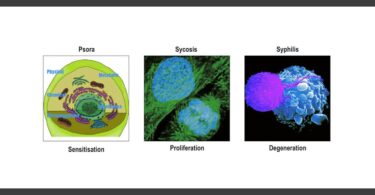
With Aphorism 79, Hahnemann introduces his miasmatic observations on chronic disease known familiarly as the Theory of Miasms from in The Chronic Diseases. Interesting to note is his flow of thought and his plan of presentation here, which is different to that of the Chronic Diseases.
Hitherto syphilis alone has been to some extent known as such a chronic miasmatic disease, which when uncured ceases only with the termination of life.
Aware that for most of the medical men in his time, Syphilis and its various stages of development was an already observed and accepted phenomenon, Hahnemann begins with what is familiar. The concept of chronic disease and its uncontrollable progress was already understood in terms of Syphilis, which meant contracting a condition of lifelong progressive disease, terminating in death. This was the background he wanted his Theory of Miasms to be placed in. The difference was that this now needed to be understood and perceived in terms of a symptom expression of the vital force that progressively deteriorates throughout life under the influence of a fundamental miasm [Aph 5] terminating in death. This could easily be perceived by traditionalist classical homeopaths who eventually adopted and clinically applied the miasm theory very successfully (Miasms-II) over the last 100 years as EVOLUTION OF DISEASE. This also suggests that there were those (famous homeopaths) who did not easily understand it and criticized it finding it difficult to apply it clinically.
It is well known that Syphilis progresses in stages beginning with the external symptom of the chancre and bubo, followed by a latent period, on toward secondary manifestations that include venereal condylomata, copper colored skin eruptions, urethral symptoms, and finally terminating in disease of the nervous system with a diagnosis of ‘general paralysis of the insane’. I wrote a series of articles a couple of years back where this evolution of miasmatic disease has been explained (Miasms-II). Based on the pathological evolution of the Syphilitic infection with Treponema Pallidum, we can grasp the brilliance of this observation by Hahanemann and the perception of the vital force being progressively disturbed toward deeper destruction.
I caution here, there are two aspects to the miasm theory to be aware of, (like two sides of the same coin) that seem to have confused those who choose to restrict their view to one side or the other. One is the miasma (Miasm I), the external agent that is causative in producing a particular miasmatic expression. In general Hahnemann considered Itch/Psora to be typical of scabies, but he also considered leprosy, etc to have a similar expression; Gonorrhea to be typical of Sycosis, but he also considered, as we understand today, the expression of Human Pappiloma Virus (HPV) and the secondary infection of syphilis (venereal condylomata) to be sycotic in expression; and Syphilis to be typical of Syphilitic miasm. JF Allen supported the addition of the Tubercular miasm that is understood a combination of Pora and Syphilis (also perceived by Hahnemann, see Miasm I) both acting in combination where Tuberculosis is a typical expression.
Concentrating only on this aspect of a responsible causative organism (miasma) is only one side of the miasm theory. One would be misguided to believe that if these infections don’t exist, then the miasm does not either. At an extreme are those who wish to produce a miasm for every type of infecting organism without proper investigation as to what the pathological evolutionary development of that infection is over a lifetime. This leaves us with a confusion that requires two pages of explanation to sort out.
The other side of the coin is the ability to recognize miasmatic expression in terms of a totality, i.e. a picture of symptoms representing the miasmatic totality. Every individual expresses a completely different combination of miasmatic symptoms based on their past history or family history. Miasmatic treatment is tackled in an individual manner, as much as any individual chronic case is. The miasmatic picture is however not divorced from the fact that at some point in the patient’s history he may have acquired (by infection) a miasmatic expression or that he harbours an inherited diathesis towards a particular miasmatic expression.
Cancer or the Cancer miasm first propounded by Burnett, can be understood as an expression of combined miasms, depending on the pathology of the symptom expression. There is no causative miasma attributable, which does not qualify it to be a primary miasm, but rather, a secondary miasm like Tubercle observed due to a typical picture rather than a specific miasma. We will discuss this more at an appropriate place.
