4 As such the possibility of a high prevalence of constipation amongst the South African population is probable.5Current patient satisfaction levels with the standard available treatment strategies are only partially favourable.5 A survey conducted on chronic constipation sufferers indicates that around 47% of participants were dissatisfied with their current constipation treatment; 50% felt that fibre intake did not relieve their constipation, 44% felt that over-the-counter laxatives did not relieve their constipation and 50% felt that prescription laxatives did not relieve their constipation.6 Approximately half the group felt that their constipation treatment did not relieve the multiple symptoms of constipation and were generally disappointed in the ability of current constipation treatments to improve their quality of life.6
Homeopathyis a practice that acknowledges the fact that every individual is unique. It utilises a holistic approach in its therapeutic practice,aims to treat the person and not the disease and so treatment is not based on expectation of pathologically derived signs and symptoms, but rather according to the patient’s unique way of experiencing the disharmony, this being the unique complaint picture they present with.7,8 Individualised homeopathic treatment is an approach where a detailed case history that focuses on the totality of symptoms (physical, mental and emotional) is collected and matched with the suitable remedy.Case-taking is a unique interview process which establishes the purpose of the consultation and the goal of treatment. It is essential in gathering reliable and complete symptoms that will serve in selecting the individualised remedy after analysis of the case. 10,9,8As part of the case taking, the patient’s general and emotional wellbeing, and their medical and family history are also examined. General symptoms including the patient’s energy levels, sleep, appetite, food peculiarities, body temperature, perspiration and menstrual history are also explored. The patient’s mental and emotional symptoms are elicited by asking about their memory, dreams, fears, emotional state and their reaction to different stressful situations. Establishing all these details provides a picture of the patient as a whole and helps to individualise the case.10,9,8A physical examination as part of the case taking, is performed and a medical diagnosis is made. However, the medical diagnosis only serves to determine the severity of the pathology and prognosis of the case, rather than being a deciding factor for the remedy selection. 10,7 After the case has been taken it is then analysed and repertorised using a repertory which is an index of systematically arranged symptoms cross-referenced to their corresponding homeopathic remedies. This process identifies indicated remedies and grades them according to their appropriateness for each of the symptoms.10,9,7The single remedy method is central to the individualised approach of applying homeopathy. Potency, dosage and frequency of the prescriptions are also tailored to the individual. Homeopathic medicines are prepared through a process of successive serial dilutions and succussions (vigorous shaking). Centesimal potencies (c/cH) are diluted in a 1:100 ratio, where 1 part of the remedy is added to 99 parts of alcohol and water. To create a 30 CH potency, one part of a 29 cH homeopathic remedy is added to 99 parts of alcohol, and then succussed to create a 30cH potency, a30cH implies that the remedy has undergone serial dilutions 30 times.10Previous research studies using a homeopathic treatment have shown variable levels of effectiveness11,12 and indicate that further research studies need to be conducted on individualised homeopathic treatment for chronic constipation to more fully explore its effectiveness in treating patients with chronic constipation.
Methods
The research took the form of case studies conducted over a six-week period at the University of Johannesburg Homeopathy Health Training Centre.The aim of this study was to determine the efficacy of individualised homeopathic treatment on chronic constipation in adults using case studies, an adapted Bowel function diary with Ease and Comfort scale and the Bristol stool form scale.
Participants
The sample was set at ten participants of either gender, between the ages of 18 to 50 years,who met the Rome II criteria for constipation. Participants were recruited using non-probability convenient sampling by means of advertisements. The study consisted of four consultations per participant over a six week period. Individuals who responded to the advertisement were provided with a patient information form pertaining to the study, and after they had agreed to participate, were requested to sign a consent form. At the initial meeting a comprehensive case history was taken followed by a physical-screening examination by the researcher. The current study was granted permission by the University of Johannesburg Faculty of Health Sciences Higher Degrees Committee (HDC01-62-2014) and Ethical Clearance (AEC01-63-2014). All participants were assured of privacy, confidentiality, and anonymity, with the right to withdraw from the study at any time and signed a consent form for research publication.
Procedure
This study was a descriptive study, using ten case studies conducted over a six-week period. A Selection Questionnaire confirming the constipation status of the participants was completed to see whether they meet the inclusion criteria according to the Rome II criteria. Patient information leaflet and consent form were signed by the participants. The participants then had their full case history taken and a physical examination was performed. Participants had to attend three follow-up consultations at two week intervals. The details obtained were recorded according to the format of the homeopathic Case Taking Form. The characteristic symptoms from the case were identified and analysed by repertorisation using the Mercurius Repertorisation Software version 5.2.1.0. 13The initial potency and frequency of the remedy was standardised to 30cH, 10 drops taken once daily in order to ensure uniformity. The participants were requested to monitor each defecation session and to record the frequency of defecation, the stool form according to Bristol stool form scale and the level of difficulty on passing a stool using Ease and Comfort scale within a Bowel Function Diary. The participants were advised not to make any alterations to their usual diet or any lifestyle changes that could affect their bowel habits. At each follow-up consultation, the participant’s case was re-evaluated with special attention made to changes in symptoms or the appearance of new symptoms. Depending on the participants’ response to the initial prescription, the remedy or potency was either changed or continued.
