
Seema Mahesh1, 2, Mahesh Mallappa2, Olga Habchi3, Vasiliki Konstanta4, Cristina Chise5, Panagiota Sykiotou6, George Vithoulkas7, 8
First Published February 11, 2021 Case Report
https://doi.org/10.1177/1179547621994103
Article Information
Volume: 14
Article first published online: February 11, 2021; Issue published: January 1, 2021
Received: November 06, 2020; Accepted: January 18, 2021
1School of Medicine, Faculty of Health and Medical Sciences, Taylor’s University, Subang Jaya, Malaysia
2Centre for Classical Homeopathy, Bangalore, India
3The Modern Medical Consultation Centre, Dubai, UAE
4Homeopathic Centre of Classical Homeopathy, Athens, Greece
5Arizona Homeopathy, Phoenix, AZ, USA
6Homeopathic Centre of Classical Homeopathy, Athens, Greece
7Postgraduate Doctors’ Training Institute, Health Care Ministry of the Chuvash Republic, Cheboksary, Russian Federation
8International Academy of Classical Homeopathy, Alonissos, Greece
Corresponding Author:
Seema Mahesh, School of Medicine, Faculty of Health and Medical Sciences, Taylor’s University, 1 Jalan Taylors, 47500 Subang Jaya, Selangor, Malaysia. Email: [email protected]
article is distributed under the terms of the Creative Commons Attribution-Non Commercial 4.0 License (https://creativecommons.org/licenses/by-nc/4.0/) which permits non-commercial use, reproduction and distribution of the work without further permission provided the original work is attributed as specified on the SAGE and Open Access pages (https://us.sagepub.com/en-us/nam/open-access-at-sage).
Abstract
The Continuum theory and the Levels of Health theory propound the idea that return of efficient acute inflammation (high fever) heralds true improvement in chronic inflammatory states. We present 6 cases of atopic dermatitis (AD), which had stability in their improvement for 1 year or more, under classical homeopathy. The cases were retrospectively assessed with selected based on the Hanifin Rajka atopic dermatitis diagnostic criteria and the follow ups evaluated according to changes on SCORing Atopic Dermatitis scale (SCORAD) scale. The pictures are presented as evidence. Modified Naranjo Criteria for assessing causal attribution of clinical outcome to homeopathic intervention was used to assess the effect of homeopathy in these cases. All the cases improved and stabilised with complete skin clearance (those that relapsed within 1 year were not included). These patients had not suffered high fevers/acute inflammatory diseases since onset/aggravation of AD. Five of the 6 cases developed acute inflammatory diseases as the chronic condition improved. The last case showed return of an old, lesser pathology. The control cases – which were selected for non-improvement under classical homeopathy also showed remarkable skin clearance when there was appearance of acute inflammatory states. In this study, there is a mutually exclusive relationship between efficient acute inflammation and chronic inflammation, which is in accordance with the 2 theories considered here. Further scientific studies are necessary to establish the phenomenon at tissue level.
Keywords Atopic dermatitis, eczema, homeopathy, inflammation
Background
The idea that onset of chronic inflammatory disease implies the absence of efficient acute immune response was propounded by Vithoulkas and Carlino.1 The theory also proposed that when under classical homeopathic therapy, as the chronic inflammatory condition improves, the ability of the organism to mount an efficient acute inflammatory response to pathogenic stimulus returns; and this is a tangible clinical phenomenon confirming the stable improvement in the chronic disease in question.
This study aimed to explore if such a correlation was indeed possible to appreciate in real world scenarios by inspecting atopic dermatitis (AD) cases. The inclusion criteria for this study was – stability in improvement of atopic dermatitis for at least 1 year post classical homeopathic treatment.
