ABSTRACT
Allergic rhinitis is a very common medical problem in the age group 20 to 40 years. The prevalence is 10-20 % worldwide. Allergic rhinitis being a non-fatal condition is often taken for granted but it can cause significant morbidity in this age group. The diagnosis of allergic rhinitis is mainly clinical, so it becomes difficult sometimes to differentiate between allergic and non-allergic rhinitis. The importance of this study is to find the effectiveness of homoeopathic medicines in treatment of allergic rhinitis.
Objectives: The main objectives were to see whether homoeopathic medicines can reduce the intensity of allergic rhinitis and episodes of allergic rhinitis.
Materials and Methods: This was an open level, single arm, experimental, prospective and randomized without control, before and after comparison study done on 30 cases satisfying the case definition and, inclusion and exclusion criteria for a time period of one and half years.
Results: Moderate results were seen after giving homoeopathic treatment as the t-calculated value with level of significance P at a differential field 29 is greater i.e. 9.918, for number of episodes of allergic rhinitis per week after giving homoeopathic medicines than the t- table value with level of significance P = 0.01, i.e. 2.756.
INTRODUCTION
DEFINITION: Allergic rhinitis can be defined as the presence of 2 or more recurrent symptoms of excessive sneezing, watery nasal discharge, nasal congestion, nasal itching, and red itchy eyes for at least one hour on most of the days or on most days of the season if symptoms are seasonal after exposure to certain allergens.9
PREVALENCE: Allergic Rhinitis is a global health problem and is increasing in prevalence. It is 10-20% worldwide and 10-15% in India. The prevalence of allergic rhinitis has increased in last 2-3 decades and it continues to increase. The International Study of Asthma and Allergies in Childhood (ISAAC) noted the prevalence of rhinitis with itchy-watery eyes in six to seven years olds as 0.8 to 14.9 percent and in 13 to14 years’ olds from 1.4 to 39.7 percent in different countries throughout the world.5 In Western countries, between 10 and 30 percent of people are affected in a given year. It is most common between the ages of twenty to forty years.
Allergic rhinitis being a non fatal disease has been considered trivial but it can cause severe morbidity to the sufferers. In infants it may cause feeding difficulties and in childhood it may cause sleep disturbance, lack in daytime concentration, lack in productivity in school, work or sport and social trouble, thus significantly affecting the quality of life.
AETIOLOGY: Allergic rhinitis is an IgE mediated immunologic response of the nasal mucosa to airborne allergens such as pollens, dust, or animal dander. Inhalation of allergens in individual with sensitized immune system produces degranulation of mast cell with the release of chemical mediators. These mediators are responsible for the symptoms of allergic rhinitis. Mainly three types of allergic rhinitis are seen.
- SEASONAL- It includes pollen from grasses, flowers, weeds or trees.
- PERENNIAL- It includes house dust, fungal spores.
- OCCUPATIONAL- It includes animal antigens 4
CLINICAL FEATURES:
- Sudden attack of sneezing
- Profuse watery nasal discharge
- Nasal obstruction
- Associated features:
- Smarting and watering of eyes
- Conjunctival infection with itching1
- Itching of oropharynx 2
- Nasal itching2
INVESTIGATION: Investigations are not always required to confirm diagnosis. However, a confirmation of allergic rhinitis sometimes involves a skin prick test and/or specific and serum total IgE tests. The use of investigations for confirming diagnosis therefore is not an inclusion criterion.
DIAGNOSIS: Accurate history of occurrence coincident with the offending allergens.
PREVENTION: Avoidance of exposure to offending allergens.2
RESEARCH QUESTION:
- Do homoeopathic medicines help to reduce the recurrence of episodes of allergic rhinitis?
- Do homoeopathic medicines help to reduce intensity of symptoms of allergic rhinitis?
NULL HYPOTHESIS:
- There is no significant difference between the number of episodes of allergic rhinitis before and after giving homoeopathic treatment.
- There is no difference between the intensity of symptoms of allergic rhinitis before and after treatment.
BACKGROUND AND JUSTIFICATION:
Allergic rhinitis is very common in our country India. It is also very common in younger age groups especially between 20 to 40 years. It affects a person’s quality of life, financial condition, family and social life and also employment life. Moreover, if not treated properly it may manifest asthma (40% cases).
In Homoeopathy we have many remedies that have specific action on nasal mucous membrane and these remedies can be applied to reduce the acute symptoms of allergic rhinitis. There are deep acting remedies as well, which can be applied constitutionally to reduce the recurrent attacks of allergic rhinitis. Also there are some miasmatic remedies which can be applied as an intercurrent remedy to remove the miasmatic dyscrasia if any. Moreover, as allergic rhinitis is predominantly hereditary in origin so, homoeopathic treatment can reduce the tendency of allergic manifestations in the next generation.