Intervention
A single homeopathic remedy best suited the participant was administered in accordance with classical prescribing, where only a single remedy is prescribed. The initial potency and frequency of the remedy was standardised to 30cH, 10 drops taken once daily in order to ensure uniformity.Depending on the participants’ response to the initial prescription, the remedy was either continued, the potency changed or a new remedy selected. Each participant was given an explanation and a demonstration on how to take the remedy and a set of written instructions was also provided.The remedies were manufactured by CoMED Health (Pretoria, Gauteng, South Africa), a homoeopathic company that manufacture medicines according to the good manufacturing practices (GMP) and quality control.
Outcome Measures
Bristol Stool Form scale and Ease and Comfort scale as the component of the Bowel Function diary were utilised as the secondary outcome measures.
The Bowel Function Diary is a daily record of factors relating to defecation. For the purpose of this study only two of the items were monitored, this being the number of bowel movements and the associated ease or difficulty of defecation. It demonstrates an acceptable test-retest reliability and supported validity for each item, with a p-value of <0.001, and thus concluded that items from the Bowel Function Diary are a valid and reliable measure. Straining on defecation was measured using an Ease and Comfort scale.14
The Bristol Stool Form Scale is a seven score visual scale to measure stool consistency. It is a reliable and valid measure, and can be effectively used with participants over the age of eight for research purposes.14
Statistical Analysis
Data collection was in the form of case studies. A full case history was taken at each consultation in order to monitor all aspects of the participants’ progression to treatment. There after a qualitative data was gained and these were analysed for case management and described in written case studies. In addition, quantifiable data was collected by means of a Bowel Diary that was provided to the participants at each consultation. The participants used the Bowel Function Diary to record their bowel movement frequency and to monitor severity of associated symptoms. Details regarding the stool itself was evaluated using the Bristol Stool Form scale, whilst straining on defecation was measured using an Ease and Comfort scale.These results were then represented in the form of graphs. No statistical analysis was performed due to the qualitative nature of the study and the small sample size.
RESULTS
The study was a descriptive study, using ten individualised cases of homeopathic treatment. Even though ten cases were utilized in this study only three cases will be discussed and analysed and the summary of the other seven cases will be discussed in the discussion section.Repertorisation for all ten cases was analysed using Mercurius Repertorisation Software version 5.2.1.0.13
Case 1
First Consultation: An Indian female age 44 presented with constipation that started during her matric year, during which her parents also went through a divorce. She reported having only one bowel movement weekly with great difficulty. The stools were hard in consistency, required much straining and accompanied by abdominal cramps. There were burning pain at the anus after passing a stool and occasionally some blood. The constipation was worse during her menses. The participant explained that she was usually a very active person but lately she was tired all the time, had no energy, felt weak and sluggish, and yawning throughout the day. She was a light sleeper, waking up at slight disturbances and finding it difficult to fall asleep again. She described herself as being warm-blooded and requiring fresh air. In hot weather she experienced throbbing headaches and at change of season her sinuses would be aggravated. She had adopted a healthier diet recently, preferred salty taste and although not a thirsty person would drink two litres of water daily knowing that it is good for the health. She also has recurrent candida albicans infection (vaginal thrush). Her menses were regular, with clotted blood and no associated pains, but she would become very irritable and easily upset before the onset of the menses. The participant described herself as being “quiet, shy, non-intrusive and perfectionistic”, while others may add “sweet and helpful, always willing to go the extra mile and beyond her own needs to help out”. She mentioned that she was sensitive to other people’s hardships and she cry easily.
Physical Exam: BP: 118/72 mmHg, HR: 52 bpm, RR: 16 bpm, T°: 35.7°C oral
On examination, a sharp pain scoring 3-5/10 was felt across the abdomen and a dull percussion note was elicited in the left lower abdominal quadrant with a tympanic note in the other three quadrants.