Atopic Dermatitis (AD) is a chronic inflammatory disease,2 affecting over 20% children and 3% adults globally.3 Many times, it is the first step in the march of allergic conditions (food allergy, asthma, allergic rhinitis, allergic conjunctivitis and eosinophilic esophagitis).3 It usually runs a chronic relapsing course and is only controlled but not cured by conventional therapy.3,4 Latest research shows that atopy represents systemic involvement and is not restricted to the cutaneous affection alone. Various co-morbidities (cardiovascular, neuropsychiatric, malignancies, etc.) associated with AD seem to confirm the systemic affection.5 Management wise, the control of itch is especially challenging in these cases despite many therapeutic solutions offered. The mast cells that are responsible for the initiation and amplification of allergic response, release many pruritogens. Classically, histamine was thought to produce the sense of itch through its receptors on sensory neurons and H1 anti histamines were applied for control of AD related itch. However, this has been disappointing clinically. Recent studies have revealed the role of interleukins released by mast cells, in the generation of itch in AD and novel therapeutic strategies involving blocking these interleukins are being developed.6–8
Further, studies have shown that though there is evidence of AD individuals being sensitised to allergens, over 20% of them are not, to any allergen whatsoever. This implies that the disease has varied phenotypes and there is a need to tailor the treatment to every individual’s genetic and phenotypic make up.4 Researchers agree that AD is the result of an allergic constitution and this tendency to allergy needs to be addressed.3
In classical homeopathy, a patient’s complete hereditary attributes and phenotypic presentation (peculiar symptomatic presentation) is studied in detail and the medicine selected is individualised to the highest degree clinically possible.9 There have been reports demonstrating similar possibilities in other dermatological pathologies such as vitiligo.10
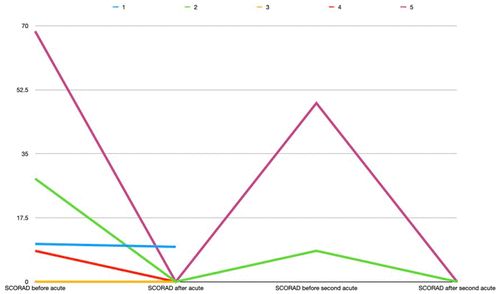
We conducted a retrospective analysis of AD cases from clinical records which are presented here as a series of 6 cases diagnosed with AD, reconfirmed by retrospectively plotting against the Hanifin Rajka criteria for atopic dermatitis. They had all stabilised for a year or more under individualised classical homeopathic treatment. The results were assessed on the SCORing Atopic Dermatitis scale (SCORAD)11 (Figure 1). In the end, the cases were assessed for development of any acute inflammatory diseases and their correlation to the SCORAD, indicative of the chronic inflammatory disease in question here (Figure 2).
Figure 1. SCORAD graph of all the cases.
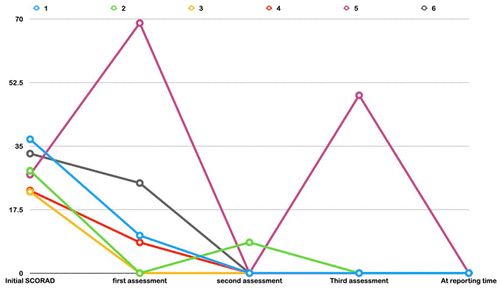
Figure 2. Correlation of acute disease with SCORAD.
In order to test if it holds good for every acute inflammation, we assessed the same association in cases that were not improving under homeopathic treatment.
The aim of this study was to examine if there is a relationship between onset of efficient acute inflammation and improvement in the chronic inflammatory conditions (in this case, AD), from the real-world scenarios.
Case Series
The case series involved 6 patients under classical homeopathic treatment. The inclusion criterion was, remission of AD for 1 year or more after cessation of treatment. Table 1 gives the details of the patient characteristics. The patients’ age ranged from 3 months to 39 years. One of them was male. The diagnosis of AD was retrospectively confirmed using the Hanifin-Rajka criteria12 (Table 2). None of these patients were using any pharmacological agent for their condition at the time of consultation or during follow ups. None of them developed any adverse reactions during treatment. The severity of AD was assessed using the SCORAD scale and their progress was recorded accordingly (Figures 3-8). Where the clinical scores were not assessed during consultation, it was assessed retrospectively according to the detailed clinical record description and photographs.
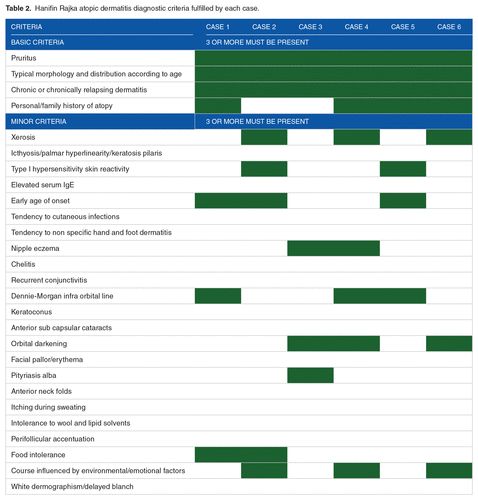

Figure 3. Case 1 evolution of atopic dermatitis under treatment.