Hence, I have selected this topic to confirm the efficacy of homoeopathic remedies in the treatment of allergic rhinitis.
MATERIALS AND METHODS
Study settings–
Study setup– The study was carried out in Bharati Vidyapeeth Medical Foundation’s Homoeopathic Hospital, OPD, IPD and peripheral OPD.
Case definition– According to ARIA (Allergic Rhinitis and its Impact on Asthma) guidelines allergic rhinitis can be defined as presence of 2 or more recurrent symptoms of excessive sneezing, watery nasal discharge, nasal congestion, nasal itching, red itchy eyes for at least one hour on most of the days or on most days of the season if symptoms are seasonal after exposure to certain allergens. Cases fulfilling this definition in the age group of 20-40 years were taken.9
Inclusion criteria –
- All the patients fulfilling the case definition.
- Patients between 20 years to 40 years were taken.
- Patients who are willing to join research and co-operate with regular follow-ups after willingly signing the consent form for participation in research project about which the details are explained to the patient.
Exclusion criteria –
- Patients with severe epistaxis, sinusitis, asthma and other systemic diseases were not taken.
- Cases not fulfilling the case definition.
- Patients below 20 years and above 40 years were not taken
Diagnostic criteria –
- Diagnosis was done on clinical basis.
- Frequency of episodes of sneezing and rhinorrhoea on exposure to particular allergen.
Study design – An open level, single arm, experimental, prospective, randomized without control, before and after comparison study was done on minimum 30 cases satisfying the case definition and, inclusion and exclusion criteria for a time period of 1 and half years.
Sampling procedure – Patients diagnosed with allergic rhinitis was selected for the study by simple random technique.
Selection of remedy – After detailed homoeopathic case taking and physical examination, individualizing totality was formed and the selection of remedy was done according to symptom similarity based on homoeopathic principles.
Dose and strength of drug – Potency in centesimal scale was used as per requirements of the patient on the basis of following criteria: 3
- HIGH POTENCY –
- a) Greater the similarity of symptoms
- b) Predominant mental symptoms in a case.
- c) Cases no longer responding to lower potency, with same indication.
- d) Intercurrent remedy was prescribed in higher potency.
- MEDIUM POTENCY – If any doubt about accuracy of the prescription or about the probability of an aggravation.
- LOW POTENCY – Cases in which mental and physical generals are less.
Drug administration – This was done through oral route.
Drug dispensing – Was done in globules, powder and liquid form.
Clinical protocol –
- Ethical Committee approval was availed.
- Data was collected by proper method and was processed in standard format with following aspect –
- Patient was selected on the basis of case definition, inclusion and exclusion criteria.
- Details of the study work were explained to the patient and their consent was taken separately.
- Detailed case taking was done according to the standard homoeopathic case Performa.
- Totality of case was formed and individualization was done according to the homoeopathic principles.
- Repertorization of each and every case was done.
- After Repertorization the most simillimum remedy was selected.
- Total dissertation was submitted to ethical committee.
Criteria for follow up – All the patients were duly followed and details of the symptomatic and clinical changes were recorded with following criteria:
- Follow -up was taken in every 15 days.
Standard follow –up Performa was prepared.
Data collectionwas done according to standardized homoeopathic case Performa and was thoroughly maintained.
Criteria for assessment – This was done on the basis of following symptoms:
- Frequency of sneezing
- Nasal discharge
- Nasal blockage
- Associated symptoms like lachrymation, conjunctival, nasal or oropharyngeal itching
- Number of episodes per week
- Good –if all the symptoms get reduced in 3 weeks and no recurrence in 3 months.
- Moderate –if all the symptoms get reduced in 3weeks and recurrence within 3 months.
- Poor –if all the symptoms get reduced in more than 3 weeks and much recurrence within 3 months.
OBSERVATIONS:
In this study 37 patients were enrolled, among which 32 fulfilled the case definition, 5 cases were drop out. Total 30 cases were included in final analysis.