Repertorisation of case 1
| Rubric | Weight | Nat-m. | Sulph. | Mag-c. | Puls. | Sil. | Phos. | Nit-ac. | Lyc. |
| Female, menses, clotted, coagulated | 6 | 1 | 3 | 4 | 4 | 1 | 4 | 3 | |
| Generalities, air, open, desires | 6 | 3 | 4 | 3 | 4 | 1 | 4 | ||
| Generalities, food and drinks, cold, drinks, water, aversion | 18 | 1 | 1 | 1 | 2 | 1 | 1 | ||
| Mind, horrible things, sad stories affect profoundly, agg. | 6 | 4 | 3 | 4 | 3 | 3 | 3 | 3 | |
| Mind, weeping, tearful mood, easily | 12 | 3 | 4 | 1 | 3 | 1 | |||
| Rectum, pain, burning, stool, after, hard | 21 | 3 | 3 | 1 | 4 | 1 | 1 | 1 | |
| Sleep, falling asleep, difficult, waking, after | 24 | 3 | 1 | 3 | 3 | ||||
| Sleep, light | 9 | 1 | 4 | 3 | 3 | 1 | 3 | ||
| Sleep, yawning, frequent | 7 | 4 | 4 | 3 | 3 | 1 | 3 | 1 | 4 |
| Stool, hard, stony | 25 | 1 | 3 | 1 | |||||
| Value | 198 | 175 | 175 | 149 | 137 | 134 | 133 | 132 | |
| Percentage | 100 | 88 | 88 | 75 | 69 | 68 | 67 | 67 | |
Prescription: Natrium muriaticum30cH, 10 drops taken once daily.
First Follow-up: The participant responded positively in the preceding two weeks. She experienced an increase in the frequency of bowel movements (five times per week from one per week), the stools were still hard and difficult to pass, the concomitant abdominal cramps and bloating had reduced and there was no more burning at the anus. There was an improvement in her energy levels and sleep.The headaches as well as the candida albicans infection were not as prominent as before. She experienced coryza which indicates a progression in the direction of Hering’s Law of Cure which states symptoms get relieved from inside outwards8. Natrium muriaticum30cH was repeated, 10 drops taken once daily.
Second Follow-up:The participant continued to show a positive response. Both bowel movement frequency and ease of evacuation had improved further and no abdominal cramping was reported. She had eight bowel movements over the past two-weeks. The stools were much softer and passed without any straining. The coryza had ameliorated. For her menses,both the blood and flow were lighter, she had no clots and no premenstrual symptoms were experienced. The patient continued with the remedy, same potency and frequency.
Third Follow-up: The frequency had increased to ten bowel movements during the past two weeks. The stool form and ease of evacuation were still optimal.
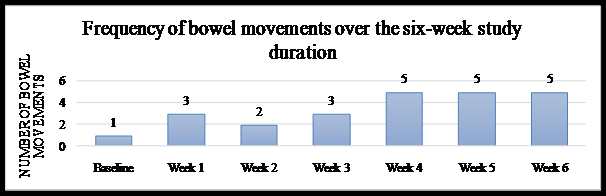
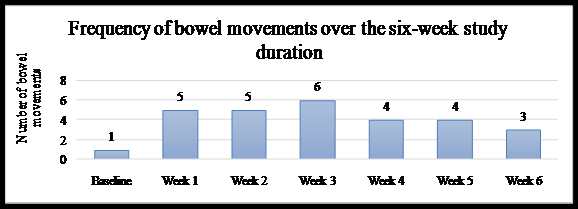
Overview of case 1: The participant showed improvement from the onset of treatment. Although it was less obvious to her in the early stages as she was looking for changes in her stools only, on assessing all her previously mentioned symptoms she became aware of the positive impact that the remedy had on her general wellbeing. Her sleep, energy levels and frequency of headaches had responded favourably from the start of treatment. Although her sinusitis was initially aggravated, it resolved completely from the third week of treatment. The frequency of her bowel movements had gradually increased over the six weeks, such that by the end of the study she was having five bowel movements weekly as compared to one bowel movement a week before participating in the study. The physical symptoms were all addressed. The participant declared herself cured of constipation as well as having an improved state of wellbeing.
Figure 1: Stool Frequency for case 1
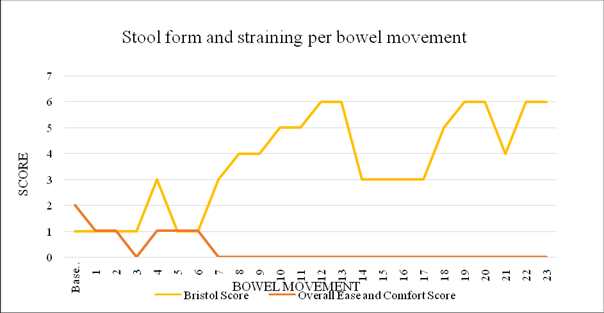
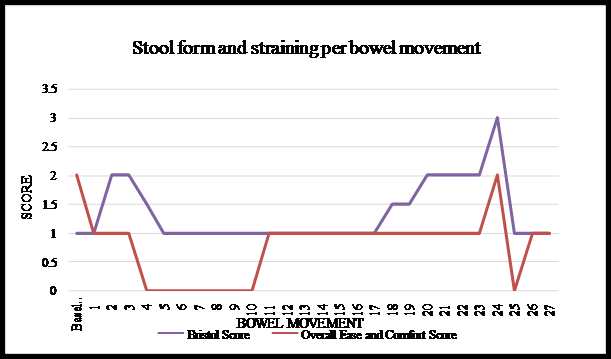
Graph 1: Stool Form and Ease of evacuationfor case 1
As treatment progressed the stools had become softer, from a baseline score of 1 (separate hard lumps) they had improved to a score of 4-6 (soft and smooth to mushy). The straining had decreased from a score of 2 (straining throughout the bowel movement) to a score of 0 (no straining).