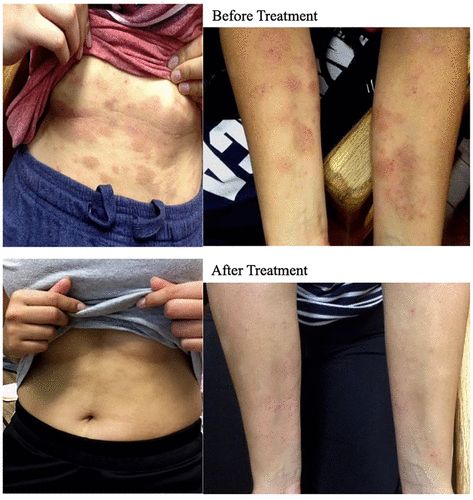
Figure 4. Case 2 evolution of atopic dermatitis under treatment.

Figure 5. Case 3 evolution of atopic dermatitis and pityriasis versicolor under treatment.

Figure 6. Case 4 evolution of atopic dermatitis under treatment – after shift to palm.

Figure 7. Case 5 evolution of atopic dermatitis under treatment.

Figure 8. Case 6 evolution of atopic dermatitis under treatment.
Case 1 (Figure 3)
A 6-moth old Greek infant was brought on 27/08/2007 with extensive AD on the face, with exfoliation, crusting and severe pruritus (SCORAD 36.8). It first appeared at the age of 3 months. The child was on exclusive breastfeed and no other complaints were apparent.
Family history: Mother had allergic reaction to cereals 5 years ago.
First prescription: The infant was prescribed Graphites 200CH 1 dose.
Follow up: 2 days later there was a slight therapeutic aggravation (an expected reaction after the medicine and not an adverse event) followed by considerable amelioration in the dermatitis from the sixth day onwards (SCORAD 10.35). When solid food was introduced at the age of 8 months the infant had a relapse and Graphites 200CH had to be repeated. The baby continued to be breast fed. Every attempt at introducing any solid food (fruit, vegetables, cereals, chicken, meat) resulted in a relapse of the AD. Calcarea carbonica 200CH was prescribed with little effect. The physician now sought to treat the mother. The physician now sought to treat the mother. While this concept needs scientific investigation, there is some evidence regarding the change in the composition of breast milk when mother is psychologically affected.13 The studies have investigated other effects of such alteration in the infant but not atopic dermatitis specifically. However, it is a widely accepted clinical phenomenon among homeopathic physicians that when the mother is affected the breast-fed child may develop any complaint – physical/psychological. Here, it turned out that the mother was in grief due to loss of a loved one (during the pregnancy of this child). Her detailed case was taken, and she was prescribed Natrum muriaticum 200CH and 1M.
This was followed by a therapeutic aggravation in the mother, where she felt an intensification of her sadness for 2 days accompanied by fever of 100.4°F, and the infant, on the fourth day of treating the mother, developed fever of 101.8°F, lasting 24 hours. The mother and baby both improved considerably hereafter (SCORAD 9.55). The AD on the face of the infant subsided and eruptions developed on the trunk (shift of skin lesions downwards is an indication of improvement according to homeopathy). The infant gradually was introduced to solid food and there was a relapse at the age of 11 months when he was introduced to egg and fish. Now the Natrum muriaticum was given to the child directly, which ameliorated the AD completely (SCORAD 0).
Outcome: The follow up at the age of 12 years, shows no allergic episodes since the last one at 11 months age (Figure 1).
Case 2 (Figure 4)
A 22-year-old American woman consulted the homeopathic physician on 11/02/2014 for AD on her face, neck, arms and abdomen (SCORAD 28.2). The eczema first appeared on her arms when she was 4 years old slowly spreading to the neck, and since previous year it spread to the face and appeared on the abdomen. At the age of 14 she was tested for food allergies and was found to be allergic to milk, wheat and gluten.
The plaques were erythematous, intensely pruritic and dry. Sometimes she scratched until it bled. The face was very dry and painful, and she had to apply lotion several times a day. She came in holding a small container of petroleum jelly and applied it on her face during the consultation.
She also had intermittent asthma, which started around the age of 7. It usually bothered her during cold. She used a rescue inhaler when affected and was not on regular medication for this.