- SEX DISTRIBUTION
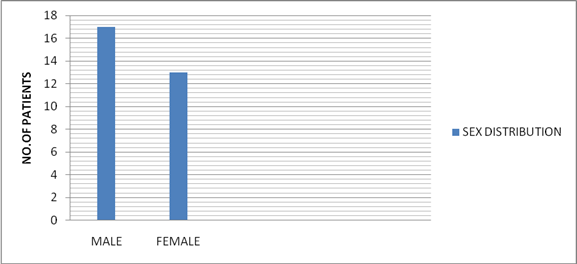
Bar diagram no. 1- sex distribution
- AGE DISTRIBUTION
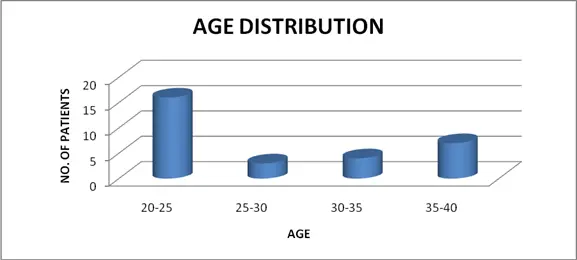
Bar diagram no. 2- age distribution
- COMMON TRIGGERING FACTORS
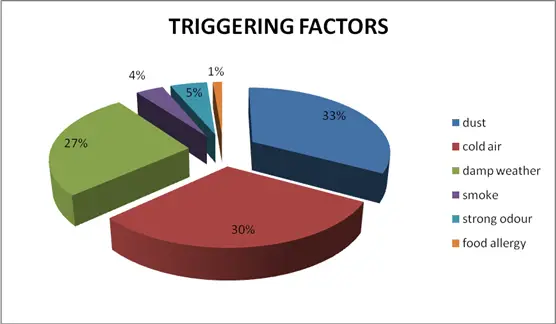
Pie diagram no. 1- triggering factors
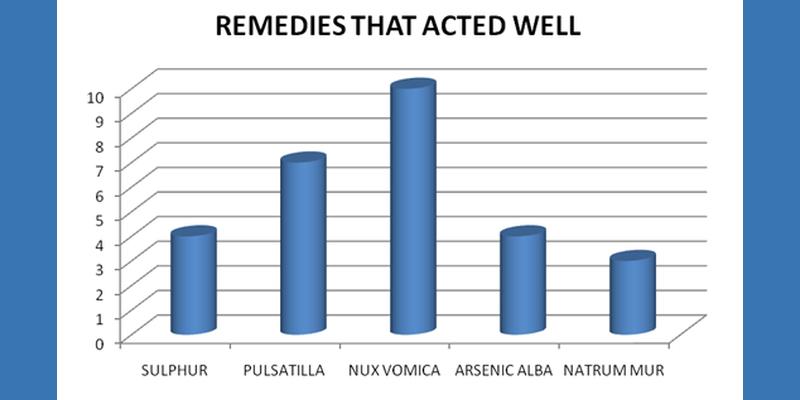
- REMEDIES THAT ACTED WELL
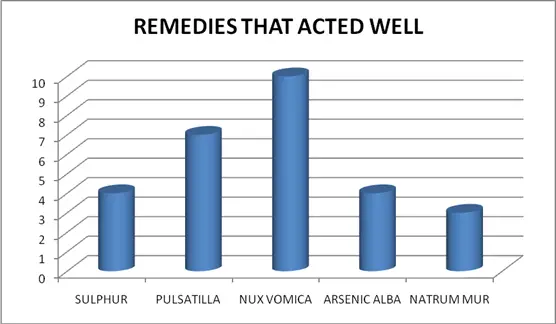
Bar diagram no.4- remedies that acted well
As the number of sample size is 30 so t-test was done to see the difference between episodes of allergic rhinitis before treatment and after treatment
| Serial no. | Case no. of patients | No. of episodes in 1 week before treatment(X1) | No. of episodes in 1 week after treatment(Y1) | D= (X1-Y1) |
| 1 | P-2268 | 4 | 0 | 4 |
| 2 | K-2760 | 5 | 3 | 2 |
| 3 | K-2464 | 4 | 1 | 3 |
| 4 | N-709 | 5 | 3 | 2 |
| 5 | P-2191 | 5 | 1 | 4 |
| 6 | K-2536 | 7 | 0 | 7 |
| 7 | M-1599 | 6 | 2 | 4 |
| 8 | P-2174 | 5 | 1 | 4 |
| 9 | G-1484 | 7 | 3 | 4 |
| 10 | R-755 | 2 | 0 | 2 |
| 11 | S-3653 | 7 | 2 | 5 |
| 12 | R-655 | 7 | 2 | 5 |
| 13 | R-706 | 5 | 2 | 3 |
| 14 | H-252 | 6 | 0 | 6 |
| 15 | J-1479 | 3 | 3 | 0 |
| 16 | H-229 | 7 | 3 | 4 |
| 17 | H-238 | 7 | 2 | 5 |
| 18 | YR-195 | 3 | 0 | 3 |
| 19 | K-2487 | 4 | 1 | 3 |
| 20 | K-2752 | 5 | 2 | 3 |
| 21 | H-231 | 4 | 1 | 3 |
| 22 | B-1502 | 4 | 0 | 4 |
| 23 | N-710 | 6 | 1 | 5 |
| 24 | K-2480 | 3 | 0 | 3 |
| 25 | YR-147 | 4 | 2 | 2 |
| 26 | YR-142 | 4 | 0 | 4 |
| 27 | R-707 | 6 | 2 | 4 |
| 28 | YR-207 | 5 | 0 | 5 |
| 29 | FC-1190 | 6 | 0 | 6 |
| 30 | I-119 | 7 | 7 | 0 |
| ∑D=109 |
Here, X1= number of episodes of allergic rhinitis/week before treatment
Y1= number of episodes of allergic rhinitis/week after treatment
Null hypothesis (Ho) X1=Y1
Alternative hypothesis (H1) X1≠Y1
Level of significance P = 0.01 or 0.05 at degree of freedom (n-1) = 29
ttable at P value 0.01 is 2.756 and at P value 0.05 is 2.045
d = ∑D/n = 109/30 = 3.63
d is the mean difference between x and y
Now, ∑ (D- d)2= 117
SD = √∑ (D-d)2/n-1 = √117/30-1 = √4.034 = 2.008
SE = SD/√n = 2.008/√30 = 0.366
tcal = d/SE = 3.63/0.366 = 9.918
tcal is greater than t table, so, null hypothesis is rejected
RESULTS: After applying t-test it is seen that there is a significant difference between the number of episodes of allergic rhinitis per week before treatment and after treatment. So, it is clear that homoeopathic medicines are effective in reducing the number of episodes of allergic rhinitis.
It is also seen throughout the study that homoeopathic medicines not only help to reduce the episodes of rhinitis but are also capable of reducing the intensity of symptoms, such as number of sneezing at a time, nasal discharge, nose blockage, eye symptoms etc.