Case 2
First Consultation: A 21-year-old black female student had constipation for the last four years. Her stools were very hard and dry, with excessive pain and straining throughout the bowel movement. The pain started at the rectum then extended to the entire abdomen and back and was sharp and labour-like with a score of 9/10 in intensity. It was exacerbated by straining and getting up from the toilet seat. She had a bowel movement twice a week on average, with very little stool passed each time. The constipation was worse the week before and during her menses. She experienced much bloating before her menses and a constant thirst not relieved by drinking water. She was a chilly person but preferred the cold as her eczema would flare-up when it was hot. She had no daytime appetite, only able to eat around 10am and would feel constantly thirsty. She had difficulty on initiating sleep, this being ascribed to thinking a lot due to stress from her studies. Her menses appeared monthly although occasionally she skipped a month. It was short, lasting 2-3 days with severe cramping pains around her abdomen, back and into her legs. She described herself as a friendly person who was always happy and rarely angry. She cried easily, preferring to be by herself when crying and feeling better afterwards. She would get easily irritated at little things, especially before her menses or when under much stress.
Physical Exam: BP: 114/86 mmHg, HR: 64 bpm, RR: 16 bpm, T°: 35.5°C oral
On examination of the abdomen, hardness was felt around the umbilicus and in both lower quadrants. There were also sharp pains felt around the umbilicus and in the right upper quadrant with tenderness in the right lower quadrant on deep palpation. The right lower quadrant was dull on percussion whereas the rest of the abdomen had a tympanic note.
Repertorisation of case 2
| Rubric | Weight | Nat-m. | Kali-c. | Sil. | Sep. | Lach. | Graph. | Sulph. | Bell. |
| Abdomen, pain, constipation, during | 24 | 1 | 1 | 1 | |||||
| Abdomen, pain, standing, agg. | 14 | 1 | 4 | 1 | 3 | 3 | |||
| Female, menses, irregular | 9 | 3 | 3 | 3 | 3 | 3 | 3 | 3 | 3 |
| Generalities, summer, agg. | 7 | 3 | 1 | 1 | 3 | 4 | 2 | 3 | 4 |
| Mind, anxiety, agg., ailments from | 4 | 3 | 3 | 4 | 4 | 3 | 4 | 4 | 4 |
| Mind, cheerfulness | 3 | 4 | 1 | 3 | 3 | 4 | 4 | 4 | 4 |
| Mind, weeping, tearful mood, easily | 12 | 3 | 1 | 3 | 1 | 3 | |||
| Rectum, constipation, menses, before | 23 | 1 | 4 | 4 | 3 | 3 | 1 | ||
| Rectum, constipation, menses, during | 18 | 4 | 4 | 4 | 4 | 1 | 4 | 1 | 1 |
| Respiration, asthmatic, summer, agg. | 28 | ||||||||
| Skin, summer, agg. | 29 | 1 | 1 | 1 | |||||
| Stomach, appetite, diminished, morning | 11 | 3 | 1 | 3 | 3 | 1 | 1 | ||
| Stool, dry | 6 | 4 | 3 | 4 | 2 | 1 | 3 | 4 | 1 |
| Value | 233 | 227 | 208 | 201 | 190 | 180 | 175 | 171 | |
| Percentage | 100 | 97 | 89 | 86 | 82 | 77 | 75 | 73 | |
Prescription: Natrium muriaticum30cH, 10 drops taken once daily.
First Follow-up: A positive reaction to the remedy was apparent. Although stool frequency remained static, the stool form, ease of evacuation, completeness of bowel movement, pain and bloating all showed tremendous improvement. The stools were softer with straining only on initiating the bowel movement and no pain experienced. Her appetite improved slightly in the mornings of the first week. Improvements were not as marked in the second week. As such, and seeing that the stool frequency was static, the researcher decided to increase the potency of the same remedy as higher potency would have a deeper action and stimulate a more lasting improvement. Natrium muriaticum200cH was given, 10 drops taken once daily.