History of past illness: She suffered recurrent tonsillitis in early childhood which were treated with antibiotics. Her father died when she was 12 years old and there was a noticeable aggravation of the eczema at that time. Last time she ran a high fever was 5 years ago at the age of 17. In the past 5 years she had some mild acutes without fever.
Family history: Her mother was thalassemia minor; father was healthy but died in a car accident at the age of 42. Both grandfathers had heart attacks, 1 grandmother had a stroke and the other dementia, both grandmothers had high blood pressure.
First prescription: Medorrhinum 200CH 1 dose.
Follow up: (Medorrhinum) brought out a fever within a couple of months after which tonsillitis became recurrent as in her childhood. Sulphur 30CH and Baryta carbonica 1M were prescribed with eventual complete remission of skin and reduction in tonsillitis episodes.
Outcome: As on 08/05/2009, the patient had been clear of AD since August 2016 (Figure 3) and had a few episodes of tonsillitis with fever which subsided on their own. She was otherwise well and happy.
Case 3 (Figure 5)
A 13-year-old Indian girl living in Dubai suffered AD of the nipples (more on the right side) for the past 4 months (SCORAD 22.4). The nipples were oozing and crusted over with intense pruritus. She also had pityriasis on the right cheek for 6 months and had amenorrhoea for the past 6 months. She first sought homeopathic consultation on 12/03/2018.
The girl had pityriasis on her face on and off for the past 10 years. She used clotrimazole cream on them whenever they appeared. She also had an episode of eczema on her lower abdomen at the age of 12 which disappeared with topical steroids. Till the age of 8 years she developed occasional acutes with high fever but since the age of 8 she did not get any acutes or fevers. She developed chickenpox at the age of 9 years and used zovirax cream at that time. She attained menarche in August 2017 and the next period was on time in September 2017. After this there was secondary amenorrhoea till the homeopathic consultation.
Family history: Mother had chronic bronchitis during pregnancy and lactation of this child and had to be put on bronchodilators and antibiotics. She had poly cystic ovarian syndrome and underwent hysterectomy at the age of 40 years. There was history of diabetes mellitus, hypertension and myocardial infarction in the grandparents.
First prescription: Graphites 6 CH in increasing dilutions every day for 3 weeks.
Follow up: 21/01/2019: The AD completely regressed, and skin became smooth within a month from Graphites 6 CH. She had regular menses till October 2018 but since then there was amenorrhoea and the pityriasis had relapsed very mildly since a few days. The girl had tremendous anxiety about the approaching final examinations. She was prescribed Carcinosinum 200CH for 3 weeks.
06/02/2019: Patient developed acute viral fever with cough, diarrhoea and vomiting with a temperature of 101.3°F (after 5 years). This subsided without any medication in 2 days. She had menses 3 weeks after the Carcinosinum and has had regular menses since then.
Outcome: The last follow up was made on 8/9/2019; the girl had been clear of AD since April 2018 (Figure 3) and the co-morbidity of pityriasis also responded well. She again developed a high fever which was absent since the age of 8 years.
Case 4 (Figure 6)
A 15-year-old Indian girl consulted the homeopath on 28/8/2013 for AD of both the breasts, popliteal fossa and face (SCORAD 22.75). She suffered this condition for the past 8 years. The lesions were dry, fissured and pruritic in general but fissured, oozing and painful in the nipples. She had to apply a bandage to the nipples in order to prevent the discharge from soaking through her clothes. She also had allergic rhinitis with sneezing in the mornings. She had dysmenorrhoea on the first 3 days of her menses. She developed high fevers with upper respiratory tract infections occasionally in early childhood but was usually treated with antibiotics and had no high fever for over 10 years now. At the age of 4 years she had developed 2 episodes of wheezing respiration and was given inhalers.
Family history: There was strong allergic tendency in the family – both parents had allergic rhinitis and paternal grandfather had asthma; maternal grandmother had suffered oesophageal cancer and maternal grandfather, prostate cancer.
First prescription: Graphites 200CH 1 dose.
Follow up: There was a therapeutic aggravation following this prescription which was followed by remission in the lesions to a considerable degree. The case however took a long time to see real change. She was prescribed Psorinum 200CH in December 2013 which kept the skin lesions at bay for over a year. Later the symptomatic picture changed again and Petroleum 200CH was required next. It was after the prescription of Natrum muriaticum 200CH in February 2015, however, that the lesions began to move distally, an important development according to the rules of homeopathy, depicting a good response to treatment. The dermatitis patches on breast, face and neck completely disappeared and the lesion began on her palm (SCORAD 8.45). This was very itchy and oozing initially but with Natrum muriaticum 200CH and later 1M this also became completely better. At this time, (December 2018) the patient developed very high fever (104°F) which she had not developed since early childhood, and on unavailability of the homeopath at that time, the patient was forced to take antibiotics. Immediately following this, the palmar dermatitis relapsed and the Natrum muriaticum 1M had to be repeated.