Considering the criteria of assessment good response was seen in 6 cases, moderate response in 14 cases and poor response in 10 cases.
DISCUSSION:
Allergic rhinitis was predominantly noted among males in my study. 26 cases were taken from Bharati Vidyapeeth Homoeopathic Hospital OPD and 4 cases were taken from peripheral OPD at Yawat. As my study was done on patients between 20 to 40 years so most patients were found less than 30 years.
Recurrent sneezing was the most common symptom found in all cases. My criteria of assessment were to observe the changes in symptoms of allergic rhinitis for at least 3 months after giving homoeopathic treatment in each case. Only the observations found in 5 follow up after giving medicines were studied, every follow up being taken at around 15 days.
Homoeopathic medicines were found to be effective in almost all cases though in a few cases severe aggravations were seen. The most frequently indicated medicines were Nux vomica, Pulsatilla, Sulphur, Arsenicum album, Sepia, Nat mur. Best results were seen with Nux vomica and Pulsatilla. Sabadilla I prescribed in 3 cases but results were not satisfactory, though Sabadilla is one of the most preferred remedies for allergic rhinitis.
In a study done by Dr Vatsana Kasana and Dr K. C. Bhinda in Jaipur, they found Psora as the most common miasm behind allergic rhinitis. But in my study, the Tubercular miasm was found in the background in most of the cases (17 cases), while Psora exhibited in 10 cases, Sycosis in one case and Psora-Sycosis in 2 cases. Tuberculinum, Psorinum, Sulphur and Thuja were prescribed as intercurrent remedies to remove the miasmatic dyscrasias. With Tuberculinum 1M, symptoms were better with less recurrence of episodes of allergic rhinitis in 16 cases. In 2 cases, Psorinum 1M was prescribed with very severe aggravation. Sulphur was prescribed in 2 cases as an intercurrent remedy with excellent results. Also, Sulphur was found to be very effective in reducing acute symptoms of allergic rhinitis if prescribed on symptom similarity.
Sepia, Calc carb and Natrum mur showed good results in 3 cases when prescribed constitutionally. Belladonna, Rhus tox and Arsenicum album were found to be more effective in reducing the associated symptoms, like redness of eyes, lachrymation, nasal and oropharyngeal itching respectively.
The 200 potency was found to be more effective in most cases, though 30c and 1M were also prescribed with satisfactory results. In only a few cases was repetition needed in acute onset, otherwise single dose, single remedy showed brilliant results.
Along with the medication, steam inhalation and avoidance of allergens during treatment were found very helpful. 12 patients could stop allopathic medicines totally during and after treatment with Homoeopathy.