Second Follow-up: The symptoms of constipation were much improved and a remarkable effect was seen on the menses. Mentally she was much better and felt that she able to cope better with stress. She had four bowel movements in week three and two in week four. She claimed to no longer being constipated as the stools were soft and lumpy, and no pain, straining or bloating was experienced. Her menses were painless, without clots and none of the usual moodiness or irritability that came beforehand. Although a continued improvement was apparent, there was a similar trend of the positive effects wearing off during the latter week. As such it was decided to increase the frequency of the prescription in order to obtain a sustained improvement. Natrium muriaticum200cH, 10 drops taken twice daily.
Third Follow-up: A continued improvement was observed in both the constipation and her general wellbeing. Her bowel movement frequency had increased to seven during week five and four times in week six.
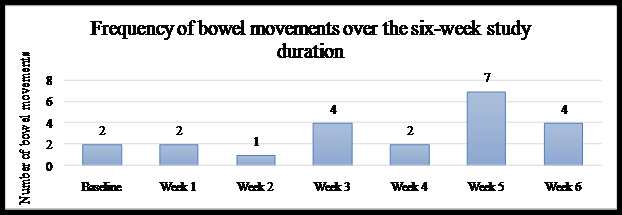
Overview of case 2: The participant showed marked improvement on all levels as seen in the presentation of her constipation as well as her general wellbeing. Her menses presentation exhibited a remarkable improvement,with no premenstrual symptoms occurring and no dysmenorrhoea. Her appetite, energy levels and her stress tolerance and coping abilities had also improved.However, throughout the entire study duration it was noted that although she responded well to the prescription, the effects would fade slightly in the course of the second week. This was notable in the frequency of bowel movements following the increase of the potency or frequency at the follow-up consultations, that the number of bowel movements would increase dramatically and only to decline in the following week. This could have been due to the fact that the dosage of the remedy was not sufficient for her vital force in order for the curative effects to hold entirely.
Figure 2: Stool Frequency for case 2
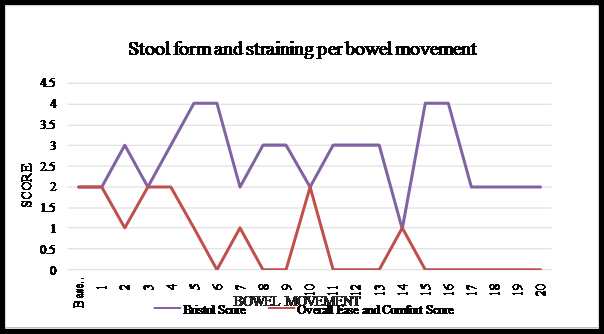
Graph 2: Stool Form and Ease of evacuation for case 2
As treatment progressed the stools became softer, from a baseline score of 2 (hard lumps) it improved to scores of 3-4 (neither hard nor soft but firm). The last few bowel movements scored a 2 again (hard lumps). The straining decreased from a score of 2 (straining throughout the bowel movement) to scoring 0 (no straining). Although hard stools were passed at the end, these were without any straining, pain or discomfort.
Case 3
First Consultation: A 21-year-old black female student had been suffering with constipation since infancy. She passed stool once or twice a week. The stools appeared as small balls of a dark brown colour and were very hard, making it difficult to expel even with much straining throughout the bowel movement. She had painful burning fissures at the anus. As a result of the constipation she had felt tired all the time. If she had not passed stool on a day, she would experience a headache as if her temples were being pushed together and a cold pain sensation at the bridge of her nose. During cold weather, she would experience a needle-like pain up the rectum. The constipation was aggravated by eating pap, and was slightly ameliorated by drinking warm lemon water or tea. Her appetite was small and she could not eat much. She craved lemon and was often thirsty. Her menses were regular with severe dysmenorrhea scoring a 15/10 in intensity. She would take Ibuprofen analgesic tablets, as without it the pains would radiate to her back and legs. She added that walking, cold weather or cold food and drinks, aggravated the pain; whilst warmth, pressure and sleeping ameliorated her symptoms. She was a chilly person and sensitive to windy weather as it would bring about her typical headache. She enjoyed sleeping and was a deep sleeper, however at night she would become very hot and broke out in a sour perspiration over her torso, waking up drenched. She described herself as happy but sensitive and disliked rude jokes. She was under much stress from her studies and was anxious about passing the year.
Physical Exam: BP: 120/84 mmHg, HR: 76 bpm, RR: 20 bpm, T°: 36.5°C oral
On examining the abdomen both lower quadrants were firm. There was no tenderness or pain on palpation. The left lower quadrant was dull on percussion while the rest of the abdomen had a tympanic note.