Outcome: Since the repetition of Natrum muriaticum 1M in December 2018, the skin has remained clear till date (SCORAD 0) (Figure 5). Her rhinitis has reduced greatly and so has the pain during menses.
Case 5 (Figure 7)
A 3-month-old Greek female infant was brought to consultation on 26/05/2009 with severe AD on her cheeks, behind the ears, on arms and legs (SCORAD 27.1). The baby started showing allergic symptoms at the age of 25 days, which did not abate with the mother avoiding allergenic food. She was then tested to be allergic to milk (cow, goat) 4+, gluten 4+, egg (yolk, white) 3+ by radioallergosorbent (RAST) test. She could not tolerate breast feed and was on special formula amino acids feed devoid of any cow milk proteins, gluten and lactose. This slightly reduced her atopic dermatitis. The mother had suffered severe anaemia and headaches during the pregnancy of this child and in the 37th week of pregnancy had to undergo blood transfusion. This was immediately followed by the foetus changing position although was already in the cephalic presentation for delivery. The mother was prescribed the homeopathic remedy pulsatilla 200CH, followed by return of the foetus to cephalic presentation and a normal delivery. The baby suffered omphalitis 3 days after birth and was given the homeopathic remedy Abrotanum 200CH which helped in reducing the infection – no other treatment was given.
Family history: The mother is allergic to propranolol, ciprofloxacin, parietaria, grass and nuts. She had laryngeal oedema by grapes at the age of 21. She also suffers chronic severe cluster headaches. The father has urticaria from peach. Her sister, 4 years old had mild atopic dermatitis from the age of 4 to 14 months.
First prescription: Astacus fluviatilis 30CH, 2 doses per day, increasing by 1 potency every week.
Follow up: The problem escalated severely when her sister inadvertently fed her a piece of apple (SCORAD 68.5) (Supplemental Video 1). This responded well to Apis mellifica 200CH. After this, however, she started having episodes of acute bronchitis with high fever which had to be treated with Kali carbonicum 200CH. Once the bronchitis went down, there was one more episode of flare up of AD (SCORAD 48.95). When this episode was treated with Psorinum 12CH, the skin cleared up completely, but she developed mild bronchitis again, followed by acute otitis media with offensive discharge from the ear. After this, the skin remained clear.
Outcome: When assessed at 3.5 years’ age, she could eat most food except fruits and vegetables. The AD did not recur. At the age of 10 years, which is the most recent assessment, she remained clear of any eruption and was mildly intolerant to fruits and vegetables. She got mild itching in throat from some fruits but could tolerate others well. Some mild itching in the throat occasionally if she ate fish (but not prawns or octopus which she tolerated well) but these pass away quickly. She was generally well and had not been given any medicine since the age of 2 years.
Case 6 (Figure 8)
Thirty-nine-year-old Indian lady presented with atopic dermatitis of left ankle, which was lichenified, fissured and intensely pruritic (SCORAD 32.9). She had developed mild eczema in the last 2 years, but it had aggravated a lot in the last 2 months. She had some mild rhinitis on exposure to dust. She was also under depression and was apathetic to everything in life. She had no significant past medical history.
Family history: Father had eczema and there was a strong heart complaints history in her uncles and first cousins.
Treatment: She was mainly treated for her depression at the beginning. Till beginning of 2015 she battled with depression and during treatment of this state there was no change appreciable in the AD. However, by beginning of 2015 she began healing on the emotional level and the skin became the focus of treatment. The SCORAD was still around 39 on 10/1/2015. She was better in her depression than before but had episodes of intense sadness and she tended to dwell constantly on past unpleasant incidents.
First prescription (for AD): Ignatia amara 200CH 3 times a day for 3 days.
Follow up:
28/03/2015: Patient was emotionally much better. No sadness or depressed feeling. Skin was better than before but not remarkably. SCORAD 24.8.
Prescription: Rhustox 200CH 1 dose.
27/06/2015: New wart appeared on left forefinger; AD eruptions were better – only itching persisted, disturbed sleep; SCORAD 9.5. The rhinitis had also reduced completely.