CONCLUSION:
- This research concludes that homoeopathic remedies are effective in treatment of allergic rhinitis, especially in reducing the number of sneezes and also in reducing the number of episodes of allergic rhinitis.
- This research shows the effectiveness of Nux vomica and Pulsatilla in treatment of allergic rhinitis especially where sneezing with nasal blockage due to hypertrophy of nasal mucosa was found.
- Pulsatilla was found to be the most valuable remedy in cases with thick nasal discharge.
- Specific remedies like Lemna minor and Teucrium M V were used in a few cases with nasal polyp.
- Miasmatic remedies, especially Tuberculinum, were helpful to reduce the recurrence.
- Psorinum should be prescribed with caution as it may aggravate the symptoms undesirably.
- My study contributes to the existing knowledge in the homoeopathic treatment, as it sheds some light on the most effective remedies for allergic rhinitis.
- Further study is needed to know whether allergic rhinitis could be cured completely or not with homoeopathic remedies.
- As my study period was just one and half years, it was a limitation for cases with seasonal allergic rhinitis, as at least 2 years is needed to see the recurrence.
- Also my study was mainly concerned only with perennial allergic rhinitis, so further research is suggested for seasonal allergic rhinitis to see the effectiveness of homoeopathic remedies in its treatment.
SUMMARY:
Allergic rhinitis cases are increasing day by day specially in younger age groups between 20-40 years. Though many researches in allergic rhinitis have already been done in modern medicine, no permanent cure has been seen so far. Homoeopathy being one of the most effective lines of treatment in removing allergic tendencies, it can be helpful in treating allergic rhinitis as well. The aim of this dissertation was to see the effectiveness of homoeopathic medicines in the treatment of allergic rhinitis in the age group 20 to 40 years. The study was carried out in Bharati Vidyapeeth Medical Foundation’s Homoeopathic Hospital, OPD, IPD and its peripheral OPD at Yawat. An open level, single arm, experimental, prospective, randomized without control, before and after comparison study was done on 30 cases for a time period of 1 and half years. The statistical analysis shows positive results after applying t- test in the no. of episodes per week of allergic rhinitis before and after homoeopathic treatment. Overall good response was seen in 6 cases, moderate response in 14 cases and poor response in 10 cases. Intercurrent remedies were found very helpful in reducing the recurrences. Nux vomica and Pulsatilla were found to be the most effective remedies in acute episodes of allergic rhinitis.
BIBLIOGRAPHY/REFERENCES:
- Davidson’s principles and practice of medicine –by Davidson 20th edition ( Page no. 721-722)
- Harrison’s principles of internal medicine- 19th edition(pages 2121- 2122)
- Principles and practice of Homoeopathy – by Dr. M. L. Dhawalen. API textbook of medicine 8th edition ( page no. 353-354)
- Scott-Brown’s Otorhinolaryngology 7th edition,volume-2 (page no.138)
- Diseases of ear nose and throat by Dr. PL Dhingra & ShrutiDhingra
- Miasmatic prescribing 2nd extended edition-by Dr. S. K. Banerjea (page no.77, 79)
- Lectures on Homoeopathic Philosophy-by Dr. J.T. Kent(page no.180)
- Brozek JL, Bousquet J, Baena-Cagnani CE et al. Allergic Rhinitis and its Impact on Asthma (ARIA) guidelines: 2010 revision. J Allergy Clinical Immunology. 2010 Sep 126(3) page 466-476.
- KushalBenerjee, CeireCostelloe, Robert T. Mathie and Jeremy Howick, 10 June 2014 BioMed Central journal.
- DrVatsanaKasana&Dr K. C. BhindaInternational Organisation of Scientific Research Journal Jan-Feb 2016 Volume 11, Issue 1 Ver. IV ( page no.08-13).
- EdzardErnst Focus on Complementary and Alternative Therapy.20 September 2011 volume 16 ( page no 200 -203.)
- ncbi.nlm.nih.gov
- hpathy.com


Really great post.I enjoy to reading this article.There is such a true article there is more information for us .thanks for sharing this lovely post.
Thank you sir
beautiful and scientific article excellent presentation.
My wife is having blocked nose for the last 50 yeas and is sing Otrivine nasal drops every 4 hours. Dr.Rukia do yu think Nux vomica and Pulsatilla will help her.
I want her nose to open and want her to be off otrivine.
Please advise. Afte reading your paper I am sure you can help her.
I am Anaesthesiologist working in teaching hospital in Jeddah.
Wish you a bright career and health and happiness.
My e mail is [email protected]
If you do private consultation please let me know how can I contact you.
Please reply on my e mail.
THANKS.
Dr.Syed Murtaza
Thank you. I do consult online.