Repertorisation of case 3
| Rubric | Weight | Merc. | Sulph. | Hep. | Kali-c. | Rhus-t. | Sil. | Bry. | Sep. |
| Generalities, food and drinks, sour, acid, desires | 7 | 3 | 4 | 3 | 1 | 3 | 3 | ||
| Generalities, food and drinks, water, desires | 20 | 1 | 3 | ||||||
| Generalities, weather, cold, dry, agg. | 9 | 1 | 1 | 4 | 4 | 3 | 3 | 3 | 1 |
| Head, pain, headache, pressing, temples | 4 | 3 | 4 | 3 | 4 | 4 | 3 | 3 | 1 |
| Head, pain, headache, wind, storm, agg. | 15 | 1 | 4 | 3 | 4 | 4 | 2 | 3 | |
| Mind, music, amel. | 17 | 1 | 1 | ||||||
| Perspiration, sour odor, night | 21 | 4 | 3 | 4 | 3 | 1 | 1 | 3 | |
| Rectum, pain, chill, during | 23 | 3 | 3 | 1 | 1 | 1 | |||
| Stomach, appetite, diminished, eating, while, little | 29 | ||||||||
| Stool, balls, small | 19 | 3 | 3 | 3 | 1 | ||||
| Value | 197 | 181 | 167 | 150 | 145.9 | 131 | 129 | 116 | |
| Percentage | 100 | 92 | 85 | 76 | 74 | 67 | 66 | 59 | |
Prescription: Mercurius solubilis30cH, 10 drops taken once daily.
First Follow-up: The participant responded well to the remedy. All aspects of her constipation improved dramatically from the beginning of the treatment. She was having five bowel movements per week as compared to passing stool once a week previously. The stools were softer and her attempts at defecation were successful, apart from the last few days. Significant improvement had occurred with regard to her dysmenorrhoea, the intensity of pain being reduced from a score of 15/10 to 6/10. Her energy levels and appetite were also better in those two weeks. However, the effect of the remedy was less dramatic towards the end of the second week. She would experience much urging but the attempts at defecation were unsuccessful and her appetite was once again poor. The patient continued with the same remedy and potency and the frequency was increased in an attempt to establish a sustained improvement. Mercurius solubilis30cH, 10 drops taken twice daily.
Second Follow-up: The treatment was progressing favourably. Bowel movement frequency was good with six and then four stools passed per week. The stools were soft and easy to pass. The participant still perspired during her sleep, but it was a bland perspiration instead of sour. She was able to focus better although under much academic pressure. She was in the fourth academic term at the time, where she was busy with assignments, semester tests and final exam preparations. During this demanding periodshe reduced her fluid intake and frequently skipped meals. This explain the straining on initiation of the bowel movement and consequent return of constipation.The participant disclosed that at the beginning of the study she had only taken the remedy in the first week as she had been very busy and had forgotten to take it during the second week. This could have explained why the improvements were not as dramatic in the second week of the study. As such, increasing the frequency of the prescription would not have been necessary. The participant was given Mercurius solubilis30cH, 10 drops taken once daily.
Third Follow-up: A deterioration was observed in the symptoms of constipation. The frequency of bowel movements had decreased since the third week of treatment, from six times in week three to only three times in week six, but still better than only one bowel movement a week that she presented with initially. Her stools had become hard again and the anal fissures had reoccurred because of the return to a hard stool. On a general level, her energy had increased and so had her appetite. The dysmenorrhoea which had decreased from 15/10 to 6/10 the previous month, had completely vanished on her last menstruation. The continued improvement in general symptoms asserted that the remedy was well indicated.
The deterioration in her presentation of constipation may have been due to the fact that she was barely eating during this period. It may have also been that the potency of the remedy was insufficient to cause a lasting effect, and as such a 200cH might have been better suited. However, as the 30cH potency had produced significant improvements, the participant was advised to continue with the same prescription for a further week in order to establish whether the remedy will ameliorate the constipation again since the stress of the examination was over and she was back to eating consistent meals.
Overview of Case 3: The participant experienced dramatic improvements in all aspects of her constipation as well as in her general wellbeing from the start of the treatment. The dysmenorrhoea had completely resolved by the end of the study. Her energy levels were enhanced and her appetite had a general improvement after some interim fluctuation. Bowel movement frequency, successful defecation attempts, stool form and ease of evacuation fluctuated slightly during the course of the research study, with the most decline occurring in the final two weeks. The anal fissures had returned in the fourth and fifth week respectively as a result of the regression in stool form and subsequent difficulty on evacuation. At the conclusion of the study the participant reported that she had passed stool almost daily, having ten bowel movements across eight of the ten days since. The stools were much softer (Bristol score of 3) with barely any straining. The anal fissures had healed, her appetite was good and she was able to eat a larger portion.