Prescription: Thuja occidentalis CH 1 dose.
The state of AD slowly reduced after this phase while the corns on her soles and wart on the palm were the main complaints.
24/04/2016: The eczema was completely cleared; SCORAD 0; no allergic rhinitis; emotionally patient was better.
Outcome: Patient continued to consult for the wart on the hand and the painful corns on feet.
The patient has been reporting periodically and has been followed up last on 16/08/2019 and there were no relapses of the depression, AD or rhinitis.
These cases were followed up for a considerable length of time (Table 1) and skin clearance has been stable. In each of these cases, no high fevers had occurred since onset of AD. With treatment, 4 of these cases developed high fevers from infections of various kinds before the skin clearance (SCORAD 0) was achieved (Figure 2). The acute conditions were also handled with homeopathy when treatment was warranted, otherwise, they were allowed to run while keeping a close watch. One case developed high fever after skin clearance and the last case developed old complaints that existed long before the appearance of the AD but no fever. The initial AD scores were of a wide spectrum (Figure 1; Table 1), mostly moderate AD according to Kunz et al.14 Five of the patients gave positive family history for atopy and 3 of them were tested for and diagnosed with specific allergies/atopy. All patients were treated with individualised remedies, based on their presenting symptomatology according to the principles of homeopathy. The mean initial SCORAD was 28.36 ± 5.664 and the mean SCORAD after acute infections or appearance of suppressed old complaints was 4.59 ± 5.037 (P < .0001), exhibiting a statistical significance, although the significance with such small sample may not amount to a real picture.
Control cases: (Table 2).
We compared 6 AD cases of AD that were running a chronic relapsing course as control for the occurrence of acute infectious diseases. The cases were of similar age range (3 years-36 years). Four were females and 2 were males. One of these cases did not exhibit any fevers during the follow up period and 3 exhibited occasional fever which were in the mild range (100°F-101°F) and 2 of them ever exhibited high fever (102°F-103°F). The average initial SCORAD was 14.5. The average SCORAD after fevers in these cases was 6 (Figure 9) and the final average SCORAD was 5.17 (P = .0031).
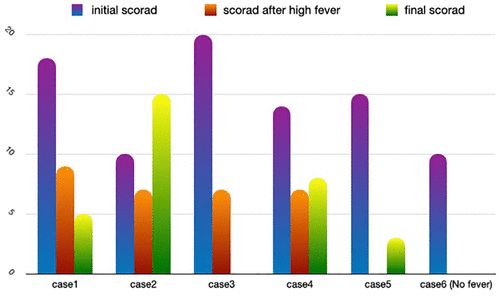
Figure 9. SCORAD changes in control cases (non-responsive AD cases).
Discussion
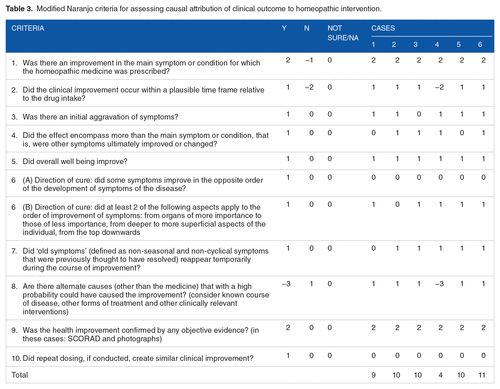
The 6 cases of AD under classical homeopathic treatment improved considerably. The effect of treatment was assessed with Modified Naranjo Criteria for assessing causal attribution of clinical outcome to homeopathic intervention15 and most of the cases had a clear causality score (Table 3). The investigators sought to assess if this was according to the continuum theory that proposes the mutual exclusivity of chronic inflammation and acute inflammatory response (high fever). In these 6 cases, the appearance of acute inflammatory conditions/fever was strongly associated with remarkable skin clearance. The control cases were selected for their non-improvement while under classical homeopathic treatment. While these cases did not exhibit stability in skin clearance over time, they too demonstrated a remarkable skin improvement associated with the appearance of acute inflammation (Figure 9). Thus, there may be grounds to investigate the relationship between absence of efficient acute inflammation and prevalence of chronic inflammatory states.
|

Table 3. Modified Naranjo criteria for assessing causal attribution of clinical outcome to homeopathic intervention.