Sycosis (the condylomatous disease),…
The quality of Sycosis is the condylomata, the excessive growth of unwanted/non-malignant tissue. Hahnemann made a mistake of pathological observation when he suggested that this was due to gonorrhea. In actuality, this is either due to HPV, or is an expression of Syphilis in the secondary stage. The point to be borne in mind though, is that the expression of Sycosis is an overgrowth of cells and tissues, increased discharges especially abnormal ones with typical staining and color, a slowing of metabolism, and various other manifestations as we understand it today. Hahnemann’s mistake has inadvertently confirmed that miasmatic expression is not solely the domain of an infecting miasma, but requires the other side of the coin, the symptomatic expression.
equally ineradicable by the vital force without proper medicinal treatment,
The treatment that Hahnemann refers to here, is the DYNAMIC chronic remedy supported by the appropriate miasmatic remedy. Antibiotics, so effective nowadays that seem almost magical cure to these dreaded diseases, do only half the work. They deal with the PHYSICAL expression of disease, but they have NO effect on the DYNAMIC effect of disease which continues to persist, progress and is passed down through the generations in genetic mutations, weaknesses and diathesis.
was not recognized as a chronic miasmatic disease of a peculiar character, which it nevertheless undoubtedly is,
Here Hahnemann refers to condylomata being part of a chronic disease, and not a local expression of disease. He explains this short-sightedness of mistaking constitutional (progressive) disease as a local disease more in detail in aphorism 185-190. He uses the terms more precisely in these aphorisms based on his homeopathic philosophy and classification of disease expression.
and physicians imagined they had cured it when they had destroyed the growths upon the skin, but the persisting dyscrasia occasioned by it escaped their observation.
Physicians in his time failed to observe the difference between local disease and chronic disease, because the philosophical understanding of disease did not exist. The reason why these external growths (like warts and condylomata, etc) are not local diseases is because the entire organism (through the vital force) is involved in its expression [Aph 189]. The reason for this involvement is a peculiar ‘dyscrasia’ that the vital force either acquires or inherits that needs the appropriately timed anti-miasamtic DYNAMIC remedy for cure. This can begin right from childhood when cells are still developing, and genetic problems can be corrected more easily. If uncured they will present themselves again at an older age with much less chance of cure. Early treatment would result in a longer lifespan, less troubled by advancing disease expression fueled by miasmatic daithesis; and a corrected genetic weakness that would hence NOT be passed to the next generation.
BIBLIOGRAPHY
1. Hahnemann, Samuel C, MD: (1896) The Chronic Diseases, Volume 1; Translation by Tafel, LH; BJain Publishers.
2. Hahnemann, Samuel C, MD: (1921) Organon of Medicine, 6th Edition; Translated by William Boericke, MD, BJain Publishers Ltd, Reprint edition 1986.
3. Allen, JH, MD; (1908) The Chronic Miasms – Volume I and II; B. Jain Publishers, India.
4. Boenninghausen, C von ;(1846) Boenninghausen’s Therapeutic Pocket Book, Part 1: Preface; 5th American Edition by Dr. T. F Allen
5. Boger, Dr. CM, MD; (1915) A Synoptic Key of the Materia Medica; Foreword, 5th Edition: B. Jain Publishers, India.
6. Boger, Dr. CM, MD; (1964) Studies in the Philosophy of Healing: 2nd Edition; B. Jain Publishers, India.
7. Das, Ashok Kumar: Treatise on the Organon of Medicine, B.Jain Publishers
8. Dhawle, ML (2003); ICR Symposium Volumes I,II,III; 2003 Edition
9. D’Souza, L (2006): Miasms in Case Management, Part 2: Disease Evolution and its Miasmatic Management, 3rd edition, 2006; URL: https://hpathy.com/organon-philosophy/miasms-in-case-management-ii/
Last accessed Sept 2007
10. Kent, James T, MD ; (1926) Lesser Writings – Part II; Editor W.W. Sherwood, p. 292-310; B. Jain Publishers, India, Reprint edition 1997
11. Kent, James T, MD; (1900) Lectures on Homeopathic Philosophy, B. Jain Publishers, India
12. Dudgeon RE, Boericke William; Organon of Medicine by Samuel Hahnemann, Fifth and Sixth Edition Combined.
13. Vijayakar, Dr. Prafull, LCEH; (2003), The End of Myasumption of Miasms
14. Banerjea, SK: Miasmatic Diagnosis (Notes from seminars).
15. Little, David: Case Management available on www.simillimum.com
at gement/aicr/article.php
Last accessed June 2007