Graph 3: Stool Frequency of case 3
Graph 3: Stool Form and Ease of evacuation for case 3
The stools became increasingly softer, from a baseline score of 1 (separate hard lumps) it improved to a score of 2-3 (firm and sausage-shaped). Although the participant appointed a score of 1 (separate hard lumps) to most of the bowel movements in the second and third week of treatment, during the consultations she described the stools as being soft balls, passed easily. This description does not entirely conform to the score of 1, which is characterised by hardness of stool and difficulty in passing the stool. In the last week the stools became hard again, scoring 1 (separate hard lumps). The straining decreased from a score of 2 (straining throughout the bowel movement) to 0 (no straining) but then got worse again from week three onwards scoring a 1 (straining only at the beginning of the bowel movement).
DISCUSSION
The research comprised of ten case studies.The average age range of the participants was between 21-28 years, with two participants over the age of forty. The study sample was of asymmetric gender distribution, with a female to male ratio of 8:2.Majority of the participants were of black ethnicity (seven), with two Indians and one Caucasian.
Three of the participant’s sought intervention prior to the study due to their constipation but with limited benefit. All ten participants had previously tried various forms of management strategies, comprising either over-the-counter laxatives, herbal constipation teas, drinking hot water daily or fibre supplementation. In these cases, the management strategies mentioned above were ineffective or only offered partial and/or temporary assistance. Concomitant symptoms of pain, discomfort and bloating were not relieved. Most participants were unhappy with the results of such strategies and thus did not persevere with them. This emphasises the results found on a study that was conducted suggesting that patient satisfaction levels with many first-line management strategies for constipation are at best only partially favourable.5
Although this research study had a short duration, all ten participants expressed satisfaction with the treatment over the course of the study.Every participant claimed to have benefitted from the study, with their symptoms of constipation being partly relieved or completely resolved. Most of the participants also exhibited improvements in other aspects of their general health and expressed that they experienced an enhanced state of wellbeing. Although majority of the participants in the study were not following a particularly healthy diet, no dietary advice was given during the course of the study and participants were requested not to alter their usual diet. Even though the participants responded positively to the remedy, it does not discard the importance of correcting the diet. A poor diet encumbers optimal health and functioning, and could pose as an obstacle to cure in many health conditions.10,15
It was observed that only three of the participants adhered to the minimum recommended intake of two litres of water daily, and only four participants were engaged in some form of physical activity on a regular basis. Insufficient fluid intake and a sedentary lifestyle contribute to the incidence and severity of constipation.16 Treatment outcomes may be enhanced if these factors are addressed simultaneously.
All initial prescriptions were in the 30cH potency, with the dosage instruction of 10 drops taken once daily. This method of prescribing ensured uniformity of the initial administration of the remedy, in order to limit treatment variables. The 30cH potency was decided upon as a good balance, as it was deep acting enough to also stimulate a response on the general and mental-emotional level, whilst limiting the possibility of aggravations. Participants were instructed to continue with the remedy until the completion of the study, after which they were advised to use the remedy only as needed. The approach of a continued administration of the remedy throughout the six-week period was adopted to exclude the possibility that a lack of improvement in the symptoms of constipation could be ascribed to insufficient administration of the remedy. This method did not adhere completely to the principles of classical prescribing, which directs that if dramatic improvements are seen (as in Case 2, 3, 4, 6,7, 8 and 10) the remedy should be discontinued so as not to interfere with the curative action produced by the administered dose. A second dose should only be administered if improvements diminish and the original symptoms reappear.10It is a possibility that with regard to Case 6 and 8, the continued dosing after a dramatic improvement had occurred could have been the cause of the relapse in some symptoms.Homeopathic remedies are often considered to take a long time to work. However, it was observed that all ten participants experienced improvement within the first week of taking the remedy, with seven participants experiencing an improvement the very next day.Eight different homeopathic remedies were prescribed, demonstrating the highly individualised presentation of constipation.
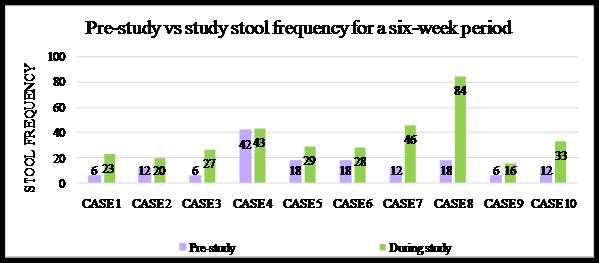
The graph below represents the stool frequency across six weeks for each participant, comparing an extrapolated pre-study frequency to the frequency during the study period. The pre-study figure was obtained by multiplying the baseline weekly figure by six to determine an expected frequency across six weeks. Case 4 is an exception, being almost on par for pre-study and during study frequency; however, with this case the participant did not refer to stool frequency but rather to stool form, ease of evacuation and completeness of evacuation.