The Levels of Health theory and The Continuum theory1,16 attempt to explain the connection between acute and chronic inflammatory conditions in the wide spectrum of health situations in the population. They propound the idea that people born with healthy immune systems, capable of efficient acute inflammatory response may, due to different stresses (including unnecessary drug treatment for fevers), drop in the level of health and enter a state of low-grade chronic inflammation; when efficient acute inflammatory response to pathogenic stimulus is no more possible. Further, under the right therapy, as the chronic inflammatory condition improves and the body begins to resolve it, the immune system is again capable of efficient acute inflammatory response. This provides a tangible way of assessing the improvement in chronic disease is by appreciating onset of high fever in response to infections. This has been corroborated by immunological studies – that disruption of acute inflammation leads to activation of the chronic17,18 and people during severe chronic inflammatory states may be incapable of reacting efficiently to pathogenic stimulus.19,20 They may not raise any reaction at all and in case the pathogen is very virulent, they may have exaggerated response, resulting in severe damage or death.21
The objective of this study was to examine if the appearance of efficient acute inflammatory condition (viz., fever) was associated with improvement in the AD, a chronic inflammatory disease. As it turns out, there was a strong association, in both the groups considered here. While tissue level studies are required to establish this phenomenon, there seems to be grounds to do so.
This study has many limitations. First of all, the remission of AD for 1 year or more was not based on any established follow up criteria for AD stability, but, based on a clinical experience that this is a good enough time period to consider. Secondly, the retrospective SCORAD was assessment may have resulted in minor differences from the actual situation. However, homeopathic case records are very descriptive and contain exhaustively detailed explanation of the symptoms, therefore the difference may be assumed to be minimal and of no consequence. Thirdly, it would have helped to test the inflammatory markers and atopy markers and correlate them at every major change in the disease. This was not possible as the cases were selected retrospectively. No control was performed in this study with either placebo or established treatment to assess if such phenomenon occurred universally. The authors believe that the prognosis assessment as detailed in the 2 theories were appreciated in these cases and planning controlled larger studies may help decide their value.
Conclusions
Continuum theory proposes return of high fever as a sure sign of improvement in chronic inflammatory diseases under treatment, as efficient acute inflammation implies improvement in the chronic. In the 6 atopic dermatitis cases presented here, long remission after treatment was associated with return of acute inflammatory diseases/fever, absent since onset of AD. The control cases that did not improve under homeopathic treatment also showed remarkable improvement associated with appearance of fever. This phenomenon needs to be investigated on a large scale to facilitate the development of an objective clinical prognostic tool and immunological research is necessary to understand if efficient acute inflammation and chronic are indeed mutually exclusive.
Acknowledgements
The patients’ willingness to render their cases for medical knowledge is greatly appreciated. The authors wish to acknowledge the help of Aaditi Lakshman, Amritha Belagaje and Pooja Dhamodar in refining the manuscript.
Funding:
The author(s) received no financial support for the research, authorship and/or publication of this article.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Author Contributions
SM, MM, OH, VK, CC and PS were the primary physicians who treated the cases, collected and analysed the data. SM drafted the manuscript and obtained references.
GV is the guide and gurantor of the study.
All authors have made considerable contributions to the paper.
All authors have read and approved the final version of the manuscript.
Consent for Publication
Patients provided written consent for publication.
ORCID iD
Seema Mahesh https://orcid.org/0000-0002-4765-5595
Supplemental Material
Video of Case 5 on a particularly bad night https://figshare.com/s/0d4750675a65ff96cf9e.
References
| 1. | Vithoulkas, G, Carlino, S. The “continuum” of a unified theory of diseases. Med Sci Monit. 2010;16:15. Google Scholar |
| 2. | Brunner, PM, Guttman-Yassky, E, Leung, DY. The immunology of atopic dermatitis and its reversibility with broad-spectrum and targeted therapies. J Allergy Clin Immunol. 2017;139:S65-S76. doi:10.1016/j.jaci.2017.01.011 Google Scholar | Crossref | Medline |
| 3. | Nutten, S. Atopic dermatitis: global epidemiology and risk factors. Ann Nutr Metab. 2015;66:8-16. doi:10.1159/000370220 Google Scholar | Crossref | Medline |
| 4. | Cabanillas, B, Brehler, A-C, Novak, N. Atopic dermatitis phenotypes and the need for personalized medicine. Curr Opin Allergy Clin Immunol. 2017;17:309. Google Scholar | Crossref | Medline |
| 5. | Brunner, PM, Silverberg, JI, Guttman-Yassky, E, et al. Increasing comorbidities suggest that atopic dermatitis is a systemic disorder. J Investig Dermatol. 2017;137:18-25. Google Scholar | Crossref | Medline |
| 6. | Franza, L, Carusi, V, Altamura, S, et al. Interrelationship between inflammatory cytokines (IL-1, IL-6, IL-33, IL-37) and acquired immunity. J Biol Regul Homeost Agents. 2019;33:1321-1326. doi:10.23812/Editorial Google Scholar | Crossref |
| 7. | Gallenga, CE, Pandolfi, F, Caraffa, A, et al. Interleukin-1 family cytokines and mast cells: activation and inhibition. J Biol Regul Homeost Agents. 2019;33:1-6. Google Scholar | Medline |
| 8. | Yang, T-LB, Kim, BS. Pruritus in allergy and immunology. J Allergy Clin Immunol. 2019;144:353-360. doi:10.1016/j.jaci.2019.06.016 Google Scholar | Crossref | Medline |
| 9. | Hahnemann, S . Organon of Medicine. B. Jain Publishers; 2002. Google Scholar |
| 10. | Mahesh, S, Mallappa, M, Tsintzas, D, et al. Homeopathic treatment of vitiligo: a report of fourteen cases. Am J Case Rep. 2017;18:1276-1283. doi:10.12659/ajcr.905340 Google Scholar | Crossref | Medline |
| 11. | Stalder, J, Taieb, A, Atherton, D, et al. Severity scoring of atopic dermatitis: the SCORAD index: consensus report of the European task force on atopic dermatitis. Dermatology. 1993;186:23-31. Google Scholar | Crossref | Medline |
| 12. | Deleuran, M, Vestergaard, C. Clinical heterogeneity and differential diagnosis of atopic dermatitis. Brit J Dermatol. 2014;170:2-6. doi:10.1111/bjd.12933 Google Scholar | Crossref | Medline |
| 13. | Di Benedetto, MG, Bottanelli, C, Cattaneo, A, et al. Nutritional and immunological factors in breast milk: a role in the intergenerational transmission from maternal psychopathology to child development. Brain Behav Immun. 2020;85:57-68. doi:10.1016/j.bbi.2019.05.032 Google Scholar | Crossref | Medline |
| 14. | Kunz, B, Oranje, AP, Labrèze, L, et al. Clinical validation and guidelines for the SCORAD index: consensus report of the European task force on atopic dermatitis. Dermatology. 1997;195:10-19. doi:10.1159/000245677 Google Scholar | Crossref | Medline | ISI |
| 15. | Van Haselen, R . Homeopathic clinical case reports: development of a supplement (HOM-CASE) to the CARE clinical case reporting guideline. Complement Ther Med. 2016;25:78-85. Google Scholar | Crossref | Medline |
| 16. | Vithoulkas, G. Levels of Health. 3rd ed. International Academy of Classical Homeopathy; 2019. Google Scholar |
| 17. | Serhan, CN, Savill, J. Resolution of inflammation: the beginning programs the end. Nat Immunol. 2005;6:1191-1197. doi:10.1038/ni1276 Google Scholar | Crossref | Medline | ISI |
| 18. | Rajakariar, R, Yaqoob, MM, Gilroy, DW. COX-2 in inflammation and resolution. Mol Interv. 2006;6:199. Google Scholar | Crossref | Medline |
| 19. | Sibley, W, Bamford, C, Clark, K. Clinical viral infections and multiple sclerosis. Lancet. 1985;325:1313-1315. Google Scholar | Crossref |
| 20. | Perrotta, F, Corbi, G, Mazzeo, G, et al. COVID-19 and the elderly: insights into pathogenesis and clinical decision-making. Aging Clin Exp Res. 2020;32:1-10. doi:10.1007/s40520-020-01631-y Google Scholar | Crossref | Medline |
| 21. | Wang, B, Li, R, Lu, Z, et al. Does comorbidity increase the risk of patients with COVID-19: evidence from meta-analysis. Aging. 2020;12:6049-6057. doi:10.18632/aging.103000 Google Scholar | Crossref | Medline |
View Abstract
SAGE Recommends
https://journals.sagepub.com/doi/full/10.1177/1179547621994103?fbclid=IwAR0cEcXfaPPqzy1nKE0UtnabQYK8KjitTDY009XFclFUowVjDv3wxwGWHXU#.YCZvIPqOPoU.facebook