Limitations of the study
The study duration was short and no long-term follow-ups were conducted to determine the long-term efficacy of the treatment. The sample size was small. More weight could be given to results if a larger sample was used. There was no control group to make comparison to and therefore the validity of the study is very low. As such no conclusive statements can be made.
Individualised homeopathic case studies are very time consuming, such that a larger sample creates difficulty.The Bristol Stool Form scale and Ease and Comfort scale were not sensitive enough to adequately represent ameliorations in some cases, as seen with three participants (Case 3, 5 and 8). There was limited control over external factors that could have an influence on bowel functioning. Although participants were requested not to change their diet and eating patterns or make any significant lifestyle changes, it was not always possible and such changes had an impact on the bowel movements.
CONCLUSION
Individualised Homeopathic approach treated the participants as a totality and this was witnessed with a favourable progression in participant’s psychological and physical symptoms of constipation, as well as an increased state of general wellbeing. Participants were consequently pleased with the improvements that had occurred.
Acknowledgements: The authors would like to thank the researcher for conducting case histories.
Authors’ Disclosure Statement: The current study was financed by the University of Johannesburg (UJ). The contents of the work are solely the responsibility of the authors and do not represent the official views of UJ. The authors have no conflicts of interest related to the study.
REFERENCES
- Longmore, M. Oxford handbook of clinical medicine, Oxford University Press, Oxford, UK. 2012:248-249, 276, 630.
- MugieSM, Benninga MA, Di Lorenzo C. Epidemiology of Constipation in Children and Adults: A Systematic Review, Best Practice & Research Clinical Gastroenterology; 2011, 25:3-18.
- Wald, A. Constipation. JAMA, 315(2), 2016.p.185.
- Meiring PJ, Joubert G. Constipation in Elderly Patients Attending a Polyclinic,South African Medical Journal; 1998, 88(7):888-890.
- Statistics South Africa. Social Profile of South Africa, Stats SA, Website: http://www.statssa.gov.za/publications/Report-03-19-00/Report-03-19-002009.pdf, Accessed September 2015.
- Johansen JF, Kralstein J. Chronic Constipation: A Survey of the Patient Perspective,Alimentary Pharmacology & Therapeutics; 2007, 25(5): 599-608.
- Jayasuriya A. A to Z homeopathy, B Jain Publishers, New Delhi, India; 2010:5-13, 24-25, 35-48, 59, 710, 713, 784-786
- Vithoulkas G. The science of homeopathy, Grove Press, New York; 1980:13-21, 92-98, 120-121, 169-182, 213-232
- Roberts E. Homeopathy: Principles and Practice, Winter Press, UK; 2005: 35-52, 94-103, 107-120
- De Schepper L. Classical homeopathy for the professional, B Jain Publishers, New Delhi; 2010:26-43, 56-87, 112-141, 169-190, 286-304.
- Sabath L. A Study to Determine the Efficacy of the Homeopathic Similimum in LM Potency in the treatment of Constipation in Adults, Faculty of Health Sciences, Technikon Witwatersrand, Johannesburg, South Africa; 2005.
- Ramguthy A.Efficacy of the Homeopathic Complex Remedy, Constipation 6c on the Symptoms of Functional Chronic Constipation in Females, Faculty of Health Sciences, University of Johannesburg, South Africa; 2010.
- Van Zandvoort R. Complete Repertory, Mercurius homeopathic software, version 5.2.1.0. (Computer software), Aeon Group; 2009.
- Camilleri M, Rothman M, Ho KF,EtropolskiM. Validation of a Bowel Function Diary for Assessing Opioid-Induced Constipation. American Journal Gastroenterology; 2011, 106(3):497-506.
- Caruso H. Your drug-free guide to digestive health, Library and Archives Canada Cataloguing in Publication, Canada; 2008:86-96.
- McCance K, Huether S, Brashers V, Rote N. Pathophysiology 7th edition, Elsevier, UK;2010:1424-1425



DEAR SIR,
IT IS NEW TO ME THAT A DOSE OF POTENTIATED, REMEDY 30C /200C CONSISTS OF 10 DROPS . I HAVE BEEN ADMINISTERING ONE DROP AS ONE DOSE [EXCEPT Q] WITH CORRECT RESULTS. I AM AFRAID 10 DROPS MAY SOON GIVE AGGRAVATION PARTICULARLY WHEN THE REMEDY IS NOT SIMILAR. MOREOVER IF THE REMEDY IS FROM TERRIBLE POISON MAY PROVE DANGEROUS IN SUCH QUANTITY? PL ENLIGHTEN ME
THANKS
[email protected]